DESTINY-Breast11 Key Takeaways
Design — Phase 3, open-label; neoadjuvant T-DXd->THP vs ddAC-THP, high-risk HER2+ early breast cancer (NCT05113251). (ESMO 2025)
pCR (primary) — 67.3% vs 56.3% (delta 11.2%; p=0.003). (ESMO 2025, Harbeck)
RCB-0+I (updated) — 81.3% vs 69.1% favoring T-DXd-THP. (ESMO Breast 2026, Pusztai)
Safety — Better than ddAC-THP: Grade >=3 AEs 37.5% vs 55.8%; serious AEs 10.6% vs 20.2%; all-grade LV dysfunction 1.3% vs 6.1%. (ESMO 2025)
Regulatory — FDA approved May 15, 2026 (neoadjuvant HER2+ Stage II-III, followed by THP). (FDA.gov)
Sponsor / Drug — Daiichi Sankyo / AstraZeneca; T-DXd (Enhertu), a HER2-directed antibody-drug conjugate. (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.
Top KOLs Discussing DESTINY-Breast11







DESTINY-Breast11 Key Slides & Visuals
Trial slides shared by KOLs at SABCS 2025 / ESMO Breast 2026. Click any image to expand. OCR text extracted via AWS Textract.



[Slide 1] What We Have Learned A neoadjuvant ADC-based regimen, T-DXd-THP, with less chemotherapy improves pathologic response compared to ddAC-THP in high-risk HER2+ early breast cancer This is the 4th trial to show anthracyclines do not improve pCR in high-risk HER2+ Sara Hurvitz early breast cancer Invited Discussant 2910 Anthracyclines are less safe than non-anthracycline, T-DXd-based regimens Without a better way to select patients, use of an ADC as the sole source of chemotherapy is inadequate neoadjuvant treatment for high-risk HER2+ early BC congress ESMO Content of this presentation 8 copynght and responsibility of the author Permission is required for re use --- [Slide 2] DESTINY-Breast11: The FIRST Phase 3 Trial of Neoadjuvant T-DXd in HER2+ eBC ITT population* (primary endpoint) HR-positive HR-negative A11.2% A16.1% 100 (95% CI 4.0, 18.3; P=0.0031) (95% CI 3.0, 28.8) A9.1% 80 67.3 83.1 (95% C102. 17.9) 56.3 67.1 60 61.4 pCR (%)* 52.3 Sara Hurvitz 40 Invited Discussant 2910 20 216/321 180/320 145/236 123/235 69/83 57/85 0 T-DXd-THP ddAC-THP T-DXd-THP ddAC-THP T-DXd-THP ddAC-THP pCR significantly improved in T-DXd-THP arm! Control arm performed as predicted First phase III evidence that replacing chemotherapy with an ADC in neoadjuvant setting improves pCR congress ESMO Content of this presentation is copyright and responsibility of the author Permission is required for re-use Sara Hurvitz, MD --- [Slide 3] Would T-DXd-THP have beat TCHP? pCR in Phase III Trials of Neoadjuvant Taxane/Carbo/HP Regimen/ Study N pCR pCR HR- pCR HR+ TCHP X 6 KRISTINE-TRIO-021/Hurvitz, et al. 221 56% 73% 44% Lancet Oncol 2018 TCHP X 6 HELEN-006/Chen X-C et al. Lancet 337 58% 70% 48% Oncol. 2025;26(1):27-36. Sara Hurvitz TCHP X 6 (T=q3 weekly docetaxel, Invited Discussant 2910 paclitaxel or nab-paclitaxel) 387 66% 78% 59% neoCARHP/Wang K et al. ASCO 2025 Paclitaxel/Carbo/HP X 9 cycles TRAIN-2/van Ramshorst et al. 206 67% 84% 55% Lancet Oncol 2018 Presenter: Sara A. Hurvitz, MD. FACP ESMO Content of this presentation 13 copyrighted and responsibility of the author Permission a required for re-use --- [Slide 4] CONCLUSIONS T-DXd-THP improves pCR compared to AC-THP in high-risk HER2+ early breast cancer This provides further (already ample) evidence that anthracyclines are less safe than non-anthracycline based regimens and do not add to pCR rates in high-risk HER2+ early breast cancer Use of an ADC such as T-DXd as the sole source of chemotherapy is inadequate neoadjuvant treatment for high-risk HER2+ early breast cancer but patients with lower risk disease or biomarker- defined populations might be selected for a de-escalated strategy with single agent ADC in the future Long term outcomes with T-DXd THP are not yet known (and the study was not powered for these endpoints); moreover the management of residual disease after T-DXd-THP remains undefined Eagerly await the results of DB-05 (just moments away!!) to determine whether the use of T-DXd for very high-risk patients with residual disease after standard neoadjuvant therapy leads to improved outcomes congress ESMO Content of this presentation is copyright and responsibility of the author Permission is required for re-use

[Slide 1] No pCR Benefit with Addition of Anthracycline to Neoadjuvant Trastuzumab-Based Regimen in HER2+ BC Study pCR Anthracycline pCR Non-Anthracycline TRYPHAENA/Schneeweiss Ann Oncol 2013;24:2778-84 56% 64% (FECHPx3 THPx3 vs TCHPx6) TRAIN-2/van Ramshorst et al, Lancet Oncol 2018;19 67% 68% (FECx3 TCHPx6 vs TCHPx9) neo-CARH/Gao HF, et al. Ther Adv Med Oncol. 2021;13; 37% 56% (EC-TH vs TCH) DESTINY-Breast11/Harbeck ESMO 2025 (ACx4 THPx4 VS T-DXdx4 THPx4) 56% 67% Presenter: Sara A. Hurvitz, MD, FACP ESMO Content of this presentation is copyrighted and responsibility of the author Permission is required for re-use

[Slide 1] 16:30 - 18:15 Presidential Symposium | CHAIRS: GIUSEPPE CURIGLIANO, BRIGETTE MA FUTURE STUDIES NEEDED HOW COULD WE INTEGRATE DB11 AND DB05? Can we use a response-guided approach? HP pCR X 14 cycles ctDNA cT≥3 or cN+ THP Breast MRI undetectable Surgery TDXd HER2+ BC x12 wks (at C2D1) response RD x14 cycles Any HR status Sara Tolaney Check ctDNA: If no response Baseline & Baseline breast MRI Cycle Day 1 HP Invited Discussant LBA1 for all patients ctDNA pCR T-DXd for 4 X 14 cycles Baseline tumor-informed detectable cycles Surgery ultrasensitive ctDNA for (at C2D1) RCB2/3 all patients RD ACx4-T-DM1x Plasma samples for serial ctDNA testing 14 cycles RCB1 " " T-DM1 X 14 cycles Baseline C2d1 (week 0) (week 3) Side adapted from Bia Sequi/Ada Waks BERLIN AUDITORIUM - HUB 27




[Slide 1] DESTINY-Breast11 study design A randomized, global, multicenter, open-label, Phase 3 study (NCT05113251) Data cutoff: March 12, 2025 n=321 T-DXd* THP Recommended Primary endpoint Patient population 4 + 4 cycles post-neoadjuvant pCR (ypTO/is ypN0) by blinded Previously untreated central review treatment per study HER2+ eBC protocol Secondary endpoints HR-positive or n=320 HR-negative Randomized ddAC THP$ Surgery pCR: radiotherapy and pCR (ypTO ypN0) by blinded concomitant trastuzumab + central review 1:1:1 4 + 4 cycles High-risk defined as: pertuzumab for up to 1 year EFS - ≥cT3 and NO-3 or No pCR: radiotherapy and Safety cT0-4 and N1-3 T-DM1 for up to 14 cycles Pharmacokinetics and n=286 T-DXd* - Inflammatory BC HR-positive: endocrine immunogenicity 8 cycles therapy Invasive disease-free survival Overall survival Stratification factors Health-related quality of life HR status: ER and/or The T-DXd alone arm closed on March 13 2024, following Additional outcome PR-positive or negative Independent Data Monitoring Committee recommendation measures HER2 status: (IHC 3+ or The reasons were multifactorial, including a lower pCR rate, low likelihood Residual cancer burden (RCB) ISH+ in the absence of that T-DXd alone would be superior to ddAC-THP, and the timing of surgery IHC 3+ status) High-resolution computed tomography chest scans were performed every 6 weeks during treatment; if IL Dipneumonitis was suspected while receiving T-DXd. treatment was interrupted and a full investigation completed. Echocardiograms or multigated acquisition scans were performed during screening (<28 days prior to randomization). during treatment (<3 days before Cycle 5). and at end of treatment to assess left ventricular ejection fraction *5 mg/kg Q3W; pacitaxel (80 mg/m2 QW) trastuzumab (6 mg/kg Q3W) pertuzumab (840 mg loading dose followed by 420 mg Q3W): dexorubicin (60 mg/m2 Q2W) cyclophosphamide (600 mg/m2 Q2W): paclitaxel (80 mg/m3 QW) trastuzumab (8 mg/kg loading dose followed by 6 mg/kg Q3W) perfuzumab (840 mg loading dose followed by 420 mg Q3W): "the recommended window for surgery was 3-6 weeks following administration of the last dose of neoadjuvant study treatment administered as part of the patient's SOC at the investigator's discretion cT, clinical tumor stage; ER estrogen receptor; IHC. immunohistochemistry: ILD interstitial lung disease: ISH+ in situ hybridization-positive; N, nodal stage PR, progesterone receptor QXW every X weeks: T-DM1 trastuzumab emtansine ypT0/is ypN0 absence of invasive cancer in the breast and axillary nodes; ypT0 ypN0. absence of invasive and in-situ cancer in the breast and axillary nodes Nadia Harbeck, MD congress DESTINY-Breast11 BERLIN 2025 ESMO Content of this presentation is copyright and responsibility of the author. Permission is required for re-use. --- [Slide 2] pCR (ypTO/is ypN0): primary endpoint ITT population+ (primary endpoint) HR-positive HR-negative 16.1% 11.2% (95% CI 3.0, 28.8) Д9.1% 100 (95% CI 4.0, 18.3; P=0.003*) (95% CI 0.2, 17.9) 83.1 80 67.1 67.3 61.4 56.3 52.3 pCR (%)* 60 40 20 216/321 180/320 145/236 123/235 69/83 57/85 0 T-DXd-THP ddAC-THP T-DXd-THP ddAC-THP T-DXd-THP ddAC-THP Neoadjuvant T-DXd-THP demonstrated a statistically significant and clinically meaningful improvement in pCR vs ddAC-THP Improvement was observed in both the HR-positive and HR-negative subgroups For the ITT population, treatment effects were estimated by the difference in pCR with 95% Cls and P-values based on the stratified Miettinen and Nurminen's method, with strata weighting by sample size (ie Mantel-Haenszel weights) Patients with no valid records regarding pCR status for any reason were considered to be non-responders (including but not limited to withdrawal from the study progression of disease or death before surgery lack of surgical specimen or defined as not evaluable by the central pathologist) Subgroup analyses were unstratified "By blinded central review; 1pCR responders were defined as patients who only received randomized study treatment (at least one dose) and had pCR; two-sided P-value crossed the 0 03 prespecified boundary ITT. intent-to-treat Nadia Harbeck, MD DESTINY-Breast11 BERLIN 2025 ESMO congress Content of this presentation is copyright and responsibility of the author. Permission is required for re-use. --- [Slide 3] pCR (ypTO/is ypN0) by subgroups pCR rate, % (n/N) T-DXd-THP ddAC-THP ApCR, % (95% CI) (n=321) (n=320) All patients 67.3 (216/321) 56.3 (180/320) 11.2 (4.0, 18.3) <65 years 66.7 (188/282) 58.0 (167/288) 8.7 (0.7, 16.5) Age at baseline >65 years 71.8 (28/39) 40.6 (13/32) 31.2 (8.0, 51.4) Asia 66.5 (101/152) 56.6 (86/152) 9.9 (-1.1, 20.6) Western Europe 75.4 (52/69) 62.3 (48/77) 13.0 (-2.2, 27.5) Geographical region North America 74.4 (32/43) 36.6 (15/41) 37.8 (16.8, 55.7) Rest of world* 54.4 (31/57) 62.0 (31/50) -7.6 (-25.7, 11.2) Eastern Cooperative Oncology 0 68.7 (191/278) 55.7 (156/280) 13.0 (5.0, 20.9) Group performance status score 1 58.1 (25/43) 60.0 (24/40) -1.9 (-22.6, 19.1) Post 68.8 (86/125) 56.9 (87/153) 11.9 (0.5, 23.0) Menopausal status Pre 66.9 (123/184) 55.2 (90/163) 11.6 (1.4, 21.7) IHC 3+ 71.1 (199/280) 61.5 (174/283) 9.6 (1.8, 17.3) HER2 status Other 42.5 (17/40) 16.7 (6/36) 25.8 (5.2, 44.4) Positive 61.4 (145/236) 52.3 (123/235) 9.1 (0.2, 17.9) HR status Negative 83.1 (69/83) 67.1 (57/85) 16.1 (3.0, 28.8) American Joint Committee on II-IIIA 65.7 (163/248) 56.4 (146/259) 9.4 (0.9, 17.7) Cancer clinical stage IIIB-IIIC 72.2 (52/72) 55.7 (34/61) 16.5 (0.1, 32.3) NO 57.7 (15/26) 57.1 (20/35) 0.6 (-24.2, 24.8) Nodal status N+ 68.3 (196/287) 56.6 (159/281) 11.7 (3.8, 19.5) 60 40 20 0 -20 -40 Favors T-DXd-THP Favors ddAC-THP Improvement in pCR for T-DXd-THP vs ddAC-THP was observed across most pre-specified subgroups Size of circle is proportional to the total sample size in a subgroup "Brazil Bulgaria Peru Poland Russia and Saudi Arabia Nadia Harbeck, MD congress DESTINY-Breast11 BERLIN 2025 ESMO Content of this presentation is copyright and responsibility of the author. Permission is required for re-use. --- [Slide 4] Post-neoadjuvant treatments Patients with pCR* Patients without pCR* T-DXd-THP ddAC-THP T-DXd-THP ddAC-THP n (%) (n=226) (n=190) (n=95) (n=130) Any adjuvant treatment+ 224 (99.1) 187 (98.4) 85 (89.5) 107 (82.3) Any cytotoxic chemotherapy-containing regimen 13 (5.8) 11 (5.8) 10 (10.5) 12 (9.2) Any T-DM1-containing regimen 4 (1.8) 4 (2.1) 50 (52.6) 74 (56.9) Any trastuzumab-containing regimen 213 (94.2) 174 (91.6) 37 (38.9) 34 (26.2) Post-neoadjuvant treatments were generally well balanced between T-DXd-THP and ddAC-THP arms In both arms, more than half of patients without pCR received post-neoadjuvant T-DM1 Patients may have had at least one anti-cancer therapy and were counted once per therapy. "By local pCR result Texcludes patients who withdrew consent or did not receive surgery; also excludes treatment given in the metastatic setting Nadia Harbeck, MD DESTINY-Breast11 BERLIN 2025 ESMO congress Content of this presentation is copyright and responsibility of the author. Permission is required for re-use.
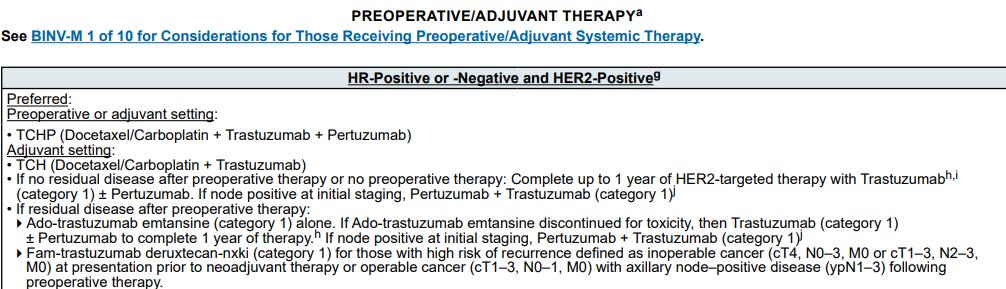
[Slide 1] PREOPERATIVE/ADJUVANT THERAPY See BINV-M 1 of 10 for Considerations for Those Receiving Preoperative/Adjuvant Systemic Therapy. HR-Positive or -Negative and HER2-Positive9 Preferred: Preoperative or adjuvant setting: TCHP (Docetaxel/Carboplatin + Trastuzumab + Pertuzumab) Adjuvant setting: TCH (Docetaxel/Carboplatin + Trastuzumab) If no residual disease after preoperative therapy or no preoperative therapy: Complete up to 1 year of HER2-targeted therapy with Trastuzumabh (category 1) + Pertuzumab. If node positive at initial staging, Pertuzumab + Trastuzumab (category 1) If residual disease after preoperative therapy: Ado-trastuzumab emtansine (category 1) alone. If Ado-trastuzumab emtansine discontinued for toxicity, then Trastuzumab (category 1) + Pertuzumab to complete 1 year of therapy. If node positive at initial staging, Pertuzumab + Trastuzumab (category 1)J Fam-trastuzumab deruxtecan-nxki (category 1) for those with high risk of recurrence defined as inoperable cancer (cT4, N0-3, M0 or cT1-3, N2-3, M0) at presentation prior to neoadjuvant therapy or operable cancer (cT1-3, N0-1, M0) with axillary node-positive disease (ypN1-3) following preoperative therapy.




[Slide 1] DESTINY-Breast11 study design A randomized, global, multicenter, open-label, Phase 3 study (NCT05113251) Data cutoff: March 12, 2025 n=321 T-DXd* THP Recommended Primary endpoint Patient population 4 + 4 cycles post-neoadjuvant pCR (ypTO/is ypN0) by blinded Previously untreated central review treatment per study HER2+ eBC protocol Secondary endpoints HR-positive or n=320 Randomized ddAC THPS HR-negative Surgery pCR: radiotherapy and pCR (ypTO ypN0) by blinded concomitant trastuzumab : central review 1:1:1 4 + 4 cycles High-risk defined as: pertuzumab for up to 1 year EFS >cT3 and NO-3 or No pCR: radiotherapy and Safety Nadia Harbeck cT0-4 and N1-3 T-DM1 for up to 14 cycles Pharmacokinetics and n=286 T-DXd* - Inflammatory BC HR-positive: endocrine immunogenicity DESTINY-Breast11: Neoadjuvant trastuzumab 8 cycles therapy Invasive disease-free survival Overall survival deruxtecan alone (T-DXd) or followed by Stratification factors Health-related quality of life paclitaxel + trastuzumab + pertuzumab (T-DXd- HR status: ER and/or The T-DXd alone arm closed on March 13 2024. following Additional outcome THP) vs SOC for high-risk HER2+ early breast PR-positive or negative Independent Data Monitoring Committee recommendation measures HER2 status: (IHC 3+ or The reasons were multifactorial, including a lower pCR rate, low likelihood cancer (eBC) Residual cancer burden (RCB) ISH+ in the absence of that T-DXd alone would be superior to ddAC-THP. and the timing of surgery IHC 3+ status) High resolution computed tomography chest scans were performed every works during treatment; Dipneumonitis was suspected while receiving T DXd. treatment was interrupted and full investigation completed chocardiograms or multigated acquisition scans were performed during screening (+28 days prior to during treatment (<) days before Cycle 5), and at end of to assess left ventricular ejection fraction mgkg Q3W pacitaxel 80 mg/m2 QW) restruzumab mgkg Q3W) perfuzumab (840 mg loading dose followed 420 mg Q3W): doxonubicin 60 mg/m3 Q2W) clophosphamide (600 mg/ml Q2W) pacitaxel (B) mg/m2 QW) trasturumab mgkg loading dose followed mg kg perfuzumab 540 mg loading dose followed by 420 mg Q3W) the recommended window for surgery was weeks following administration the last dose of neceduvant study treatment administered as part the patient's SOC the investigator discretion et clinical tumor I I ER estrogen I IHC I ILD interstitial lung disease ISH+ in situ hybridization-positive N modal stage PR progesterone receptor QXW every weeks T-DM1 trasturumab emtansine Dis ypNo absence of invasive cancer in the treast and accilary nodes ypTo yphis absence of invasive and in-situ cancer in the breast and axillary nodes Nadia Harbeck, MD congress DESTINY-Breast11 ESMO Content of this presentation is copyright and responsibility of the author. Permission is required for re-use. --- [Slide 2] pCR (ypTO/is ypN0): primary endpoint ITT population+ (primary endpoint) HR-positive HR-negative 16.1% 11.2% (95% CI 3.0, 28.8) Д9.1% 100 (95% CI 4.0, 18.3; P=0.003*) (95% CI 0.2, 17.9) 83.1 80 67.1 67.3 61.4 56.3 52.3 pCR (%)* 60 40 20 216/321 180/320 145/236 123/235 69/83 57/85 0 T-DXd-THP ddAC-THP T-DXd-THP ddAC-THP T-DXd-THP ddAC-THP Neoadjuvant T-DXd-THP demonstrated a statistically significant and clinically meaningful improvement in pCR vs ddAC-THP Improvement was observed in both the HR-positive and HR-negative subgroups For the ITT population, treatment effects were estimated by the difference in pCR with 95% Cls and P-values based on the stratified Miettinen and Nurminen's method, with strata weighting by sample size (ie Mantel-Haenszel weights) Patients with no valid records regarding pCR status for any reason were considered to be non-responders (including but not limited to withdrawal from the study progression of disease or death before surgery lack of surgical specimen or defined as not evaluable by the central pathologist) Subgroup analyses were unstratified "By blinded central review 1pCR responders were defined as patients who only received randomized study treatment (at least one dose) and had pCR two-sided P-value crossed the 0.03 prespecified boundary ITT intent-to-treat Nadia Harbeck, MD congress DESTINY-Breast11 ESMO Content of this presentation is copyright and responsibility of the author. Permission is required for re-use. --- [Slide 3] T-DXd alone arm: efficacy summary On March 13, 2024, the T-DXd alone arm closed following Independent Data Monitoring Committee recommendation.* Patients who were still receiving T-DXd alone could remain on therapy or immediately switch to local SOC pCR rate EFS 1.0 T-DXd ddAC-THP 94.4% % (n=286) (n=320) (95% CI 90.5, 96.7) EFS events Primary analysis 15/286 Switch to local SOC classified as non-pCR pCR+ 43.0 56.3 Probability of EFS 0.9 93.1% EFS events (95% CI 88.7, 95.8) 18/320 Hazard ratio 0.82 A (95% CI) -13.2 (-20.8, -5.4) (95% CI 0.41, 1.62) Prespecified supplementary analysis At data cutoff (March 12, 2025), Switch to local SOC not automatically classified as non-pCR 0.8 EFS event maturity was 5.4% pCRt 51.4 57.2 0 0 3 6 9 12 15 18 21 24 27 30 33 36 39 Number of A (95% CI) -5.8 (-13.4, 1.9) patients at risk Time from randomization (months) T-DXd alone 286 280 276 271 240 208 199 175 134 95 43 14 2 0 ddAC-THP 320 303 296 285 231 199 187 163 124 72 35 14 1 0 T-DXd alone showed inferior but robust pCR compared with the five-agent ddAC-THP EFS data were similar for T-DXd alone and ddAC-THP Treatment effects were estimated by the difference in pCR with 95% Cls based on the stratified Miettinen and Nurminen's method, with strata weighting by sample size (ie Mantel-Haenszel weights). Median duration of follow up was 24.9 months (T-DXd) and 23.6 months (ddAC-THP) Analyses are reported in the ITT population "The reasons were multifactorial including 5 lower pCR rate, low likelihood that T-DXd alone would be superior to ddAC-THP and the timing of surgery; by blinded central review Nadia Harbeck, MD congress DESTINY-Breast11 BERLIN 2025 ESMO Content of this presentation is copyright and responsibility of the author. Permission is required for re-use. --- [Slide 4] Conclusions In DESTINY-Breast11, T-DXd-THP showed the highest reported pCR rate in pCR rate HER2+ eBC for a registrational study in the neoadjuvant setting, despite a high prevalence of HR-positive disease and a high-risk population 67.3% T-DXd-THP showed a statistically significant and clinically meaningful improvement More than two thirds in pCR rate VS ddAC-THP: 11.2% (95% CI 4.0, 18.3) of patients in the - pCR benefit for T-DXd-THP VS ddAC-THP was independent of HR status and T-DXd-THP arm disease stage had a pCR An early positive trend in EFS was observed, favoring T-DXd-THP vs ddAC-THP HR-positive: 61.4% - Hazard ratio: 0.56 (95% CI 0.26, 1.17) HR-negative: 83.1% The safety profile of T-DXd-THP was favorable vs ddAC-THP - Lower rates of Grade ≥3 AEs, serious AEs, and AEs leading to dose interruptions - Lower rates of hematological AEs, left-ventricular dysfunction, and fatigue - ILD rates were low and similar between arms DESTINY-Breast11 results support T-DXd-THP as a more effective and less toxic neoadjuvant treatment compared with ddAC-THP, and it may become a preferred regimen for patients with high-risk HER2+ eBC "Historical pCR rates (defined by ypT0/is ypN0) from other registrational studies for neoadjuvant SOC treatments in HER2+ eBC ranged from 39 3% to 62 7% and HR positive prevalence ranged from 46 7% to 62 4%¹-¹ 1. Huober J. et al J Clin Oncol 2022:40 2946-2956;2 Hurvitz SA et al Lancet Oncol 2018,19.115-126:3 Gianni L, et al Lancet Oncol 2012:13:25-32 Nadia Harbeck, MD congress DESTINY-Breast11 2025 ESMO Content of this presentation is copyright and responsibility of the author. Permission is required for re-use.




[Slide 1 — SABCS 2025 Conclusions slide]
In DESTINY-Breast11, the safety profile of T-DXd-THP was manageable and less toxic than ddAC-THP.
Rates of adjudicated drug-related ILD/pneumonitis were low across arms, and there were fewer Grade ≥3 events with T-DXd-THP than ddAC-THP.
- Rates remained stable (T-DXd-THP) and were higher (ddAC-THP) in the THP phase (Cycles 5-8) vs Cycles 1-4.
Rates of overall and Grade ≥3 left ventricular dysfunction were lower with T-DXd-THP than ddAC-THP.
- There were no events of cardiac failure in the T-DXd-containing arms.
Rates of nausea and vomiting were higher with T-DXd-THP than ddAC-THP, highlighting the importance of following guideline recommendations for antiemetics; however, events were generally low grade.
Rates of hematologic toxicities were lower in the T-DXd-THP arm than the ddAC-THP arm.
Most peripheral neuropathy events occurred during the THP phase (Cycles 5-8) and were non-serious and generally low grade.
DESTINY-Breast11 safety results support T-DXd-THP as a potential neoadjuvant treatment option for patients with high-risk HER2+ eBC.
[Slide 2 — Adjudicated drug-related ILD/pneumonitis: discontinuations, interruptions, reductions, and SAEs]
T-DXd-THP ddAC-THP T-DXd
(N=320) (N=312) (N=283)
Leading to treatment discontinuation: 6 (1.9%) 7 (2.2%) 9 (3.2%)
Grade 1 0 0 2 (0.7%)
Grade 2 5 (1.6%) 4 (1.3%) 7 (2.5%)
Grade 3 0 3 (1.0%) 0
Grade 5 1 (0.3%) 0* 0
Leading to treatment interruption: 3 (0.9%) 6 (1.9%) 3 (1.1%)
Grade 1 1 (0.3%) 2 (0.6%) 0
Grade 2 1 (0.3%) 0 3 (1.1%)
Grade 3 1 (0.3%) 4 (1.3%) 0
Leading to dose reduction 0 0 0
SAE 2 (0.6%) 9 (2.9%) 1 (0.4%)
*One Grade 5 event in ddAC-THP arm, however, the patient died prior to decision to discontinue treatment.
Incidence of treatment discontinuations and interruptions due to ILD/pneumonitis were low across treatments, with no dose reductions; more SAEs in the ddAC-THP arm vs T-DXd-THP and T-DXd arms.
[Slide 3 — DESTINY-Breast 05 (companion presentation) Conclusions]
IDFS improvement with T-DXd compared with T-DM1 was consistent across subgroups regardless of: prior NACT (anthracyclines or platinum-based therapy); HER2 status (IHC 3+ or HER2 IHC 2+/1+ and ISH+).
Timing of adjuvant RT did not impact incidence or severity of adjudicated drug-related ILD.
Most patients who experienced ILD had recovered or were recovering by DCO.
Overall, T-DXd demonstrated a generally manageable safety profile with both sequential and concurrent adjuvant RT.
T-DXd over T-DM1 in the post-neoadjuvant HER2+ eBC residual invasive disease setting, supporting T-DXd as a potential new standard-of-care.
Source: SABCS 2025 (Dec 9-12, 2025) — Loibl S, Curigliano G, presenters. Tweet capture via @hoperugo (5,704 imp).DESTINY-Breast11 Top Tweets


Top Discussion Threads
Highest-engagement tweets about this trial, ranked by KOL discussant count (replies + quote-tweets). Replies in green, quote-tweets in blue. Wall Street, stock-promo, and non-substantive replies excluded.
Ask any breast oncologist today, and they’ll tell you they prefer anthracycline-free regimens in HER2-positive breast cancer — and that anthracyclines don’t improve response rates. So how did we accept a control arm containing anthracyclines in the DESTINY-Breast11 trial, which h

Anthracylines aren't so much of a problem if delivered with pre|cision technology. #silentinthebloodstream #AVCT #Avacta

As long as physicians receive direct or indirect payments from industry for clinical trial participation, true scientific equipoise is impossible. What did you expect? In such a system, research ethics can’t flourish dec

I’m glad someone like you has the courage to point this out. I was a sub investigator and didn’t have equipoise for these arms so didn’t enroll anyone—and I got nagged constantly about it because it costs a lot of money

Anthracycline-containing arms are still standard.

Would you avoid anthracyclines for very large tumours / inoperable and high nodal risk as well ?

Not harsh at all. I can think of several late game decisions by regulators refuse to consider a trial that did not assess the standard of care

Indeed. Aldoxorubicin’s P2 trial was intentionally ‘played’ to support the progression into P3, only for it to fall spectacularly. The safety and effectiveness of the drug was clear from the P1 data. Waste of time, mon

100%! Thank you for pointing this out!

Of course standard is TCH+P so this was due to achieving better score. It is similar to last year Niagara where neoadjuvant control chemotherapy was GC not M-VAC
Just a joke Yakup 😊

Totally agree, I really feel sad when someone uses 4 AC against the 4 DC in early breast cancer.

in this context, among patients with Top2-alpha mutations, aren't anthracyclines more effective than taxanes? If no clinical literature, feel free to look into preclinical literature. Thanks.

IT IS NOT HARSH,YOU HAVE CALLED A SPADE….

Anthracyclines were included because this reflected what was being offered in many countries. Not all countries have access to non-Anthracyclines regimens such as TCHP!
Harbeck is very unethical Indeed. She is also hiding in adaptcycle trial that ribociclib triggers much more toxic events than chemo over thé first 6 months: hématologic and hepatic toxicities. She state the reverse And s
Indeed, but the investigators always treat us as Guinea pigs; especially in the ribolaris trial where they force their victims to pursue exposure to ribociclib against the décision of the French authorities! To get paid






 +4
+4
DB-11 abstract just released. In high-risk (≥T3, N+, or IBC) HER2+ eBC, neoadjuvant T-DXd-THP outperformed ddAC-THP (pCR rate 67% vs 56%, p=0.003), with reduction in cardiotoxicity (LVD 1.9 vs 9%) and low rate of ILD (4.4 vs 5.1%). The last nail in the coffin for anthracyclines.

The only time I use anthracyclines in Her2 positive disease is pregnancy!!!
Glad to see these results however I don’t think Anthracyclines are going away quite yet! Still useful in TNBC and with regards to this patient population many parts of the world will not have access to T-DXd-THP due to c






 +4
+4
#ESMO25 DESTINY-Breast11-Positive✅ but Current standard: 6× THP or TCbHP, already short & anthracycline-free. pCR ↑ 11% is notable — but if residual disease remains, then what? Will we give T-DM1, which is weaker than T-DXd? Or extrapolate from DB-05 and use adjuvant T-DXd ht

More data needed regarding non PCR , is TDM1 is the right choice as we know that TDXD is outperforming it also in this situation?

It may come down to initial risk (large node positive tumors) and we need other tools like HER2DX pCR to potentially help choose.

@_NachoG12

A new era in early HER2+ breast cancer. At #ESMO25, T-DXd outperformed T-DM1 in the adjuvant DESTINY-Breast05 and Surpassed standard ddAC-THP in the neoadjuvant DESTINY-Breast11 Bringing ADCs into the curative setting. Lung monitoring remains essential. #BreastCancer #TDXd h







 +4
+4
📌 ✨DESTINY-Breast11✨ Neoadjuvant trastuzumab deruxtecan alone or followed by paclitaxel + trastuzumab + pertuzumab vs SOC for high-risk HER2+ early breast cancer @Prof_Nadia_H Presidential Symposium #ESMO25 @OncoAlert #OncoAlertAF https://t.co/Kn5FkVro6O






 +4
+4
@dr_yakupergun @SuyogCancer @AnisToumeh @drsarahsam @stolaney1 @OncBrothers @oncologician @PTarantinoMD @JAMouabbi @DrSGraff Go with Tolaney approach to spare unnecessary Rx. https://t.co/C4lvMqBK0t








About the DESTINY-Breast11 Trial
DESTINY-Breast11 is a Phase 3 multicentre, open-label randomized trial that evaluates neoadjuvant trastuzumab deruxtecan (T-DXd) followed by paclitaxel + trastuzumab + pertuzumab (T-DXd-THP) versus standard-of-care dose-dense doxorubicin/cyclophosphamide followed by THP (ddAC-THP) in patients with previously untreated, high-risk HER2-positive early breast cancer. The primary pCR endpoint analysis was reported at ESMO 2025 (T-DXd-THP 67.3% vs ddAC-THP 56.3%, Δ11.2%, p=0.003). At ESMO Breast 2026, an updated RCB (Residual Cancer Burden) analysis was presented, showing higher RCB-0+I rates with T-DXd-THP across all subgroups, deepening the prognostic case for the regimen.
FDA Approval — Enhertu (T-DXd) in HER2+ Early Breast Cancer
KOL Reactions on FDA Approval (May 15-16, 2026)
The HER2+ breast cancer community greeted the dual approval as a clear standard-of-care shift. Top voices, ranked by impressions:
- @PTarantinoMD (Paolo Tarantino) · 14,829 imp · 64 likes · 24 RT · 2026-05-15:
“Since the first phase 1 trial of T-DXd, it was clear that this drug could be transformative when taken to the curative setting. Today, the FDA approved T-DXd for the neoadjuvant or adjuvant treatment of HER2+ eBC, marking a major advancement in the field.” - @drsarahsam (Dr Sarah Sammons) · 3,323 imp · 42 likes · 15 RT · 2026-05-15:
“Major FDA news today for early-stage HER2+ breast cancer. T-DXd approved for two separate indications: neoadjuvant Stage II/III disease (T-DXd x4 followed by THP x4), and adjuvant treatment for residual invasive disease after neoadjuvant HER2-targeted therapy. The data are” - @ErikaHamilton9 (Erika Hamilton, MD, FASCO) · 2,634 imp · 53 likes · 17 RT · 2026-05-15:
“Wow- big month for breast approvals so far...and it's only May 15th! #TDXd approved for neoadjuvant and adjuvant HER-2+ #bcsm Our @US_FDA breast colleagues have been very busy, thank you!” - @OncBrothers (Oncology Brothers) · 2,554 imp · 39 likes · 16 RT · 2026-05-15:
“TDXd now @US_FDA ✅ in neoadjuvant and adjuvant high risk residual HER2+ breast cancer based off DESTINYBreast05 and DESTINYBreast11: - ⬆️ pCR & iDFS w/ TDXd - Timings of RT did NOT impact the incidence or severity of ILD - New Soc for high risk disease! #bcsm #OncTwitter” - @DrChoueiri (Toni Choueiri, MD) · 1,965 imp · 22 likes · 12 RT · 2026-05-15:
“JUST IN: @FDA approves Neoadjuvant Trastuzumab deruxtecan (TdXD) for Her-2 + breast cancer and post residual disease , based upon Destiny breast 011/05 trials.” - @SuyogCancer (Dr Amol Akhade) · 544 imp · 12 likes · 3 RT · 2026-05-15:
“Trastuzumab deruxtecan gets @US_FDA approval for NACT and for post NACT residual disease , based upon Destiny breast 011 and 05 trials . Expected approval especially for DB 05 setting . @stolaney1 @ErikaHamilton9 @dr_yakupergun @PTarantinoMD @elmayermd @OncoAlert” - @dr_yakupergun (Yakup Ergün) · 467 imp · 6 likes · 6 RT · 2026-05-16:
“In 1998, the approval of trastuzumab began to change the poor prognosis of HER2-positive breast cancer for the better. Over the following nearly 30 years, anti-HER2 therapy evolved step by step: trastuzumab, pertuzumab, T-DM1, and now T-DXd. With the latest anti-HER2 ADC data,” - @OncoAlert (OncoAlert) · 317 imp · 12 likes · 8 RT · 2026-05-16:
“FDA Approval based on DESTINY-Breast11 and DESTINY-Breast05 in #BreastCancer The FDA approved fam-trastuzumab deruxtecan-nxki for two HER2-positive early-stage breast cancer indications: neoadjuvant therapy for Stage II/III disease followed by THP, and” - @DrRishabhOnco (Dr Rishabh Jain) · 173 imp · 5 likes · 3 RT · 2026-05-16:
“🚨 FDA expands the role of Enhertu in curative-intent HER2+ early breast cancer. AstraZeneca + Daiichi Sankyo’s trastuzumab deruxtecan is now approved in the US in BOTH: 🔹 Neoadjuvant setting (DESTINY-Breast11) 🔹 Adjuvant residual disease setting (DESTINY-Breast05) Key data”
Discussion Threads: TCHP vs T-DXd-THP Neoadjuvant SOC Debate (May 15, 2026)
Immediately after the FDA approval, a thread between Oncology Brothers, Bijoy Telivala, Paolo Tarantino, Stephanie Graff, and S Premji opened the practice-question:
- @OncBrothers (155 imp, 5/15): “I do think for that high risk residual disease, this is definitely the new SoC. But is this going to be used broadly in neoadjuvant settings??”
- @BijoyTelivala (43 imp, 5/15): “Suspect T-DXd followed by THP will be the chosen regimen based on Destiny-Breast 11.”
- @OncBrothers (30 imp, 5/15): “Inflammatory disease… absolutely! Bulky nodes/N2… yes!! But for node negative… I feel TCHP might do a good job (especially when we have TDXd in adjuvant settings and this ends up declaring more aggressive disease than what I was anticipating), no?”
- @BijoyTelivala (25 imp, 5/15): “Breast cancer and Myeloma — 2 diseases where treatment paradigms change on surrogate points very quickly. I will wait to hear from experts why TCHP was not an arm in the trial?”
Open clinical questions surfacing: (1) Will T-DXd-THP replace TCHP universally, or only for high-risk subgroups (inflammatory, N2, bulky disease)? (2) For node-negative disease, is TCHP still preferred — preserving T-DXd for adjuvant residual disease? (3) Comparative trial vs TCHP arm absent.
DESTINY-Breast11 Methodology & Results
Population: Previously untreated HER2-positive early breast cancer with high-risk features: clinical stage T3+ with N0-3, OR cT0-4 with N1-3, OR inflammatory breast cancer. Both HR+ and HR- enrolled. 81.3% IHC 3+; remainder 'other' (IHC 2+/ISH+ or 1+/ISH+).
Interventions: T-DXd-THP arm: T-DXd 5.4 mg/kg every 3 weeks × 4 cycles → paclitaxel 80 mg/m² weekly × 12 + trastuzumab + pertuzumab. Control: ddAC × 4 cycles (doxorubicin 60 mg/m² + cyclophosphamide 600 mg/m² Q2W) → paclitaxel + trastuzumab + pertuzumab. Adjuvant T-DM1 or T-DXd per standard practice based on residual disease.
Endpoints: Primary: pCR (ypT0/is N0) by ITT. Secondary: EFS, RCB distribution (analysis presented at ESMO Breast 2026), DFS, OS, safety. Translational: HER2 IHC subgroup analysis, biomarker correlatives.
Efficacy — pCR 67.3% vs 56.3% (Δ11.2%, p=0.003) · RCB-0+I 81.3% vs 69.1%
Primary endpoint: T-DXd-THP achieved pCR in 67.3% vs 56.3% with ddAC-THP (Δ11.2%, 95% CI 4.0-18.3; p=0.003). Benefit consistent across HR status (HR+: 61.4% vs 52.3%, Δ9.1%; HR-: 83.1% vs 67.1%, Δ16.1%). At ESMO Breast 2026, RCB-0+I rates were higher with T-DXd-THP across all subgroups: 81.3% vs 69.1% overall (Δ12.2%). By disease stage: Stage II 83.6% vs 71.7%; Stage III 78.9% vs 66.0%. By HER2 IHC subgroup: 3+ 82.9% vs 74.2%; "other" (IHC 2+/ISH+ or 1+/ISH+) 72.5% vs 30.6% — striking 41.9-point absolute differential in this lower-HER2-expression subgroup. Continuous RCB index favours T-DXd-THP (p=0.0059). Early EFS trend favours T-DXd-THP (HR 0.56, 95% CI 0.26-1.17) at ~24 months follow-up — immature.
Safety & Tolerability — Better safety profile than ddAC-THP: G≥3 AEs 37.5% vs 55.8%; all-grade LV dysfunction 1.3% vs 6.1%
T-DXd-THP demonstrated a markedly better safety profile than ddAC-THP: grade ≥3 AEs 37.5% vs 55.8%; serious AEs 10.6% vs 20.2%; AE-related dose interruptions 37.8% vs 54.5%. Left ventricular dysfunction was less frequent with T-DXd-THP: all-grade 1.3% vs 6.1%; Grade ≥3 0.3% vs 1.9% (no Grade 5 events) [Annals Oct 2025]. ILD/pneumonitis was infrequent and similar between arms (4.4% vs 5.1%). Three treatment-related deaths total: 1 in T-DXd-THP arm (drug-related pneumonitis); 2 in ddAC-THP arm (drug-related bacterial encephalitis + drug-related pneumonitis). One Grade 5 ILD/pneumonitis event in each arm [Annals Oct 2025]. Importantly, no AE prevented surgical intervention.
Clinical Implications
Paolo Tarantino voiced “high expectations from #CompassHER2pCR and #DESTINYBreast11 to expand our anthracycline-free treatment options… for a future where most patients can be cured with less alopecia, fatigue, neutropenia, cardiotoxicity and secondary leukemias.” Erika Hamilton called it “the FIRST positive T-DXd trial in the early-stage setting.” Yakup Ergün dissented: “Ask any breast oncologist today, and they’ll tell you they prefer anthracycline-free regimens — and that anthracyclines don’t improve response rates,” questioning the ddAC-THP control. Gaia Griguolo flagged three open questions: how T-DXd-THP compares to TCbHP, whether T-DM1 or T-DXd is better post-neoadjuvant in residual disease, and whether low ILD rates reflect short treatment duration vs strict surveillance. Hope Rugo highlighted SABCS25 safety data (Sybille Loibl) showing no ILD increase when T-DXd is given through adjuvant RT. Madeleine Armstrong (Apex Onco), writing across the paired DB-05 and DB-11 ESMO 2025 readouts, flagged ILD vigilance: “Enhertu’s perioperative Destiny beckons, but watch out for ILD.” Stephanie Graff polled the overlap problem with DESTINY-Breast05 (“what are we doing in the overlapping population?”). Luca Reccoschi noted that 53% of voters would opt for TCHP→T-DXd sequencing while awaiting further DB-11 and DB-05 updates.
DESTINY-Breast11 FAQ
What is the DESTINY-Breast11 trial?
DESTINY-Breast11 is a Phase 3, multicentre, open-label, randomized trial (NCT05113251) of neoadjuvant trastuzumab deruxtecan (T-DXd) followed by paclitaxel + trastuzumab + pertuzumab (T-DXd-THP) versus dose-dense doxorubicin/cyclophosphamide followed by THP (ddAC-THP) in previously untreated, high-risk HER2-positive early breast cancer.
Is neoadjuvant T-DXd (Enhertu) FDA approved?
Yes. On May 15, 2026 the FDA approved Enhertu as neoadjuvant treatment of adults with HER2-positive (IHC 3+ or ISH+) Stage II or III breast cancer, followed by a taxane, trastuzumab, and pertuzumab (THP), based on DESTINY-Breast11. The same approval action also covers adjuvant Enhertu for HER2+ residual disease (DESTINY-Breast05).
What were the DESTINY-Breast11 pCR results?
The primary pathologic complete response (pCR) rate was 67.3% with neoadjuvant T-DXd-THP versus 56.3% with ddAC-THP (an 11.2 percentage-point improvement; p=0.003), reported at ESMO 2025.
What did the updated Residual Cancer Burden analysis show?
At ESMO Breast 2026, an updated Residual Cancer Burden analysis showed RCB-0+I rates of 81.3% with T-DXd-THP versus 69.1% with ddAC-THP, reinforcing the primary pCR result.
How did the safety of T-DXd-THP compare with ddAC-THP?
Neoadjuvant T-DXd-THP had a markedly better safety profile than ddAC-THP: grade >=3 adverse events 37.5% versus 55.8%, serious AEs 10.6% versus 20.2%, and all-grade left-ventricular dysfunction 1.3% versus 6.1%.