On July 14, 2026 the FDA approved Revtorpyk (gedatolisib) + fulvestrant, with or without palbociclib, for HR+/HER2−, PIK3CA wild-type advanced breast cancer after prior endocrine therapy — the first pan-PI3K/AKT/mTOR pathway inhibitor for this population. Basis: the Phase III VIKTORIA-1 trial (Celcuity, $CELC).
Explore Trial Data
Gedatolisib is now @US_FDA ✅ based off VIKTORIA-1: PhIII, Gedato (PI3K/mTORi) + Fulv +/- Palbo vs. Fulv in HR+ after one line of ET in HR+ - mPFS: 9.3mos w/triplet vs. single agent Fulv (HR: 0.24) - mPFS: 7.4mos w/doublet vs. single agent Fulv (HR: 0.33) - AEs (IV/⏰ https://t.co/VdkLGBgPu2
This is for PIK3CA-WT. Comparing triplet (Arm A) and doublet (Arm B) to single agent Fulvestrant (Arm C) (rather than this being compared to Alpelisib + Fulv). Thanks for pointing this out @dr_yakupergun 🙏🏽🙏🏽

The @FDA approves gedatolisib as 2nd line therapy in combo with fulvestrant in tumors w/o PIK3CA mutations. Median PFS F, 2.0m, F+G, 7.4m, F+G+palbo 9.3m. https://t.co/VPzVX3Wglb

FDA approves gedatolisib in combination with fulvestrant, with or without palbociclib, for adults with HR+/HER2-locally advanced or metastatic breast cancer without a PIK3CA mutation detected following progression on or after treatment with at least one line of endocrine therapy

FDA approved gedatolisib (Revtorpyk) + fulvestrant ± palbociclib for HR+/HER2−, PIK3CA wild-type advanced/metastatic breast cancer after progression on endocrine therapy. @Larvol @OncoAlert https://t.co/N9n8lbH21I
Treatment algorithm in outline for ER+ MBC: Column A: endocrine agent (fulvestrant, oSERD, AI, tamoxifen) Column B: targeted agent (CDK46i, PIK3CAi) Choose one from column A and one from column B. Repeat with each line of treatment.
Design — Phase 3; gedatolisib (Revtorpyk) + fulvestrant, with or without palbociclib; Study 1 = PIK3CA wild-type vs single-agent fulvestrant (NCT05501886, n=392). (FDA label)
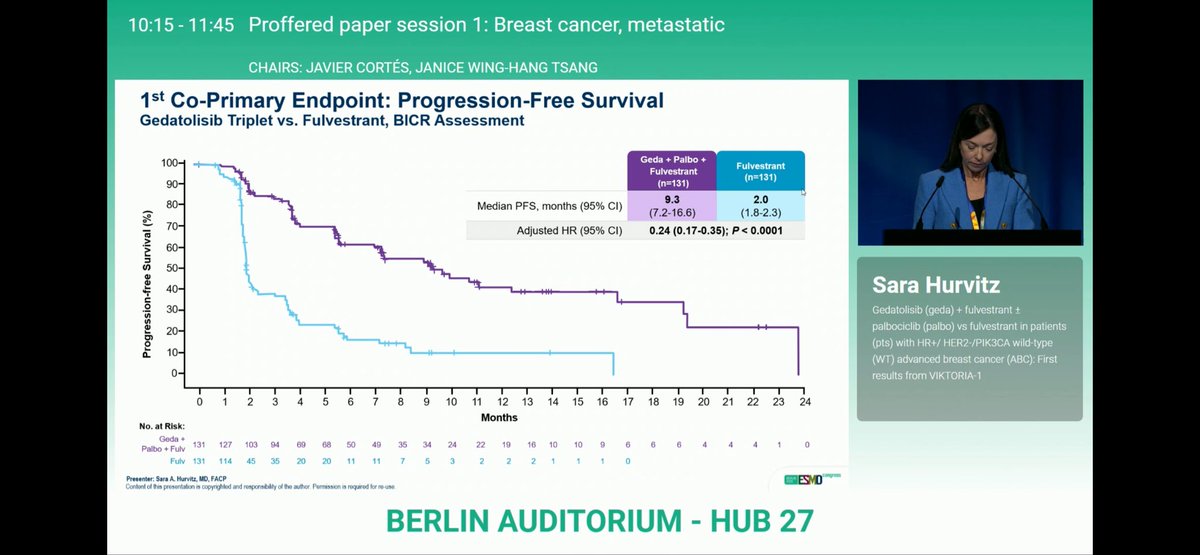
PFS (Study 1, wild-type) — Triplet 9.3 mo (95% CI 7.2-16.6) vs 2.0 mo, HR 0.24, p<0.0001; doublet 7.4 mo (5.5-9.9), HR 0.33, p<0.0001. (FDA label)
ORR — 32% (triplet) / 28% (doublet) / 1% (fulvestrant). (FDA label)
Regulatory — FDA approved Jul 14, 2026 for HR+/HER2- PIK3CA wild-type only; the PIK3CA-mutant cohort (Study 2) is NOT part of the approval. (FDA.gov)
Sponsor / Drug — Celcuity; gedatolisib, a pan-PI3K/AKT/mTOR inhibitor, 180 mg IV weekly on Days 1/8/15 of each 28-day cycle. (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 20, 2026.





Create a free account, pick the tumor types you cover, and go beyond the tweet — the intelligence pharma teams use to map influence and prepare for engagement:










May 1, 2026 — Celcuity ($CELC) announced that the Phase 3 VIKTORIA-1 trial achieved its primary endpoint in the PIK3CA-mutant cohort, joining the previously-reported positive PIK3CA-wild-type readout. Both gedatolisib triplet and doublet improved PFS vs the alpelisib + fulvestrant active comparator. Full data at ASCO 2026 (May 29–Jun 2).
Threads ranked by total KOL discussant count (replies + quote-tweets). Each main tweet shows the actual oncology KOL discussants — both replies (green) and quote-tweets (blue). Wall Street, stock-promo, WhatsApp-spam, analyst price-target tweets, and emoji-only replies all excluded.

BREAKING: positive results from the VIKTORIA-1 PIK3CA-mutant cohort Both the gedatolisib triplet and doublet improved PFS vs fulv/alpelisib, positioning gedatolisib as an active option irrespective of PIK3CA status. Key caveat: the weekly IV formulation. https://t.co/ZclPhQmcWl

The only agent with positive data in wild type and mutant BC since everolimus! Caveats as noted. IV 3 out of 4 weeks and stomatitis. @OncoAlert https://t.co/09ilVZ0pHG

We already knew the positive results in the PIK3CA-wild population. Seeing positive results in the mutant group as well is encouraging. The main drawback of the combination, however, is its parenteral administration: ➡

The incredible negative impact on LIVING while being tied to an infusion chair 3 weeks out of 4 means there has got to be way more than a statistically significant ⬆️ in PFS (which could be a month or so) - it better hav
Top 10 by impressions - click to view on X
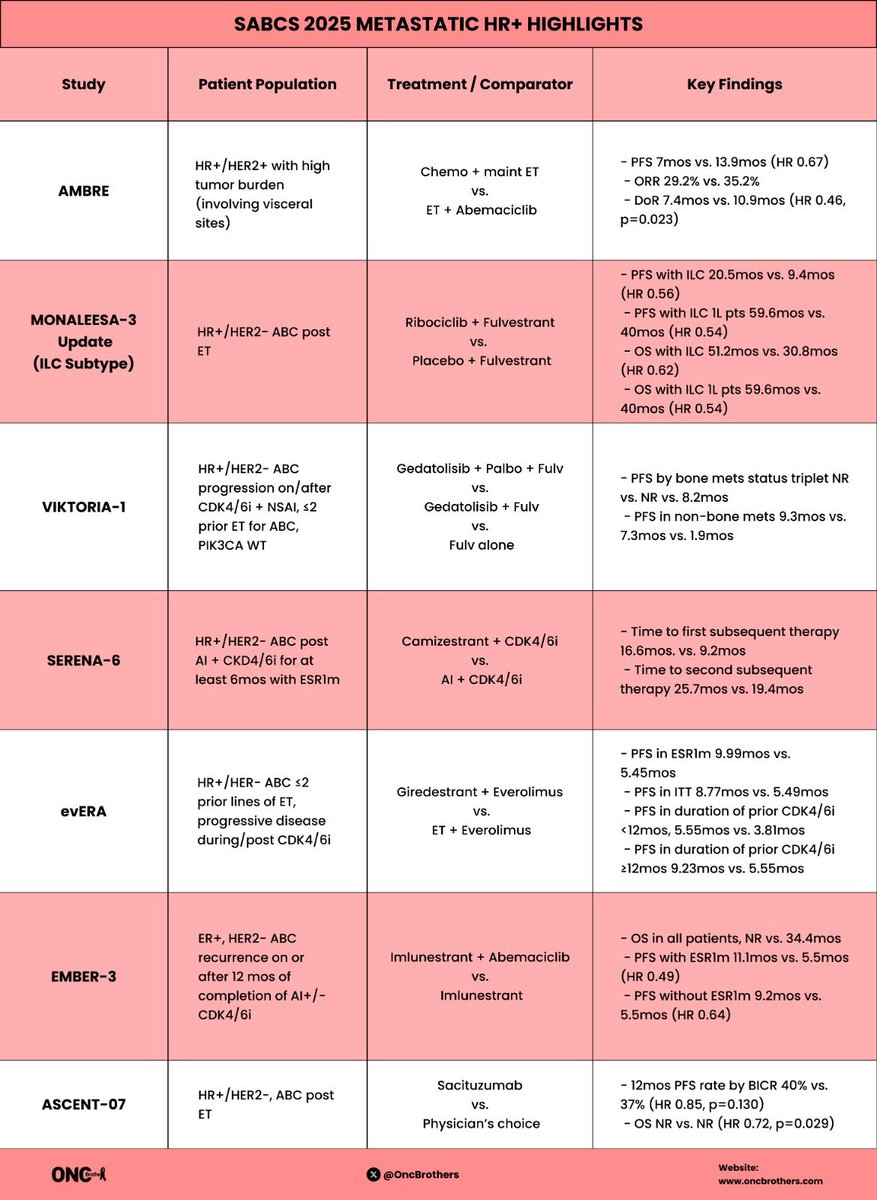
A lot was covered but summary of 7 main studies we touched on during Metastatic HR+ #BreastCancer #SABCS highlights w/ @hoperugo: ✅...
Metastatic HR+ #BreastCancer #SABCS highlights w/ @hoperugo: ✅ #AMBRE ✅ #MONALEESA ✅ #VIKTORIA1 ✅...
Excellent question from the audience. Why in the world are we still using single agent fulvestrant control arms in 2025? Apparently @US_FDA mandated this in Viktoria 1.
#VIKTORIA1: combos of gedatolisib (multi target inhibitor of PI3 and mTOR 1/2) in PI3 wt post CDK 4/6 ER+ #bcsm PFS Fulv - 2.0 mo Fulv/ged - 7.4 mo Fulv/palbo/ged...
Fantastic discussion at #ESMO25 by super @ALEDIGNUS12 on the complicated choices for second-line endocrine-based therapy in patients with advanced HR+/HER2-...
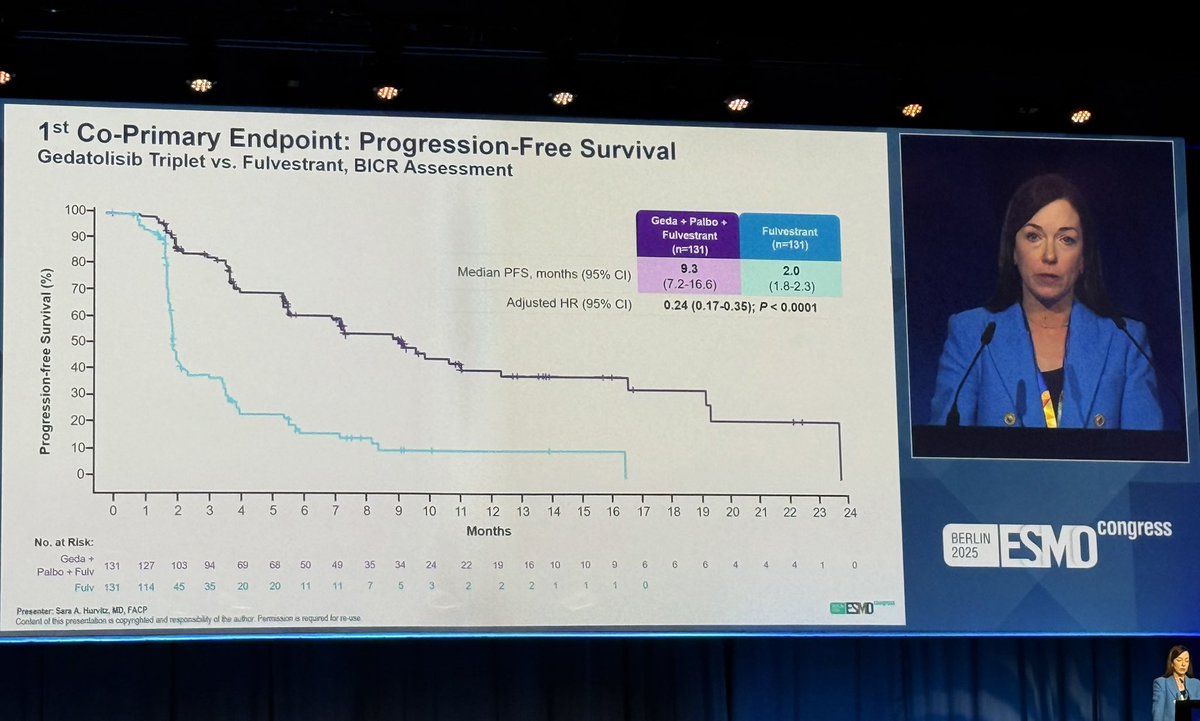
VIKTORIA-1: major improvement in PFS (9.3 vs 2 months, HR 0.24, p<0.001) with gedatolisib/palbo/fulvestrant vs fulvestrant as 2L after CDK4/6i for PIK3CAwt disease. Moderate toxicity, with 2...
#SABCS25 Day 3 Highlights: 1. #AMBRE: 1L in high tumor burden HR+ mBC 2. #VIKTORIA1: 2L after ET/CDK 4-6i in HR+ mBC 3....
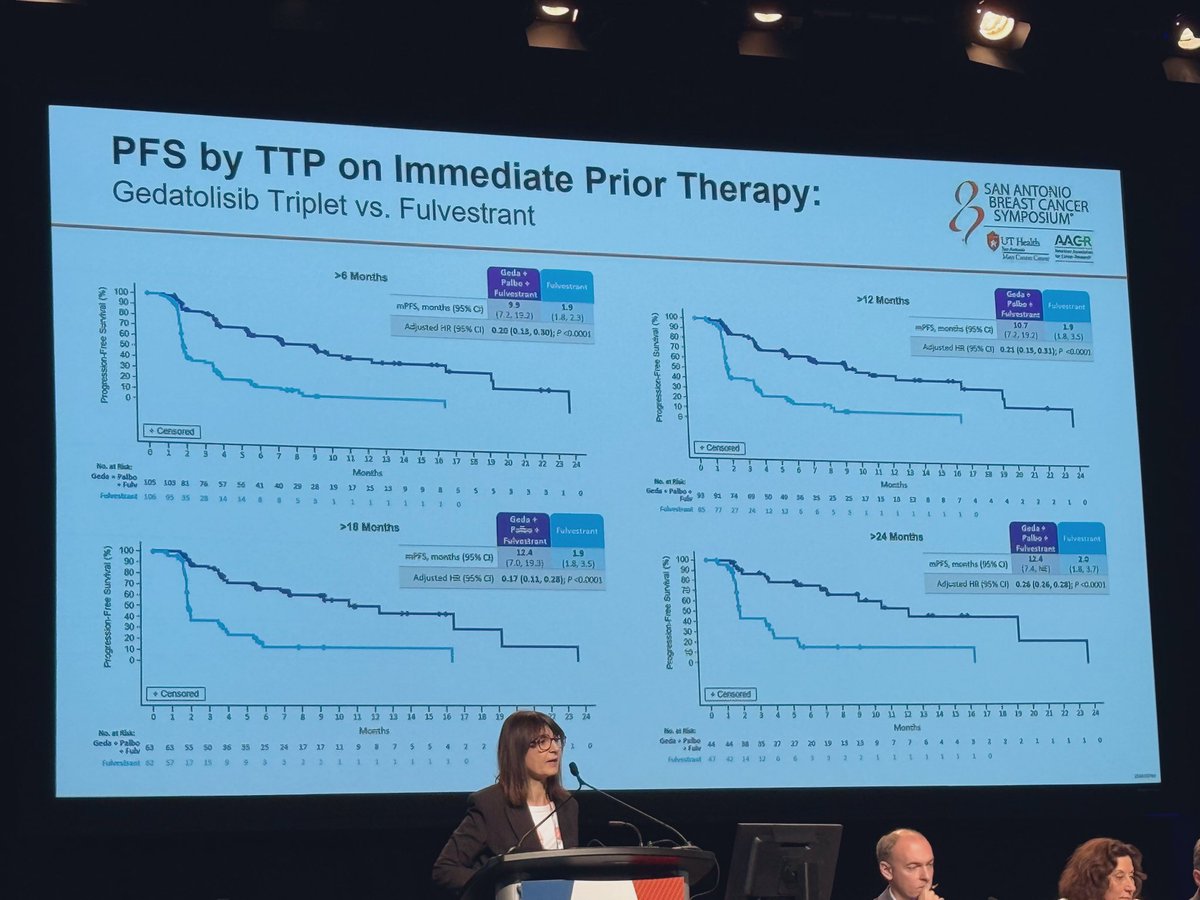
Benefit of gedatolisib in the VIKTORIA-1 trial was seen irrespective of duration of the immediate prior therapy. @BarbaraPistill2 #SABCS25
#ESMO25 Sara Hurvitz presented the fascinating and important data from Victoria-1. The PIK3CA/mTOR IV inhibitor gedatolisib markedly increased PFS with palbo (and without) comp to...
4. #VIKTROIA1: PhIII, Gedatolisib (IV, PI3K/mTORi) + Fulv +/- Palbo vs. Fulv in HR+ after CdK4/6i - mPFS 9.3mos vs. 2.0mos triplet vs. Fulvestrant in WT (Fulv alone is not what we...
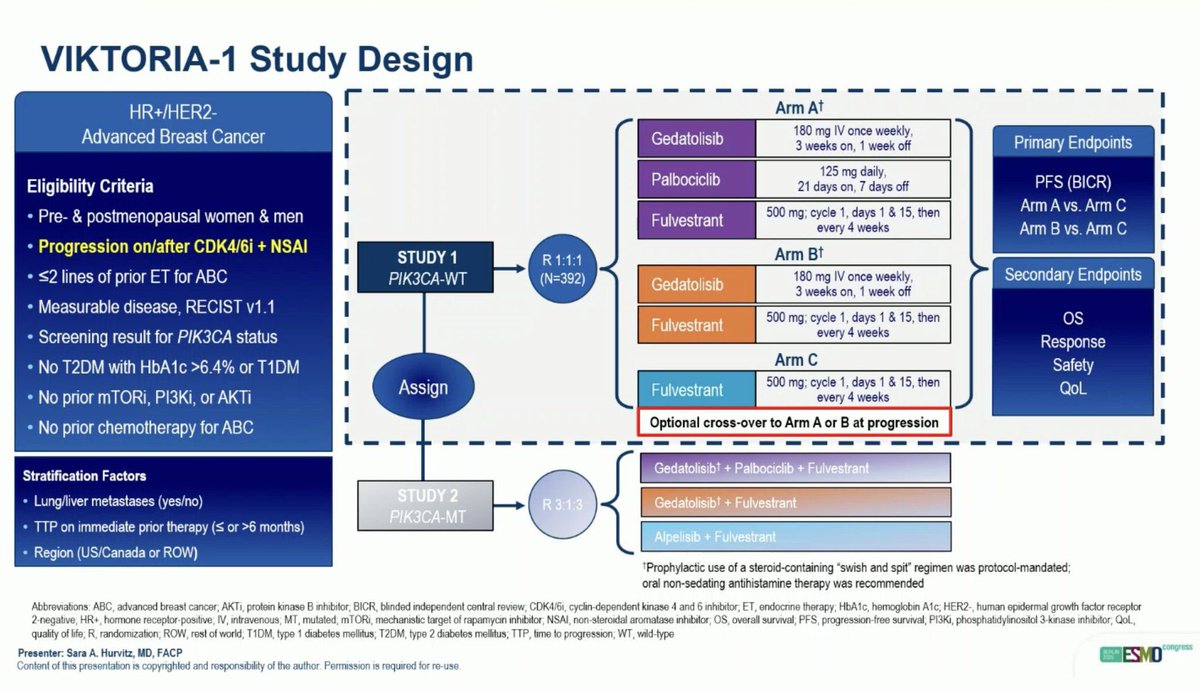
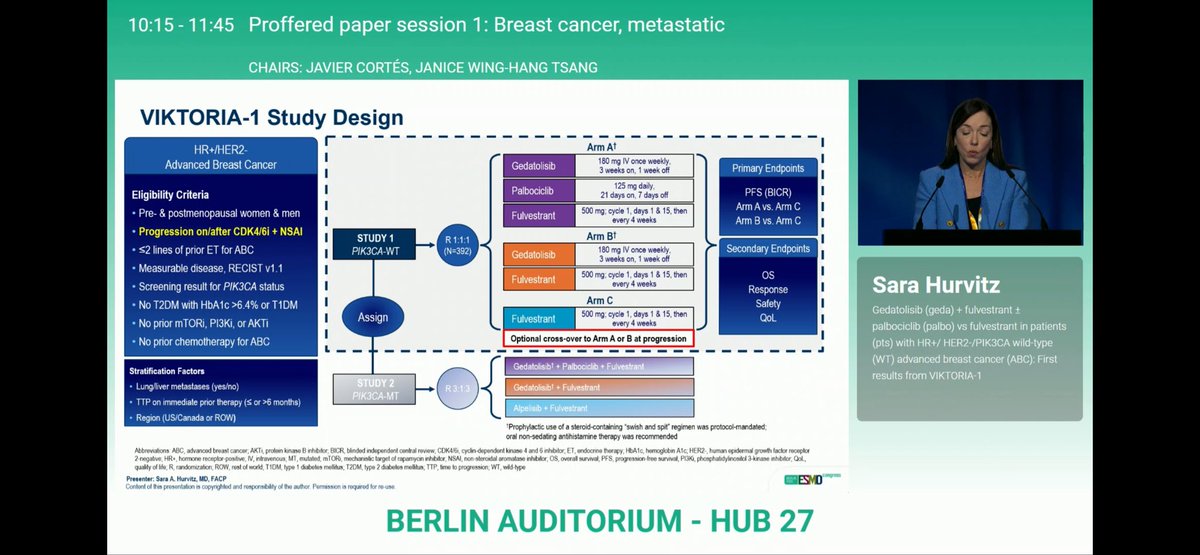
VIKTORIA-1 is a Phase III, open-label, randomized trial evaluating gedatolisib — now FDA-approved as Revtorpyk — a pan-PI3K/mTORC1/2 inhibitor (Celcuity), in combination with fulvestrant ± palbociclib versus fulvestrant alone in adults with HR+/HER2- advanced breast cancer whose disease progressed on or after a CDK4/6 inhibitor and an aromatase inhibitor. The trial enrolls separate PIK3CA wild-type and PIK3CA-mutant cohorts, both of which reported positive primary-endpoint results: PIK3CA wild-type (presented at ESMO 2025 — the basis for the July 14, 2026 FDA approval) and PIK3CA-mutant (announced May 1, 2026; presented at ASCO 2026). Gedatolisib is FDA-approved for the PIK3CA wild-type indication; its use in PIK3CA-mutant disease remains investigational, with a Celcuity sNDA planned for Q3 2026.
Phase III, global, open-label, randomized trial. The PIK3CA wild-type cohort randomized 1:1:1 to gedatolisib triplet (gedatolisib + palbociclib + fulvestrant), gedatolisib doublet (gedatolisib + fulvestrant), or fulvestrant alone. The PIK3CA-mutant cohort randomized 3:3:1 to gedatolisib triplet, alpelisib + fulvestrant (active comparator), or gedatolisib doublet.
Adults with HR+/HER2- locally advanced or metastatic breast cancer whose disease progressed on or after prior CDK4/6 inhibitor + aromatase inhibitor. Patients enrolled into separate PIK3CA wild-type or PIK3CA-mutant cohorts based on tumor genotype.
Gedatolisib 180 mg IV weekly (3 weeks on / 1 week off, 28-day cycle) + palbociclib 125 mg daily (21 of 28 days) + fulvestrant 500 mg IM (triplet); or gedatolisib + fulvestrant (doublet); or fulvestrant alone (control). PIK3CA-mutant cohort uses alpelisib + fulvestrant as the active comparator instead of fulvestrant alone.
Co-primary endpoints: PFS by blinded independent central review comparing (1) triplet vs control and (2) doublet vs control. Key secondary endpoints: overall survival, ORR, DoR, and patient-reported outcomes.
PIK3CA wild-type cohort (ESMO 2025): the gedatolisib triplet demonstrated a PFS HR of 0.24 (95% CI: 0.17–0.35) vs fulvestrant, a 76% reduction in the risk of disease progression or death. Median PFS was 9.3 months vs 2.0 months. The gedatolisib doublet showed PFS HR 0.33, a 67% risk reduction. PIK3CA-mutant cohort (May 1, 2026): positive topline announcement — both gedatolisib triplet and gedatolisib doublet improved PFS vs the alpelisib + fulvestrant active comparator. Full hazard ratios, medians, and subgroup detail will be presented at ASCO 2026 (May 29 – June 2).
OS data not yet reported in either cohort. Follow-up is ongoing; OS is a key secondary endpoint.
In the PIK3CA-WT cohort, hyperglycemia was notably lower than expected for a PI3K-pathway inhibitor (9.2% triplet, 11.5% doublet) — a key differentiator vs alpelisib. Other most-common AEs are consistent with the palbociclib + fulvestrant backbone (neutropenia, fatigue). Detailed PIK3CA-mutant safety profile to be reported at ASCO 2026.
VIKTORIA-1 represents a potential practice-changing option for HR+/HER2- mBC patients after CDK4/6i failure — a population with limited targeted-therapy choices. Gedatolisib is the first pan-PI3K/mTORC1/2 inhibitor to show positive Phase III results in both PIK3CA-WT and PIK3CA-mutant cohorts. The PIK3CA wild-type cohort (ESMO 2025) is the basis for the July 14, 2026 FDA approval of Revtorpyk (gedatolisib) + fulvestrant ± palbociclib; the May 2026 PIK3CA-mutant readout, presented at ASCO 2026, supports a planned Q3 2026 sNDA for the PIK3CA-mutant population.
VIKTORIA-1 is Celcuity's Phase 3 trial of gedatolisib (Revtorpyk) plus fulvestrant, with or without palbociclib, in HR+/HER2- advanced or metastatic breast cancer after at least one prior line of endocrine therapy. It has two cohorts: Study 1 (PIK3CA wild-type, n=392, versus single-agent fulvestrant) and Study 2 (PIK3CA-mutant, versus alpelisib plus fulvestrant).
Yes. On July 14, 2026 the FDA approved gedatolisib (Revtorpyk, Celcuity) in combination with fulvestrant, with or without palbociclib, for HR+/HER2- PIK3CA wild-type locally advanced or metastatic breast cancer after progression on/after at least one line of endocrine therapy in the metastatic setting. It is the first pan-PI3K/AKT/mTOR inhibitor approved for the wild-type population.
In Study 1 (PIK3CA wild-type), the gedatolisib + fulvestrant + palbociclib triplet had a median PFS of 9.3 months (95% CI 7.2-16.6) versus 2.0 months for single-agent fulvestrant (HR 0.24, p<0.0001). The gedatolisib + fulvestrant doublet had a median PFS of 7.4 months (95% CI 5.5-9.9; HR 0.33, p<0.0001). Objective response rates were 32% (triplet), 28% (doublet), and 1% (fulvestrant).
No. The July 14, 2026 approval is for the PIK3CA wild-type population (Study 1). The PIK3CA-mutant cohort (Study 2, versus alpelisib plus fulvestrant) is a separate readout and is not part of the FDA approval; Celcuity has said it plans a separate supplemental filing for the mutant population.
Gedatolisib is developed by Celcuity. It is a pan-PI3K/AKT/mTOR (PAM) inhibitor administered as 180 mg intravenously over 30 minutes weekly on Days 1, 8, and 15 of each 28-day cycle. Labeled warnings include stomatitis, dermatologic reactions, and hyperglycemia.
UPDATED MAY 2026: Top 8 rows below capture the May 1 PIK3CA-mutant cohort positive readout reaction.