ASCO26 Trending Images
Curated visuals from the ASCO 2026 KOL and finance communities.

 Nicole Casasanta, MD @ncasasanta
Nicole Casasanta, MD @ncasasanta
 Sara Tolaney @stolaney1
Sara Tolaney @stolaney1
 Fumiko Ladd Chino, MD, FASCO @fumikochino
Fumiko Ladd Chino, MD, FASCO @fumikochino
 Omar Peña Curiel @OmarOnco
Omar Peña Curiel @OmarOnco
 Shaalan Beg MD MBA FASCO @ShaalanBeg
Shaalan Beg MD MBA FASCO @ShaalanBeg
 Masahiro TORASAWA, MD. PhD. @M_Torasawa
Masahiro TORASAWA, MD. PhD. @M_Torasawa
 hanna geissler @hannagsslr
hanna geissler @hannagsslr
 Lorenza Rimassa @LorenzaRimassa
Lorenza Rimassa @LorenzaRimassa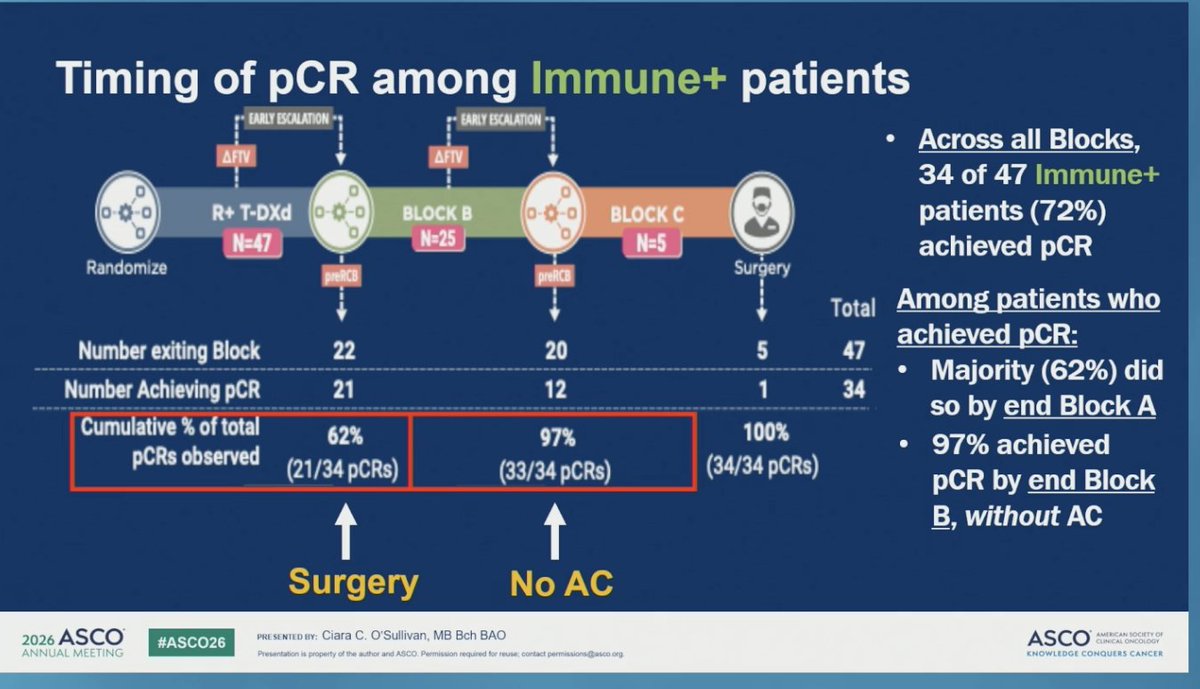 Sara Tolaney @stolaney1
Sara Tolaney @stolaney1
 Katy Beckermann @katy_beckermann
Katy Beckermann @katy_beckermann Katy Beckermann @katy_beckermann
Katy Beckermann @katy_beckermann
 Yakup Ergün @dr_yakupergun
Yakup Ergün @dr_yakupergun
 Memorial Sloan Kettering Cancer Center @MSKCancerCenter
Memorial Sloan Kettering Cancer Center @MSKCancerCenter
 Samer Al Hadidi, MD,MS,FACP @HadidiSamer
Samer Al Hadidi, MD,MS,FACP @HadidiSamer
 Elisabetta Bonzano MD, PhD @to_be_elizabeth
Elisabetta Bonzano MD, PhD @to_be_elizabeth
 Adam Feuerstein ✡️ @adamfeuerstein
Adam Feuerstein ✡️ @adamfeuerstein Adam Feuerstein ✡️ @adamfeuerstein
Adam Feuerstein ✡️ @adamfeuerstein
 MSK Department of Medicine @MSK_DeptOfMed
MSK Department of Medicine @MSK_DeptOfMed
 Thierry Alcindor, MD, MSc @Thalcin
Thierry Alcindor, MD, MSc @Thalcin




























Top Themes at ASCO 2026
Most-discussed scientific topics across 4,841 curated tweets from 683 researchers and oncologists. Tap any card to see the tweets.





Top Voices by Impressions
Ranked by total impressions across all ASCO 2026 pre-conference tweets captured. Switch tabs to view physicians, institutions, media, pharma/corporate, and finance/investor voices separately.














Top Tweets by Tumor Type
Highest-impact physician tweets by cancer type. Expand the Clinical Trials section under each tumor type to drill into trial-specific discussion.

































































































































































































































Key Trial Profiles on KOL Pulse
In-depth KOL Pulse trial profiles for studies featured at ASCO 2026 — KOL discussion, conference slides, results, and sentiment for each trial.
Major Media Coverage Heading Into ASCO 2026
Key stories, publications, and press coverage from the AACR Annual Meeting — curated from major oncology media and ASCO previews.
Finance Buzz by Tumor Type
Tweets carrying stock cashtags ($TICKER) — investor, IR, and analyst commentary — segregated from the physician feed and grouped by cancer type.
ASCO 2026 Catalysts 10 confirmed
Confirmed ASCO 2026 disclosures for tickers in the buzz feed below — abstract slots and toplines per company press releases & meeting previews. Not investment advice.
⬜ Other / Multi-Tumor 178 buzz
🔵 GI Cancers 26 buzz


🫁 Lung Cancer 19 buzz

🔷 GU Cancers 8 buzz



🌑 Melanoma 5 buzz




🩸 Leukemia & Lymphoma 2 buzz
🦴 Sarcoma 2 buzz

🎗️ Breast Cancer 2 buzz

Get Daily ASCO 2026 Updates
A quick daily digest — top KOL voices, plenary highlights, and trial signals from Chicago, delivered to your inbox throughout the meeting.