Phase III inavolisib + palbociclib + fulvestrant in PIK3CA-mutated, endocrine-resistant HR+/HER2- mBC. FDA-approved Oct 2024; final OS HR 0.67 (NEJM 2025).
Discover KOL Sentiment on INAVO120 →Design - Phase 3 inavolisib + palbociclib + fulvestrant vs placebo + palbociclib + fulvestrant, PIK3CA-mutated endocrine-resistant HR+/HER2- mBC (NCT04191499).
PFS (primary) - Median 15.0 vs 7.3 mo, HR 0.43 - roughly doubled (the page's KOL summary rounds this to ~17 vs 7 mo).
OS - Final overall survival benefit - HR 0.67 (NEJM 2025); page KOL summary cites median ~34 vs 27 mo.
Safety - PI3Kalpha-class toxicity requiring active management - hyperglycemia, stomatitis/mucositis, diarrhea, ocular events; mandatory baseline glucose assessment + prophylactic mouthwash per label.
Regulatory - FDA approved October 10, 2024.
Sponsor / drugs - Roche / Genentech; inavolisib (Itovebi) + palbociclib (Ibrance) + fulvestrant (Faslodex).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.







Trial slides shared by KOLs at SABCS 2023 / ASCO 2025 / NEJM 2025. Click any image to expand. OCR text extracted via AWS Textract.

[Slide 1] A Overall Survival in the Full Analysis Population 100 96.8 HI Median H 87.0 Overall 90.1 74.3 No. of Survival 75 76.7 Deaths (%) (95% CI) 65.8 Overall Survival (%) mo 67.2 56.5 Inavolisib 50 56.3 72 (44.7) 34.0 (28.4-44.8) (N=161) Inavolisib 46.3 Placebo 82 (50.0) 27.0 (22.8-38.7) (N=164) 25 Placebo Stratified hazard ratio for death, 0.67 (95% CI, 0.48-0.94) P=0.02 0 0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 Months No. at Risk Inavolisib 161 155 149 142 131 114 99 88 78 67 54 43 34 22 19 13 7 1 Placebo 164 155 142 127 119 104 90 77 63 48 42 36 32 18 10 4 2 1 B Analysis of Overall Survival in Key Subgroups Subgroup No. of Patients Median Overall Survival Hazard Ratio for Death (95% CI) Inavolisib Placebo Inavolisib Placebo mo All patients 161 164 34.0 27.0 0.76 (0.55-1.04) Age <65 yr 136 130 36.0 26.8 0.65 (0.46-0.92) >65 yr 25 34 14.4 NR 1.65 (0.77-3.51) Geographic region Asia 58 62 32.7 27.0 0.78 (0.45-1.34) North America or western Europe 63 64 30.2 29.3 0.95 (0.56-1.59) Other 40 38 36.0 16.6 0.53 (0.28-0.98) ECOG performance-status score at baseline 0 100 106 39.2 36.0 0.69 (0.45-1.05) 1 60 58 27.1 26.8 0.85 (0.52-1.38) Menopausal status at randomization Premenopausal 52 52 32.7 23.9 0.67 (0.38-1.19) Postmenopausal 104 111 34.0 28.0 0.81 (0.55-1.19) Visceral disease No 29 36 38.0 40.7 1.06 (0.46-2.46) Yes 132 128 33.0 24.1 0.70 (0.50-0.99) Liver metastases at enrollment No 84 73 38.0 36.0 0.87 (0.53-1.44) Yes 77 91 28.8 21.9 0.72 (0.48-1.10) No. of organs with metastases at enrollment 1 21 32 NR 31.9 0.77 (0.28-2.10) 2 58 46 44.8 24.1 0.51 (0.28-0.90) >3 82 86 28.8 24.2 0.86 (0.57-1.30) Resistance to endocrine therapy Primary 54 58 25.9 22.8 0.69 (0.42-1.14) Secondary 107 105 37.7 34.3 0.77 (0.51-1.16) Hormone receptor status ER-positive, PR-negative 45 45 25.9 38.7 1.16 (0.65-2.08) ER-positive, PR-positive 113 113 39.2 24.5 0.60 (0.41-0.88) Previous endocrine therapy Aromatase inhibitor and tamoxifen 18 19 NR NR 1.15 (0.38-3.44) Aromatase inhibitor only 60 71 26.3 24.2 0.89 (0.56-1.41) Tamoxifen only 82 73 44.8 36.0 0.68 (0.42-1.11) 0.10 0.67 1.00 10.00 Inavolisib Better Placebo Better




[Slide 1] San Antonio Breast Cancer Symposium®, December 5-9, 2023 4 INAVO120 study design Key eligibility criteria Enrolment period: December 2019 to September 2023 Enrichment of patients with poor prognosis: N=325 PIK3CA-mutated, HR+, HER2- ABC by central Inavolisib (9 mg QD PO) + palbociclib (125 mg PO QD D1-D21) ctDNA* or local tissue/ctDNA test fulvestrant (500 mg C1D1/15 and Q4W)** Measurable disease R Until PD Progression during/within 12 months of 1:1 or toxicity adjuvant ET completion Placebo (PO QD) SURVIVAL FOLLOW-UP + palbociclib (125 mg PO QD D1-D21) + No prior therapy for ABC fulvestrant (500 mg C1D1/15 and Q4W)** Fasting glucose <126 mg/dL and HbA1c <6.0% Stratification factors: Endpoints Visceral Disease (Yes vs. No) Primary: PFS by Investigator Endocrine Resistance (Primary VS. Secondary) Secondary: OSF, ORR, BOR, CBR, DOR, PROs Region (North America/Western Europe; Asia; Other) . Central testing for PIK3CA mutations was done on ctDNA using FoundationOneLiquid (Foundation Medicine). In China, the central ctDNA test was the PredicineCARE NGS assay (Huidu). : Defined per 4th European School of Oncology (ESO)-European Society for Medical Oncology (ESMO) International Consensus Guidelines for Advanced Breast Cancer.1 Primary: relapse while on the first 2 years of adjuvant ET; Secondary: relapse while on adjuvant ET after at least 2 years or relapse within 12 months of completing adjuvant ET. : OS testing only if PFS is positive; interim OS analysis at primary PFS analysis; .. Pre-menopausal women received ovarian suppression. ctDNA, circulating tumor DNA; R, randomized. 1. Cardoso F, et al. Ann Oncol 2018;29:1634-1657 This presentation is the intellectual property of the authors. Contact jhaverik@mskcc.org for permission to reprint and/or distribute --- [Slide 2] San Antonio Breast Cancer Symposium®, December 5-9. 2023 9 Primary endpoint: PFS (investigator-assessed) 6-month 12-month 18-month Inavo+Palbo+Fulv Pbo+Palbo+Fulv 100 (n=161) (n=164) 82.9% No. of events, n (%) 82 (50.9) 113 (68.9) Median (95% CI), mo 15.0 (11.3,20.5) 7.3 (5.6,9.3) 75 Stratified hazard ratio (95% CI) 0.43 (0.32, 0.59) 55.9% 55.9% p<0.0001 46.2% 50 32.6% Inavo+Palbo+Fulv 21.1% 25 Pbo+Palbo+Fulv Censored 0 0 3 6 9 12 15 18 21 24 27 30 33 36 Time (mo) Patients at risk: Inavo+Palbo+Fulv 161 134 111 92 66 48 41 Median follow-up: 31 22 13 11 5 1 Pbo+Palbo+Fulv 164 113 77 59 40 23 19 16 12 6 3 3 1 21.3 months CCOD: 29th September 2023 CI, confidence interval; Fulv. fulvestrant; Inavo, inavolisib; mo, months: Palbo, palbociclib; Pbo. placebo; PFS, progression-free survival. This presentation is the intellectual property of the authors. Contact jhaverik@mskcc.org for permission to reprint and/or distribute --- [Slide 3] San Antonio Breast Cancer Symposium®, December 5-9, 2023 12 Key secondary endpoint: Overall survival (interim analysis) Inavo+Palbo Pbo+Palbo 6-month 12-month 18-month +Fulv (n=161) +Fulv (n=164) No. of events, n (%) 42 (26.1) 55 (33.5) 97.3% 100 85.9% Median (95% CI), mo NE (27.3, NE) 31.1 (22.3, NE) Stratified Hazard 0.64 (0.43, 0.97) 73.7% Ratio (95% CI) p=0.0338 75 89.9% 74.9% 67.5% 50 25 Inavo+Palbo+Fulv Pbo+Palbo+Fulv Censored 0 0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 Time (mo) Patients at risk: Inavo+Palbo+Fulv 161 143 127 114 101 85 69 56 38 26 17 8 4 1 1 Median follow-up: Pbo+Palbo+Fulv 164 139 120 98 87 72 61 52 33 19 11 5 3 1 0 21.3 months The pre-specified boundary for os (p of 0.0098 or HR of 0.592) was not crossed at this interim analysis CI, confidence interval: Fulv. fulvestrant; Inavo, inavolisib; mo, months: NE, not estimable; OS, overall survival; Palbo, palbociclib; Pbo, placebo. This presentation is the intellectual property of the authors. Contact jhaverik@mskcc.org for permission to reprint and/or distribute --- [Slide 4] San Antonio Breast Cancer Symposium®, December 5-9, 2023 15 Adverse events with any grade AEs >20% incidence in either treatment group Adverse Events Inavo+Palbo+Fulv Pbo+Palbo+Fulv (N=162) (N=162) All Grades Grade 3-4 All Grades Grade 3-4 Neutropenia 144 (88.9%) 130 (80.2%) 147 (90.7%) 127 (78.4%) Thrombocytopenia 78 (48.1%) 23 (14.2%) 73 (45.1%) 7 (4.3%) Stomatitis/Mucosal inflammation 83 (51.2%) 9 (5.6%) 43 (26.5%) 0 Anemia 60 (37.0%) 10 (6.2%) 59 (36.4%) 3 (1.9%) Hyperglycemia 95 (58.6%) 9 (5.6%) 14 (8.6%) 0 Diarrhea 78 (48.1%) 6 (3.7%) 26 (16.0%) 0 Nausea 45 (27.8%) 1 (0.6%) 27 (16.7%) 0 Rash 41 (25.3%) 0 28 (17.3%) 0 Decreased Appetite 38 (23.5%) <2% 14 (8.6%) <2% Fatigue 38 (23.5%) <2% 21 (13.0%) <2% COVID-19 37 (22.8%) <2% 17 (10.5%) <2% Headache 34 (21.0%) <2% 22 (13.6%) <2% Leukopenia 28 (17.3%) 11 (6.8%) 40 (24.7%) 17 (10.5%) Ocular Toxicities 36 (22.2%) 0 21 (13.0%) 0 Key AEs are shown in bold. AES were assessed per CTCAE V5. Neutropenia, thrombocytopenia, stomatitis/mucosal inflammation, anemia, hyperglycemia, diarrhea, nausea and rash were assessed as medical concepts using grouped terms AE, adverse event; ALT, alanine aminotransferase; AST, aspartate aminotransferase; Fulv, fulvestrant; Inavo, inavolisib; Palbo, palbociclib; Pbo, placebo. This presentation is the intellectual property of the authors. Contact jhaverik@mskcc.org for permission to reprint and/or distribute




[Slide 1] 2025 ASCO® ANNUAL MEETING --- [Slide 2] INAVO120: A Phase III, randomized, double-blind, placebo-controlled study¹,² Key eligibility criteria Enrollment period: January 2020 to September 2023 Enrichment of patients with poor prognosis: N 325 Inavolisib (9 mg PO QD) PIK3CA-mutated, HR+, HER2- aBC by central + palbociclib (125 mg PO QD D1-D21) ctDNA* or local tissue/ctDNA test + fulvestrant (500 mg C1D1/15 and Q4W)+ R Until PD Measurable disease 1:1 or toxicity Placebo (PO QD) SURVIVAL FOLLOW-UP Progression during/within 12 months of + palbociclib (125 mg PO QD D1-D21) adjuvant ET completion + fulvestrant (500 mg C1D1/15 and Q4W)t No prior therapy for aBC Stratification factors: Fasting glucose <126 mg/dL and HbA1c <6.0% Visceral disease (yes vs. no) Endocrine resistance (primary vs. secondary): Region (North America/Western Europe VS. Asia vs. Other) Primary endpoint: Investigator-assessed PFS Secondary endpoints included: OS; investigator-assessed ORR, BOR, CBR, and DoR; PROs ClinicalTrials gov number, NCT04191499 Adapted from Jhaven KJ, of al. SABCS 2023 (Abstract GS03-13). Central testing for PIK3CA mutations was done on CIDNA using FoundationOneLiquid (Foundation Medicine, Inc.). In China, the central ctDNA test was the PredicineCARE NGS assay (Huidu); Pre-menopausal women received ovarian suppression; Defined per 4th European School of Oncology (ESO)-European Society for Medical Oncology (ESMO) International Consensus Guidelines for Advanced Breast Cancer.3 Primary: Relapse while on the first 2 years of adjuvant ET; secondary: Relapse while on adjuvant ET after at least 2 years or misses within 12 months of completing adjuvant ET. aBC, advanced breast cancer; BOR, best overall response; C, cycle; CBR, clinical benefit rate; ctDNA, circulating tumor DNA D, day: DoR duration of response; ET, endocrine therapy: HbAse glycated hemoglobin; HER2-, HER2-negative; QD, daily; R, randomization HR+, hormone receptor-positive; NGS, next-generation sequencing: ORR, objective response rate; OS, overall survival; PD, progressive disease; PFS, progression-free survival; PO, by mouth; PRO, patient-reported outcome; Q4W, every 4 weeks; 1. Turner NC, of at. N Engl J Med 2024; 391:1584-1596 2. Jhaven KJ, of al. SABCS 2023 (Abstract GS03-13); 3. Cardoso F, or at Ann Oncol 2018; 29:1634-1657 2025 ASCO #ASCO25 PRESENTED BY: Nicholas Turner, MD, PhD ASCO AMERICAN SOCIETY OF ANNUAL MEETING CLINICAL ONCOLOGY Presentation is property of the author and ASCO. Permission required for reuse, contact -.og KNOWLEDGE CONQUERS CANCER --- [Slide 3] INAVO120 updated PFS Events, n (%) Median, months (95% CI) Inavolisib (n = 161) 103 (64.0) 17.2 (11.6-22.2) Placebo (n = 164) 141 (86.0) 7.3 (5.9-9.2) 100 83.4 Stratified hazard ratio, 0.42 (95% CI = 0.32-0.55) 75 58.0 PFS (%) 49.7 50 41.8 57.9 Inavolisib 25 31.3 20.5 16.7 Placebo 0 Median follow-up: 0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 34.2 months Months No. at risk Inavolisib 161 146 129 112 89 73 65 57 46 32 25 19 15 11 10 7 3 1 Placebo 164 125 95 74 50 34 30 24 21 14 11 10 8 4 2 1 1 1 The improvement in PFS was maintained during longer follow-up Data cutoff: November 15, 2024. CI, confidence interval; PFS, progression-free survival. © Copyright 2025. 2025 ASCO PRESENTED BY: Nicholas Turner, MD, PhD ASCO AMERICAN SOCIETY OF #ASCO25 CLINICAL ONCOLOGY ANNUAL MEETING Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco.org KNOWLEDGE CONQUERS CANCER --- [Slide 4] INAVO120 key secondary endpoint: os Deaths, n (%) Median, months (95% CI) Inavolisib (n = 161) 72 (44.7) 34.0 (28.4-44.8) Placebo (n = 164) 82 (50.0) 27.0 (22.8-38.7) 96.8 100 87.0 Stratified hazard ratio, 0.67 74.3 (95% CI = 0.48-0.94) 65.8 75 P = 0.0190 90.1 56.5 OS (%) 76.7 50 67.2 Inavolisib 56.3 46.3 25 Placebo 0 Median follow-up: 0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 34.2 months Months No. at risk Inavolisib 161 155 149 142 131 114 99 88 78 67 54 43 34 22 19 13 7 1 Placebo 164 155 142 127 119 104 90 77 63 48 42 36 32 18 10 4 2 1 Improvement in median OS: 7 months. The prespecified boundary for statistical significance (p < 0.0469) was crossed Data cutoff: November 15, 2024. CI, confidence interval; OS, overall survival. © Copyright 2025. 2025 ASCO PRESENTED BY: Nicholas Turner, MD, PhD #ASCO25 ASCO AMERICAN SOCIETY OF CLINICAL ONCOLOGY ANNUAL MEETING Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org KNOWLEDGE CONQUERS CANCER

[Slide 1] Background: INAVO, a highly potent and selective PI3Ka inhibitor that also promotes mutated p110a degradation, is FDA-approved in combination with PALBO + FULV for PIK3CA-mutated, HR+, HER2-, endocrine-resistant aBC, based on the primary analysis of INAV0120 (NCT04191499), which showed a statistically significant and clinically meaningful investigator-assessed progression- free survival (INV-PFS) benefit in the INAVO arm vs. the PBO arm (hazard ratio 0.43; 95% confidence interval [CI] = 0.32-0.59; p < 0.0001). At that analysis, interim OS results were immature. Here we report the final OS analysis, including updated efficacy and safety. --- [Slide 2] Methods: Pts received INAVO (9 mg orally once daily [PO QD]; Days 1-28 of each 28-day cycle)/PBO + PALBO (125 mg PO QD; Days 1-21 of each cycle) + FULV (500 mg intramuscularly; Cycle 1 Days 1 and 15 then every ~4 weeks). OS and objective response rate (ORR) were formally tested; updated INV-PFS and safety analyses are descriptive. --- [Slide 3] Results: Data cut-off was Nov 15, 2024, at 34.2 months (mo) of median follow-up. Median OS was 34.0 mo (95% CI = 28.4-44.8) in the INAVO arm and 27.0 mo (95% CI = 22.8-38.7) in the PBO arm (stratified hazard ratio 0.67; 95% CI = 0.48-0.94; p = 0.0190 [boundary = 0.0469]). The os benefit was consistent across key subgroups. The survival probability at 6, 12, 18, 24, and 30 mo was 96.8%, 87.0%, 74.3%, 65.8%, and 56.5% in the INAVO arm and 90.1%, 76.7%, 67.2%, 56.3%, and 46.3% in the PBO arm. ORR was 62.7% (95% CI = 54.8-70.2) and 28.0% (95% CI = 21.3-35.6), respectively (p < 0.0001). Median time to chemotherapy (TTC) was 35.6 mo (95% CI = 25.4-not reached) in the INAVO arm and 12.6 mo (95% CI = 10.4-16.1) in the PBO arm (stratified hazard ratio 0.43; 95% CI = 0.30- 0.60). Updated median INV-PFS was 17.2 mo (95% CI = 11.6-22.2) in the INAVO arm and 7.3 mo (95% CI = 5.9-9.2) in the PBO arm (stratified hazard ratio 0.42; 95% CI = 0.32-0.55), with landmark --- [Slide 4] analyses supporting durable benefit. 90.7% of pts in the INAVO arm and 84.7% in the PBO arm had grade 3/4 adverse events (AEs); there were no new grade 5 AEs; 63.4% and 13.5% experienced any-grade hyperglycemia (grouped term); and AEs led to INAVO and PBO discontinuation in 6.8% and 0.6% of pts, respectively. Conclusions: INAVO + PALBO + FULV demonstrated a statistically significant and clinically meaningful os benefit compared with PBO + PALBO + FULV. Improvement in INV-PFS was maintained during longer follow-up, along with a substantial and statistically significant improvement in ORR. TTC was also substantially delayed (by ~2 years) by the addition of INAVO to PALBO + FULV. With longer exposure to INAVO, no new safety signals, nor changes in the safety profile, were noted, supporting good tolerability (reflected in low discontinuation due to AEs).
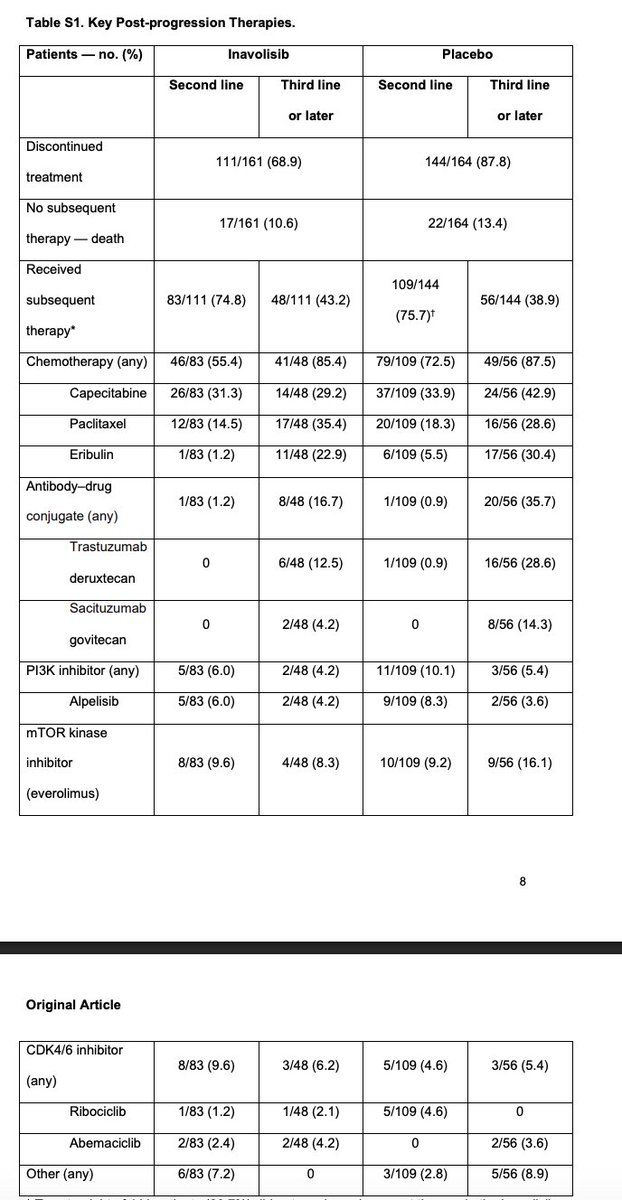
[Slide 1] Table S1. Key Post-progression Therapies. Patients — no. (%) Inavolisib Placebo Second line Third line Second line Third line or later or later Discontinued 111/161 (68.9) 144/164 (87.8) treatment No subsequent 17/161 (10.6) 22/164 (13.4) therapy — death Received 109/144 subsequent 83/111 (74.8) 48/111 (43.2) 56/144 (38.9) (75.7) therapy* Chemotherapy (any) 46/83 (55.4) 41/48 (85.4) 79/109 (72.5) 49/56 (87.5) Capecitabine 26/83 (31.3) 14/48 (29.2) 37/109 (33.9) 24/56 (42.9) Paclitaxel 12/83 (14.5) 17/48 (35.4) 20/109 (18.3) 16/56 (28.6) Eribulin 1/83 (1.2) 11/48 (22.9) 6/109 (5.5) 17/56 (30.4) Antibody-drug 1/83 (1.2) 8/48 (16.7) 1/109 (0.9) 20/56 (35.7) conjugate (any) Trastuzumab 0 6/48 (12.5) 1/109 (0.9) 16/56 (28.6) deruxtecan Sacituzumab 0 2/48 (4.2) 0 8/56 (14.3) govitecan PI3K inhibitor (any) 5/83 (6.0) 2/48 (4.2) 11/109 (10.1) 3/56 (5.4) Alpelisib 5/83 (6.0) 2/48 (4.2) 9/109 (8.3) 2/56 (3.6) mTOR kinase inhibitor 8/83 (9.6) 4/48 (8.3) 10/109 (9.2) 9/56 (16.1) (everolimus) 8 Original Article CDK4/6 inhibitor 8/83 (9.6) 3/48 (6.2) 5/109 (4.6) 3/56 (5.4) (any) Ribociclib 1/83 (1.2) 1/48 (2.1) 5/109 (4.6) 0 Abemaciclib 2/83 (2.4) 2/48 (4.2) 0 2/56 (3.6) Other (any) 6/83 (7.2) 0 3/109 (2.8) 5/56 (8.9)

[Slide 1] The NEW ENGLAND JOURNAL of MEDICINE ORIGINAL ARTICLE Inavolisib-Based Therapy in PIK3CA-Mutated Advanced Breast Cancer N.C. Turner, S.-A. Im, C. Saura, D. Juric, S. Loibl, K. Kalinsky, P. Schmid, S. Loi, P. Sunpaweravong, A. Musolino, H. Li, Q. Zhang, Z. Nowecki, R. Leung, E. Thanopoulou, N. Shankar, G. Lei, T.J. Stout, K.E. Hutchinson, J.L. Schutzman, C. Song, and K.L. Jhaveri A Progression-free Survival in the Full Analysis Population 100 82.9 Progression-free Survival (%) 75 55.9 50 46.2 55.9 Inavolisib 25 32.6 21.1 Placebo 0 0 3 6 9 12 15 18 21 24 27 30 33 36 Months No. at Risk Inavolisib 161 134 111 92 66 48 41 31 22 13 11 5 1 Placebo 164 113 77 59 40 23 19 16 12 6 3 3 1



2026 ESMO BREAST CANCER Annual Congress 420RO: Efficacy of inavolisib (INAVO) + palbociclib (PALBO) + fulvestrant (FULV) in patients (pts) with PIK3CA-mutated, hormone receptor-positive, HER2-negative (HER2-), endocrine-resistant advanced breast cancer (aBC) with and without hyperglycaemia (HG) in the Phase III INAVO120 trial Presenting author: Prof. Dr. med. Sibylle Loibl Universitätsklinikum Frankfurt am Main, Frankfurt am Main, Germany 8 May 2026 This medicinal product is subject to additional monitoring ESMO INAVO120: Background and study design Key eligibility criteria Enrolment period: January 2020 to September 2023 Enrichment of patients with poor prognosis: N 325 INAVO (9 mg PO QD) PIK3CA-mutated. hormone receptor-positive, PALBO (125 mg PO QD D1-D21) HER2-negative aBC by central ctDNA* or local FULV (500 mg C1D1/15 and Q4W)+ tissue/ctDNA test R Until PD 1:1 or toxicity Measurable disease PBO (PO QD) SURVIVAL FOLLOW-UP Progression during/within 12 months of PALBO (125 mg PO QD D1-D21) adjuvant ET completion FULV (500 mg C1D1/15 and Q4W)+ No prior therapy for aBC Stratification factors: Visceral disease (yes vs. no) Fasting glucose <126 mg/dL and HbA1c <%6.0 Endocrine resistance (primary vs. secondary) Region (North America/Western Europe vs. Asia vs. Other) Primary endpoint: Investigator-assessed PFS Secondary endpoints included: OS; investigator-assessed ORR, BOR, CBR and DoR; PROs INAVO120 (NCT04191499) demonstrated statistically significant investigator-assessed PFS and OS benefit for INAVO + PALBO + FULV compared with PBO + PALBO + FULV in patients with PIK3CA-mutated, hormone receptor-positive, HER2-negative, endocrine-resistant aBC¹² Hyperglycaemia (an on-target toxicity with PI3K inhibitors) was recorded in 63.4% VS 13.5% of patients in the INAVO VS placebo arms at the final analysis2 We report efficacy (investigator-assessed PFS, ORR, DoR and OS) in patients with and without INAVO-associated hyperglycaemia - Hyperglycaemia was defined as any reported hyperglycaemia adverse event per CTCAE v5, regardless of grade, duration or treatment received Adapted from Jhaven KJ. et at SABCS 2023 (Abstract GS03-13) Please see side notes for footnotes and abbreviations 1. Turner NC of of N Engl J Med 2024 391:1584-1 1596 2 Jhavori KL of of N Engi , Med 2025 393:151-161 3 Cardoso F. of of Ann Oncol 2018 29:1634-1657 Presenting author: Prof. Dr. med. Sibylle Loibl Content of this presentation IS copyright and responsibility of the author Permission is required for to use ESMO INAVO120: Investigator-assessed PFS by hyperglycaemia status 100 PBO arm INAVO arm with hyperglycaemia INAVO arm without hyperglycaemia 75 + Investigator-assessed PFS (%) Censored 50 25 0- 0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 Time (months) Patients at risk PBO arm 164 125 95 74 50 34 30 24 21 14 11 10 8 4 2 1 1 1 INAVO arm with hyperglycaemia 102 95 86 75 60 50 44 42 34 23 18 14 11 8 7 4 2 0 INAVO arm without hyperglycaemia 59 51 43 37 29 23 21 15 12 9 7 5 4 3 3 3 1 1 INAVO arm with hyperglycaemia INAVO arm without hyperglycaemia PBO arm Patients with event, n (%) 63 (61.8) 40 (67.8) 141 (86.0) Median investigator-assessed PFS, months (95% CI) 21.0(13.4-26.6) 12.8 (9.1-20.5) 7.3(5.9-9.2) Stratified HR vs. PBO arm (95% CI) 0.38 (0.27-0.52)* 0.51 (0.35-0.74)* - Investigator-assessed PFS was consistently improved in the INAVO arm compared with the PBO arm for all patients Data cut-off date 15 November 2024 Updated HR for investigator-assessed PFS for all patients in the INAVO arm vs the PBO arm at the final analysis 0.42 (95% C1032-055) CI, confidence interval, HR, hazard ratio INAVO. inavolisib PBO. placebo, PFS. progression free survival 1 Jhaveri KL, of of N Engl Med 2025, 393:151-161 Presenting author: Prof. Dr. med. Sibylle Loibl Content of this presentation IS copyright and responsibility of the author Permission IS required for re use ESMO INAVO120: Response by hyperglycaemia status INAVO arm INAVO arm All PBO with hyperglycaemia without hyperglycaemia arm patients (n 102) (n 59) (n 164) BOR, n (%) Complete response 4 (3.9) 2 (3.4) 1 (0.6) Partial response 62 (60.8) 33 (55.9) 45 (27.4) Stable disease 29 (28.4) 15 (25.4) 81 (49.4) Progressive disease 6 (5.9) 3 (5.1) 35 (21.3) Missing 1 (1.0) 6 (10.2) 2 (1.2) ORR, n (%) 66 (64.7) 35 (59.3) 46 (28.0) Median TTR, months (95% CI) 3.7 (2.1-7.5) 3.6 (2.0-12.9) NR (NE) Median DoR, months (95% CI) 20.3 (12.2-40.2) 18.2 (9.6-25.8) 11.1 (8.5-20.2)1 [Stratified HR vs. PBO (95% CI)] [0.57 (0.32-0.98)] [0.62 (0.32-1.17)] Data cut-off date 15 November 2024 BOR best overall response, CI, confidence interval, DoR duration of response HR, hazard ratio, INAVO, inavolisib NE not estimable NR. not reached ORR objective response rate; PBO, placebo, TTR time to response 1 Jhaveri KI., of at N Engl J Med 2025 393:151-161 Presenting author: Prof. Dr. med. Sibylle Loibl Content of this presentation IS copyright and responsibility of the author Permission IS required for re use ESMO



Highest-engagement tweets about this trial, ranked by KOL discussant count (replies + quote-tweets). Replies in green, quote-tweets in blue. Wall Street, stock-promo, and non-substantive replies excluded.
🔥 Big Win in HR+/HER2– Breast Cancer! Final #INAVO120 results at #ASCO25 show OS benefit with INAVO + PALBO + Fulvestrant in PIK3CA-mutated, endocrine-resistant ABC: ✅ OS: 34.0 vs 27.0 mo ✅ HR 0.67 | p = 0.019 ✅ INV-PFS: 17.2 vs 7.3 mo ✅ ORR: 62.7% vs 28% ✅ TTC delay: ~2 https://
Full text of INAVO120 abstract below 🙂👇. Check the tweet below for analysis @ASCO #ASCO25 https://t.co/BFQN3ULXh3 https://t.co/5VTfN5tGfM

#BreastCancer #OncoTwitter #PrecisionOncology #PIK3CA @ASCO #ASCO25 @OncoAlert A 24-month landmark analysis, if 50% of controls vs. 65% of INAVO patients survived, NNT = 1/(0.65–0.50) = ~7 patients to prevent one death

wouldn't change current indication though..
#BreastCancer #OncoTwitter #PrecisionOncology #PIK3CA @ASCO #ASCO25 @OncoAlert Demonstrating survival gains in advanced breast cancer (ABC) is notoriously difficult—this is a landmark for PI3K-targeted therapy.

Will need to see ❓crossover ❓PIK3CA ⛔️ use in control
INAVO120 OS Benefit: 7-month median (OS)(34.0 vs. 27.0 mo; HR 0.67, p=0.019) in a high-risk, endocrine-resistant. Robust PFS & Response: Inv PFS doubled (17.2 vs. 7.3 mo), with ORR >60% vs. 28% in controls, s/o tumor







 +4
+4
Nick Turner presents OS results from INAVO120. Adding inavo to 1L fulv/palvo for high-risk PIK3CAm HR+/HER2- MBC improved PFS (17 vs 7 m) & OS (34 vs 27 mo), though low crossover to alpelisib (10%). Toxicities non-negligible. Concomitant @NEJM publication: https://t.co/Ugi320uOqL
#SABCS23 Highlights w/ @hoperugo on HR+ #breastcancer - #NATALEE - #MONARCH3 - #INAVO120 - #TB01 Full discussion: - https://t.co/jZrRZsOfeq - https://t.co/ovqFoUtlwT - Also on “Oncology Brothers” podcast #MedTwitter #OncTwitter #bcsm @SABCSSanAntonio @TargetedOnc https://t







 +4
+4
Breast Cancer Highlights from #ASCO24 w/ @ErikaHamilton9 - #RxPonder - #postMONARCH - #INAVO120 - #DB06 - #EMERALD Full Int: - https://t.co/ukNyzlPC8Y - https://t.co/Q0WZyfiGBl - Also on the “Oncology Brothers” podcast #bcsm @ASCO #OncTwitter #MedTwitter @TargetedOnc http
#INAVO120, which led to the approval of inavolisib for HR+/HER2- MBC, is now published in @NEJM. Strong data, with doubling of PFS & ORR by adding inavo to fulv/palbo among high-risk patients (with PIK3CA mut & early recurrence). Non-negligible toxicities. https://t.co/Z8bXVAs4Zp
Important to see OS benefit. A theme for @ASCO #ASCO25 is vital need of defining X-over therapy/therapy at PD. In INAVO120, crossover was variable; 85% chemo but only 35% got ADC, 5% got PIK3CA inhibitor, 39% more ET. Likely important for SERANA-6 and DB-09 trials, too. https:
INAVO120 is a Phase III, double-blind, randomized trial that established inavolisib (Itovebi, oral PI3Kα inhibitor) plus palbociclib and fulvestrant as a new standard for patients with PIK3CA-mutated, HR+/HER2- endocrine-resistant locally advanced or metastatic breast cancer. The triplet doubled median PFS and produced a statistically significant 7-month median OS improvement — rare for post-CDK4/6 PI3K-targeted combinations. The FDA approved the regimen on October 10, 2024.
On October 10, 2024, the FDA approved inavolisib in combination with palbociclib and fulvestrant for endocrine-resistant, PIK3CA-mutated, HR-positive, HER2-negative, locally advanced or metastatic breast cancer. Approval based on INAVO120 PFS results; FDA-approved companion diagnostic for PIK3CA mutation testing required.
Approval date: October 10, 2024
Population: Patients with PIK3CA-mutated (centrally confirmed), HR+/HER2-, endocrine-resistant locally advanced or metastatic breast cancer.
Interventions: Inavolisib + palbociclib + fulvestrant versus placebo + palbociclib + fulvestrant. Mandatory baseline glucose monitoring and prophylactic mouthwash per labeling.
Endpoints: Primary: investigator-assessed PFS (ITT). Key secondary: OS. Other: ORR, DoR, safety.
Primary PFS analysis (NEJM 2024): median PFS 15.0 months (95% CI 11.3-20.5) with inavolisib triplet vs 7.3 months (95% CI 5.6-9.3) with placebo doublet (HR 0.43; 95% CI 0.32-0.59; p<0.0001) — doubling of median PFS. Final OS analysis (NEJM 2025): median OS 34.0 vs 27.0 months (HR 0.67; 95% CI 0.48-0.94; p=0.019) — statistically significant 7-month median OS improvement.
Hyperglycemia, stomatitis/mucositis, diarrhea, and ocular toxicity occurred more frequently with inavolisib than placebo. Mandatory baseline glucose assessment and prophylactic mouthwash recommended per FDA labeling. No new safety signals beyond known PI3Kα-class effects. Rates of treatment discontinuation due to AEs were manageable with appropriate prophylaxis.
Paolo Tarantino summarized the practice-defining OS readout: “Nick Turner presents OS results from INAVO120. Adding inavo to 1L fulv/palvo for high-risk PIK3CAm HR+/HER2- MBC improved PFS (17 vs 7 m) & OS (34 vs 27 mo), though low crossover to alpelisib (10%). Toxicities non-negligible.” In a separate post he flagged the NEJM publication, noting “Strong data, with doubling of PFS & ORR by adding inavo to fulv/palbo among high-risk patients (with PIK3CA mut & early recurrence). Non-negligible toxicities.” Harold Burstein widened the lens to the crossover question that recurs across the HR+ field: “Important to see OS benefit. A theme for @ASCO #ASCO25 is vital need of defining X-over therapy/therapy at PD. In INAVO120, crossover was variable; 85% chemo but only 35% got ADC, 5% got PIK3CA inhibitor, 39% more ET,” adding this is “Likely important for SERANA-6 and DB-09 trials, too.” Suyog Akhade tabulated the win directly: “OS: 34.0 vs 27.0 mo,” “HR 0.67 | p = 0.019,” “INV-PFS: 17.2 vs 7.3 mo,” “ORR: 62.7% vs 28%.”
INAVO120 is a Phase 3 randomized trial (NCT04191499) of the PI3Kalpha inhibitor inavolisib (Itovebi) plus palbociclib and fulvestrant versus placebo plus palbociclib and fulvestrant in patients with PIK3CA-mutated, endocrine-resistant, HR-positive, HER2-negative metastatic breast cancer. Progression-free survival was the primary endpoint.
Adding inavolisib roughly doubled progression-free survival - median PFS 15.0 versus 7.3 months (HR 0.43) - and the final analysis reported a statistically significant overall survival benefit with a hazard ratio of about 0.67 (NEJM 2025), despite low crossover to another PI3K inhibitor. Objective response rate was also roughly doubled with the triplet.
Yes. On October 10, 2024 the FDA approved inavolisib (Itovebi) in combination with palbociclib and fulvestrant for endocrine-resistant, PIK3CA-mutated, HR-positive, HER2-negative locally advanced or metastatic breast cancer, as detected by an FDA-approved test, in patients who relapsed on or after adjuvant endocrine therapy.
The regimen carries PI3Kalpha-class toxicity that requires active management, including hyperglycemia, stomatitis/mucositis, diarrhea, and ocular events, which occurred more often with inavolisib than placebo. FDA labeling recommends mandatory baseline glucose assessment and prophylactic anti-inflammatory mouthwash; no new safety signals beyond known PI3Kalpha-class effects were seen.
Candidates are patients with HR-positive, HER2-negative metastatic breast cancer whose tumors carry a PIK3CA mutation (confirmed by an FDA-approved test) and whose disease recurred on or after completing adjuvant endocrine therapy - the endocrine-resistant, PIK3CA-mutated population studied in INAVO120.













