Giredestrant (oral SERD) + palbociclib vs letrozole + palbociclib in 1L ER+/HER2- advanced breast cancer — Roche/Genentech
Read Roche Press Update →





PERSEVERA (persevERA) is a randomized, double-blind, placebo-controlled Phase 3 trial evaluating giredestrant (oral SERD) + palbociclib vs letrozole + palbociclib in patients with 1L ER+/HER2-negative locally advanced or metastatic breast cancer. ~992 patients were randomized. The trial tested whether an oral selective estrogen receptor degrader (SERD) could replace aromatase inhibitors as the endocrine backbone alongside CDK4/6 inhibition in the front-line setting. Companion programs in the giredestrant development program — lidERA (early breast cancer), evERA (advanced post-endocrine resistance), and pionERA (post-CDK4/6 resistant) — remain ongoing.
ER+/HER2-negative locally advanced or metastatic breast cancer; no prior systemic therapy for advanced disease (frontline setting). Approximately 992 patients randomized 1:1.
Experimental: Giredestrant 30 mg PO once daily + Palbociclib 125 mg PO (Days 1–21 of a 28-day cycle).
Control: Letrozole 2.5 mg PO once daily + Palbociclib 125 mg PO (Days 1–21 of a 28-day cycle).
The primary investigator-assessed PFS (INV-PFS) endpoint was not met. Full data presented at ASCO 2026 (Abstract LBA1006, Nicholas C. Turner) showed median PFS of 33.1 months (95% CI 30.2–38.3) with giredestrant + palbociclib vs 28.2 months (95% CI 25.0–33.1) with letrozole + palbociclib — stratified HR 0.89 (95% CI 0.76–1.05), p = 0.1553. The pre-specified significance boundary (HR 0.85, 2-sided p < 0.0456) was not crossed: a numerical benefit only, with no demonstrated superiority over the letrozole + palbociclib standard. Median follow-up ~52 months; data cutoff January 30, 2026.
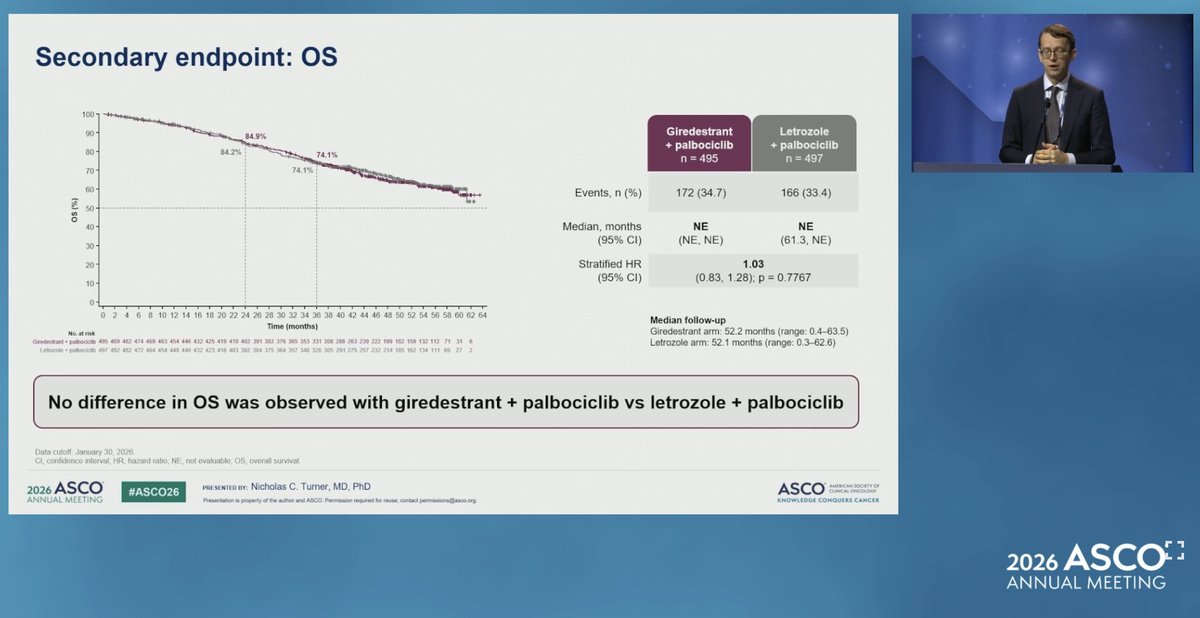
OS, a key secondary endpoint, showed no difference between arms at the January 30, 2026 data cutoff. Events: 172/495 (34.7%) with giredestrant + palbociclib vs 166/497 (33.4%) with letrozole + palbociclib. Median OS was not estimable (NE) in both arms (control 95% CI 61.3–NE). Stratified HR 1.03 (95% CI 0.83–1.28), p = 0.7767.
Tumor response was similar between arms: objective response rate (ORR) 60.2% with giredestrant + palbociclib vs 59.9% with letrozole + palbociclib; clinical benefit rate (CBR) 82.6% vs 82.1%. Duration of response (DoR) was numerically longer with giredestrant — median 38.5 months (95% CI 30.4–48.7) vs 30.4 months (95% CI 25.3–36.1) — but without statistical significance, consistent with the deeper ER suppression the oral SERD provides without translating into a PFS win.
Safety was consistent with the known profiles of giredestrant and palbociclib individually, with no unexpected findings. Any-grade adverse events occurred in 99.8% (giredestrant arm) vs 98.0% (letrozole arm); grade 3/4 AEs in 85.5% vs 80.8%; AEs leading to treatment discontinuation were low and similar (9.5% vs 8.3%). Neutropenia was the dominant AE in both arms (CDK4/6 class effect). The one distinctive signal was bradycardia, more frequent with giredestrant (11.7% vs 1.8%) — but the vast majority were grade 1 and asymptomatic, with no grade 3/4 events in either arm.
KOLs have proposed four mechanistic explanations for the negative readout, drawn from @ChandrakanthMv's published breakdown:
① Frontline disease is highly endocrine-sensitive. Aromatase inhibition + CDK4/6 already achieves strong ER pathway suppression in untreated mBC. Replacing the AI with an oral SERD offers limited incremental benefit in this setting.
② ESR1 mutations are uncommon upfront. ESR1 mutations — where oral SERDs typically show their advantage — emerge after AI exposure. Frontline populations therefore derive limited SERD-specific benefit.
③ CDK4/6 already blocks downstream signaling. Palbociclib suppresses ER-driven cell-cycle progression. Additional ER degradation may not significantly enhance disease control beyond what CDK4/6 inhibition already provides.
④ Strong comparator arm. Letrozole + palbociclib is a highly effective standard. Superiority against this backbone is difficult to demonstrate.
ASCO discussant Matthew P. Goetz, MD (Mayo Clinic) framed the central interpretation: in the frontline setting, palbociclib suppresses ER-driven cell-cycle progression so effectively that swapping the aromatase inhibitor for an oral SERD adds little incremental benefit — the CDK4/6 inhibitor "blunts" any advantage the SERD might otherwise show. He also raised an alternative hypothesis: that mechanisms driving CDK4/6 resistance are not addressed simply by exchanging a SERD for an AI. His proposed path forward is strategic deployment of oral SERDs — potentially as 1L monotherapy with timing matched to a patient's risk profile — rather than a blanket AI-for-SERD substitution on the CDK4/6 backbone.
⚠️ AI + CDK4/6 remains the standard first-line therapy in ER+/HER2- metastatic breast cancer. PERSEVERA suggests oral SERDs do not displace aromatase inhibitors in the 1L setting. The likely value proposition for oral SERDs remains after endocrine resistance or in ESR1-mutant disease — settings being tested in evERA (advanced post-endocrine resistance) and pionERA (post-CDK4/6 resistant). The adjuvant question — does an oral SERD reduce recurrence vs AI in early disease — is being tested in lidERA. Contrast against EMBER-3 (imlunestrant) and SERENA-6 (camizestrant), where SERDs have shown benefit in selected resistant/ESR1-mutant populations.