Giredestrant (oral SERD) + everolimus vs physician's choice endocrine therapy + everolimus in ER+/HER2- advanced breast cancer after CDK4/6 inhibition — Roche/Genentech
Read Roche Press Release →







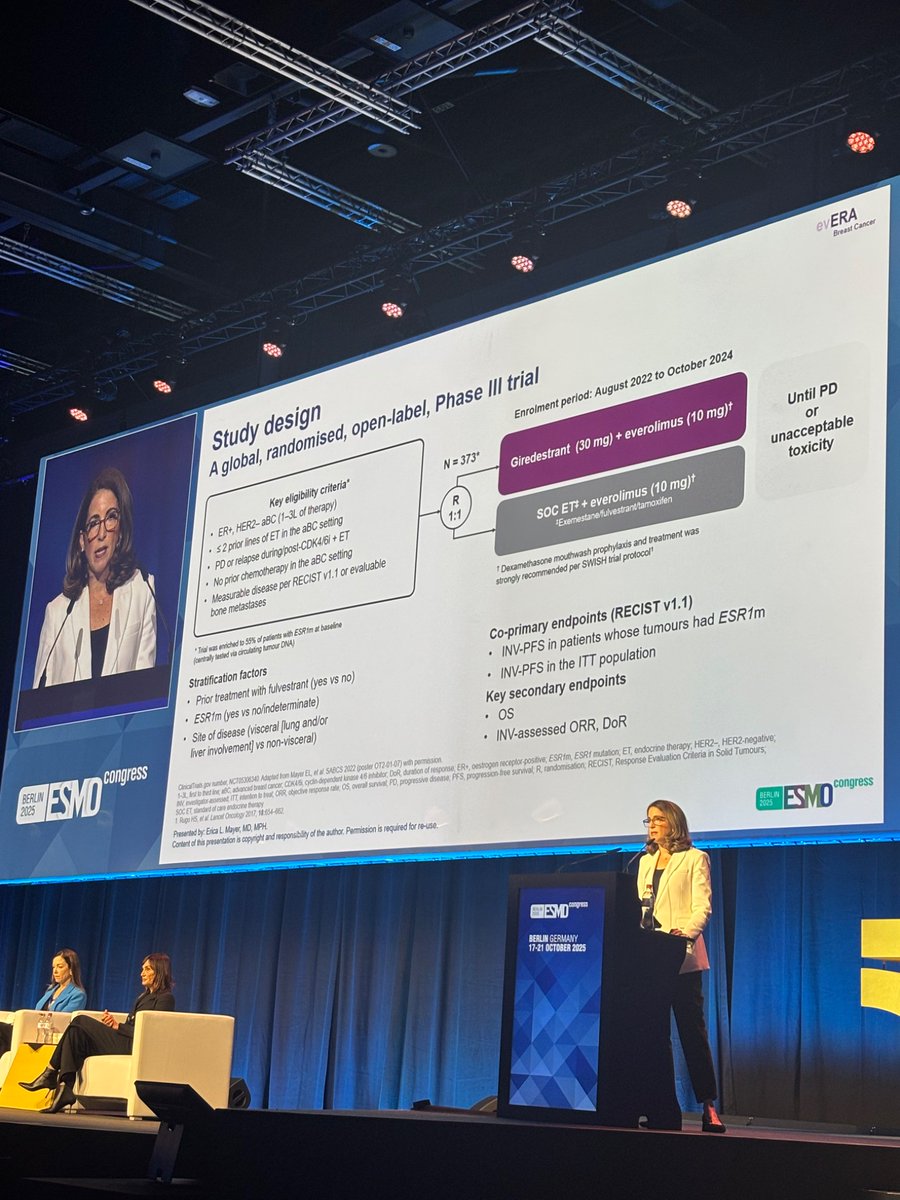
evERA Breast Cancer is a randomized, open-label Phase 3 trial from Roche/Genentech evaluating giredestrant (oral SERD) + everolimus vs physician's choice endocrine therapy + everolimus in patients with ER+/HER2-negative locally advanced or metastatic breast cancer that has progressed after a CDK4/6 inhibitor. The study was enriched for ESR1-mutated patients and built ESR1-mutation status into its co-primary analysis. At ESMO 2025 the trial met its co-primary PFS endpoints in both the ITT and ESR1-mutated populations; updated subgroup data followed at SABCS 2025, post-progression (PFS2/OS) analyses at ASCO 2026, and patient-reported outcomes at ESMO Breast 2026. evERA sits within the broader giredestrant program alongside lidERA (early breast cancer), pionERA (CDK4/6-resistant), and persevERA (1L — which did not meet its primary PFS endpoint).
Adults with ER+/HER2-negative locally advanced or metastatic breast cancer previously treated with a CDK4/6 inhibitor plus endocrine therapy. The trial was enriched for ESR1-mutated patients, with ESR1-mutation status built into the co-primary analysis. Randomized open-label, stratified by ESR1-mutation status, visceral disease, and prior endocrine-therapy duration.
Experimental: Giredestrant (oral SERD) + everolimus 10 mg daily.
Control: Physician's choice endocrine therapy + everolimus 10 mg daily.
Patients continued until disease progression or unacceptable toxicity.
The co-primary investigator-assessed PFS endpoints were met in both populations. In the ITT population, median PFS was 8.77 vs 5.49 months — HR 0.56 (95% CI 0.44–0.71); p<0.0001. In the ESR1-mutated population, median PFS was 9.99 vs 5.45 months — HR 0.38 (95% CI 0.27–0.54); p<0.0001. The benefit was largest in ESR1-mutated tumors; the ESR1-wildtype subgroup showed a more modest PFS difference (with ORR still improved).
Exploratory post-progression analyses presented at ASCO 2026 by Komal L. Jhaveri, MD (MSK / Weill Cornell) showed longer PFS2 (time to second progression) and longer chemotherapy-free survival (CFS) with giredestrant + everolimus vs SoC ET + everolimus, with the greatest benefit in the ESR1-mutated population. PFS2 HR 0.69 (ITT) and 0.61 (ESR1-mut); CFS HR 0.61 (ITT) and 0.46 (ESR1-mut). These data support durability of benefit beyond the first progression.
OS data remain immature but show a clear positive trend in both populations: ITT HR 0.69 (95% CI 0.47–1.00, p=0.0473) and ESR1-mutated HR 0.62 (95% CI 0.38–1.02, p=0.0566) at the primary analysis. Follow-up for OS continues to the next analysis.
Objective response rate (ORR) was improved with giredestrant + everolimus in both ESR1-mutated and ESR1-wildtype subgroups. SABCS 2025 subgroup analyses (presented by Hope Rugo) showed a consistent PFS benefit across genomic and clinical subgroups — including PI3K-pathway alterations (PIK3CA, AKT1, PTEN), visceral vs non-visceral disease, and prior endocrine-therapy duration — with the magnitude greatest in ESR1-mutated tumors.
Giredestrant + everolimus was well tolerated with no new safety signals and no added toxicity beyond the everolimus backbone — adverse events were consistent with the known profiles of the individual medicines. Notably there was no photopsia — a class effect seen with some other oral SERDs. Pneumonitis events were low-grade and reversible, at incidence rates consistent with prior everolimus studies. The dominant tolerability issue is stomatitis from everolimus; the ESMO Breast Cancer 2026 safety/PRO update (Miguel Martin) showed that prophylactic dexamethasone mouth rinse (used by 62.5% of patients) reduced clinically significant stomatitis — grade 2: 14.4% with prophylaxis vs 21.1% without; grade 3: 1.8% vs 4.2%; no grade 4/5 — and delayed onset. AE-related discontinuation was low (5.3% giredestrant vs 8.2% control).
The central interpretive tension is biomarker selection. Erika Hamilton flagged it directly: "No benefit among those patients WITHOUT ESR1m. Although ITT was significant with high % of pts with ESR1m, benefit is NOT in all-comers." Hope Rugo — on the discussant side of the ESMO 2025 presentation by Erica Mayer — described "very nice data from EVERA combining giredestrant/everolimus vs SOC ET/everolimus with marked improvement in PFS and ORR in mESR1 and ITT," adding at SABCS 2025: "Note PFS in non-ESR1m subgroup similar. ORR better." Sarah Sammons summarized the topline: giredestrant + everolimus "doubled PFS vs SOC ET + everolimus … 10 mo vs 5.4 mo in ESR1-mut tumors." Virginia Kaklamani placed evERA next to EMBER-3: "Combo benefit similar to evera trial although here benefit regardless of esr1m. Would love to see the combo approved." Luca Recco noted the SABCS 2025 subgroup picture (consistent benefit, particularly in PI3K-pathway alterations), and Abi Siva flagged the practical PRO detail — dexamethasone mouth rinse for all patients.
⚠ evERA positions giredestrant + everolimus as an all-oral post-CDK4/6i option in ER+/HER2- advanced breast cancer, with the largest benefit in ESR1-mutated disease — sharpening the case for ESR1 testing at progression to guide sequencing. The contrast with persevERA (negative in the 1L AI-replacement setting) reinforces that the value of oral SERDs lies after endocrine resistance rather than as a frontline AI substitute. Comparisons against EMBER-3 (imlunestrant), SERENA-6 (camizestrant, ctDNA-guided), INAVO120 (inavolisib), and CAPItello-291 (capivasertib) frame how SERD- and PI3K/AKT-pathway strategies will be sequenced in this space.