DESTINY-Breast09 is a Phase 3 trial of first-line trastuzumab deruxtecan (T-DXd, Enhertu) plus pertuzumab versus the standard taxane + trastuzumab + pertuzumab (THP) regimen in HER2-positive metastatic breast cancer. The T-DXd combination improved median PFS to 40.7 vs 26.9 months (HR 0.56; p<0.0001), supporting FDA approval on December 15, 2025. Sponsor: Daiichi Sankyo / AstraZeneca.
Discover KOL Sentiment on DESTINY-Breast09 →Design — Phase 3, open-label; 1L T-DXd (Enhertu) + pertuzumab vs standard THP, HER2+ metastatic breast cancer (NCT04784715). (NEJM)
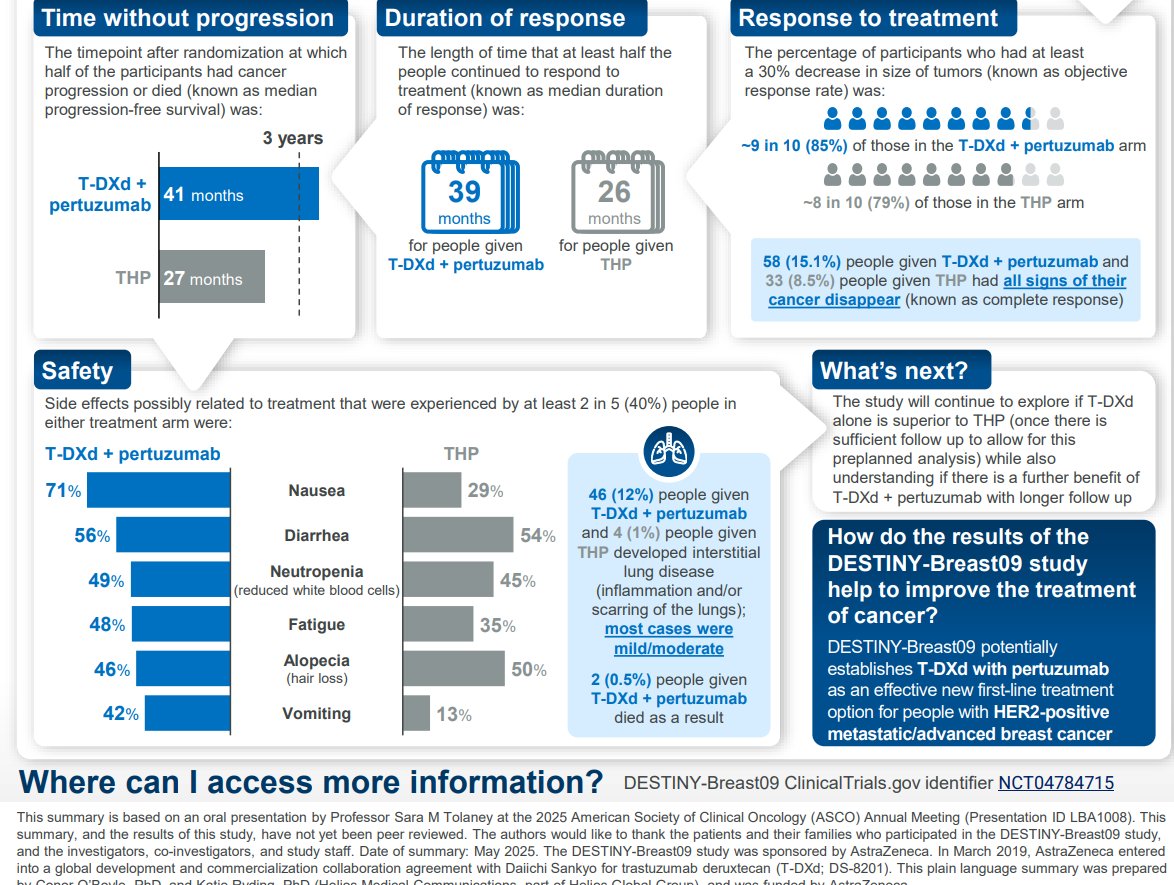
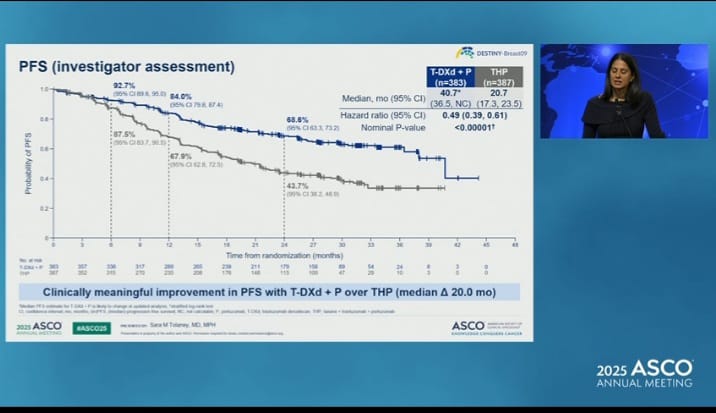
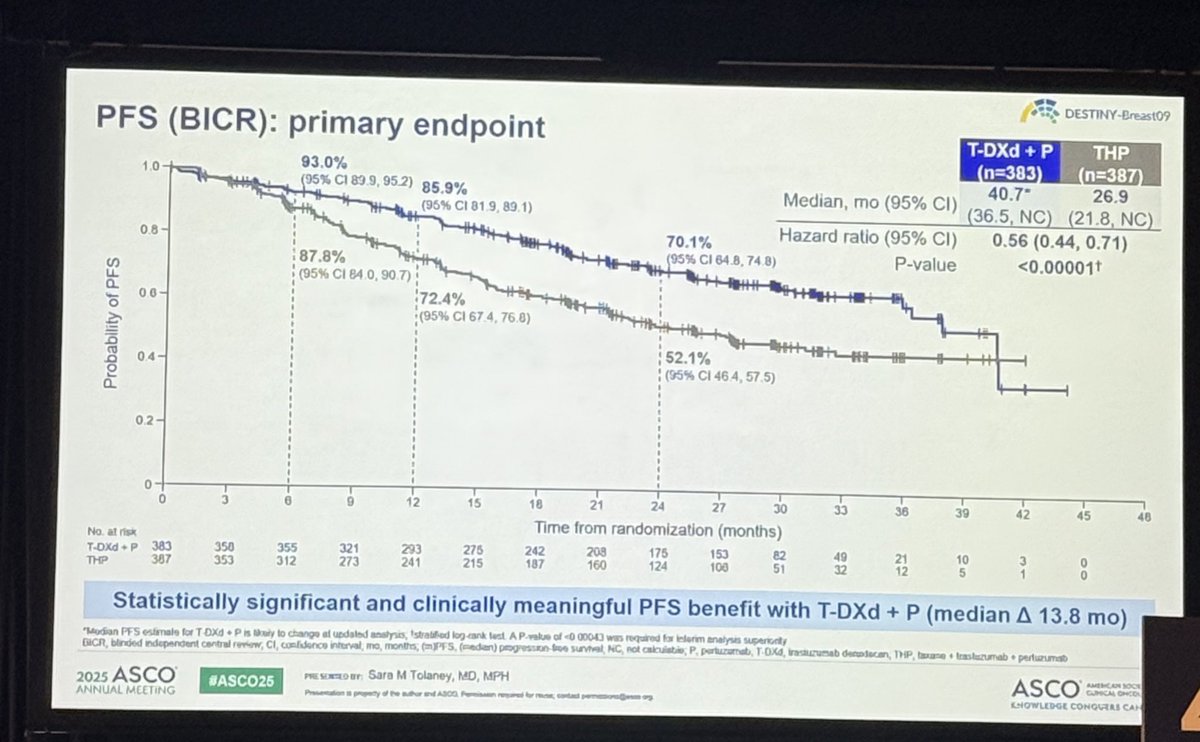
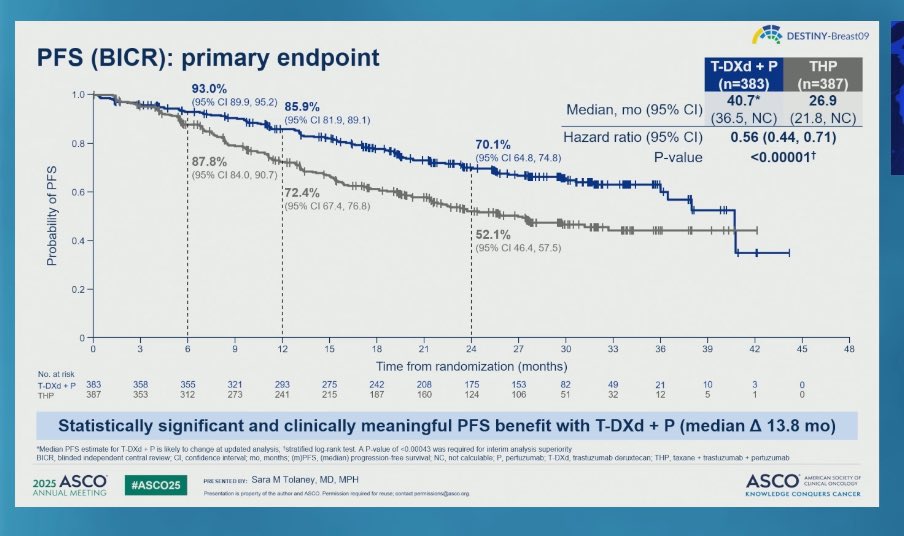
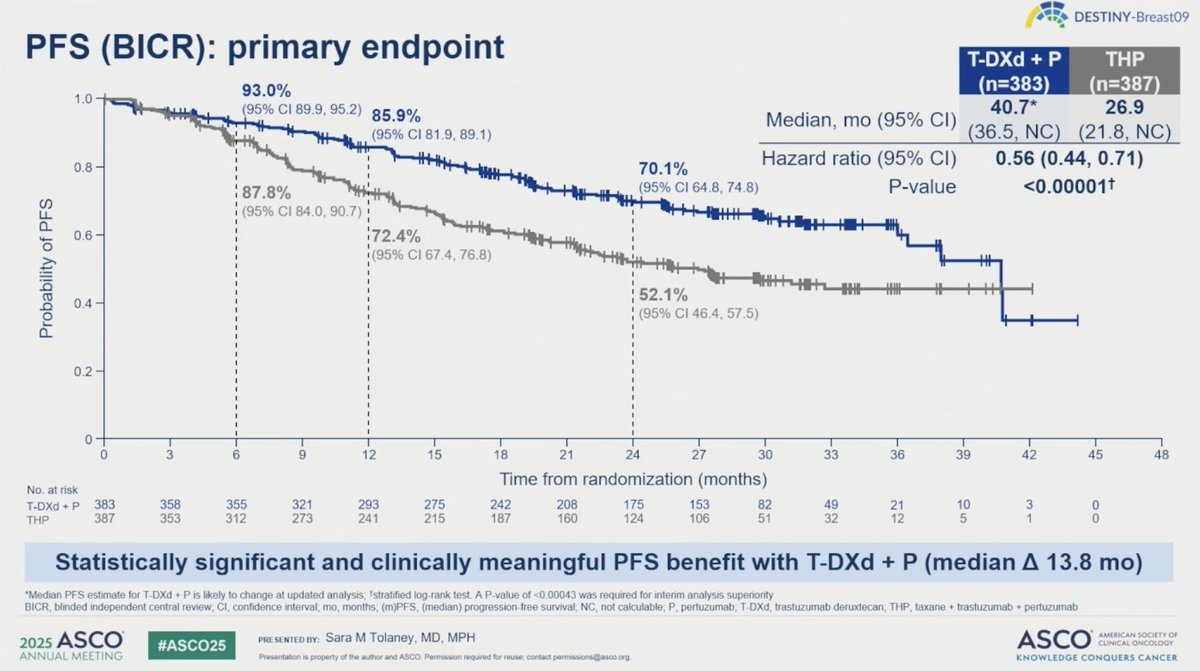
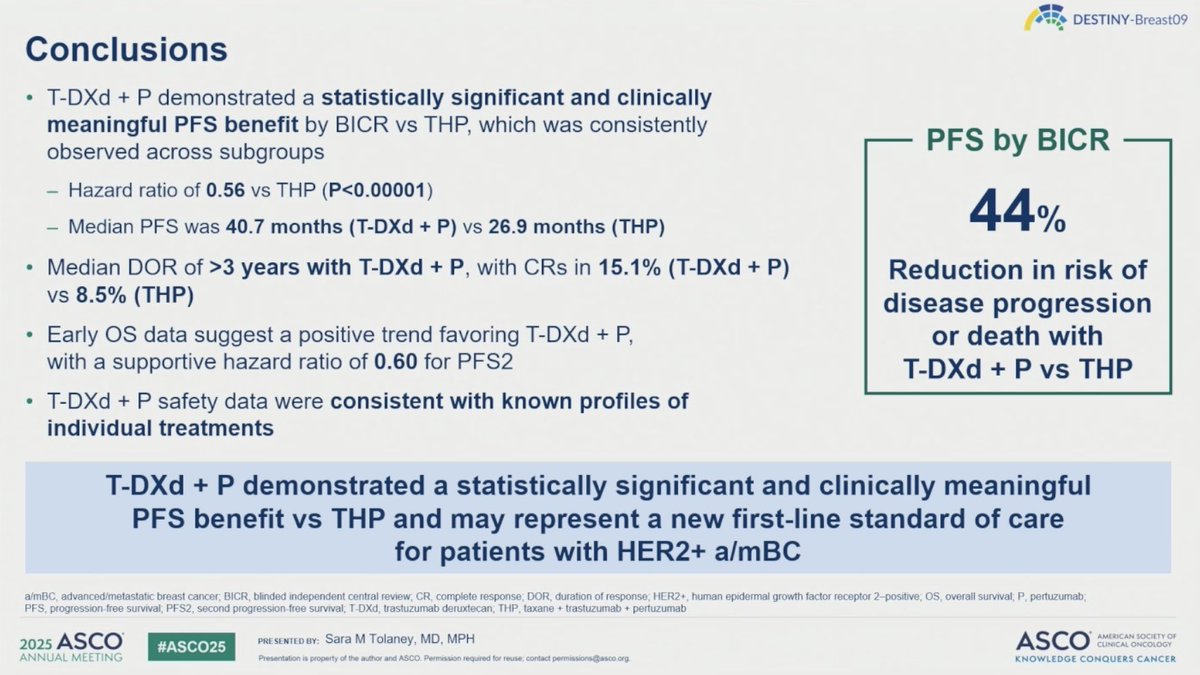
PFS (primary) — Median 40.7 vs 26.9 months; HR 0.56 (95% CI 0.44-0.71; p<0.0001) — 44% reduction, benefit regardless of HR status. (NEJM)
Overall survival — Immature (16% maturity); early numerical trend favors T-DXd + pertuzumab (HR 0.84; 95% CI 0.59-1.19). (interim)
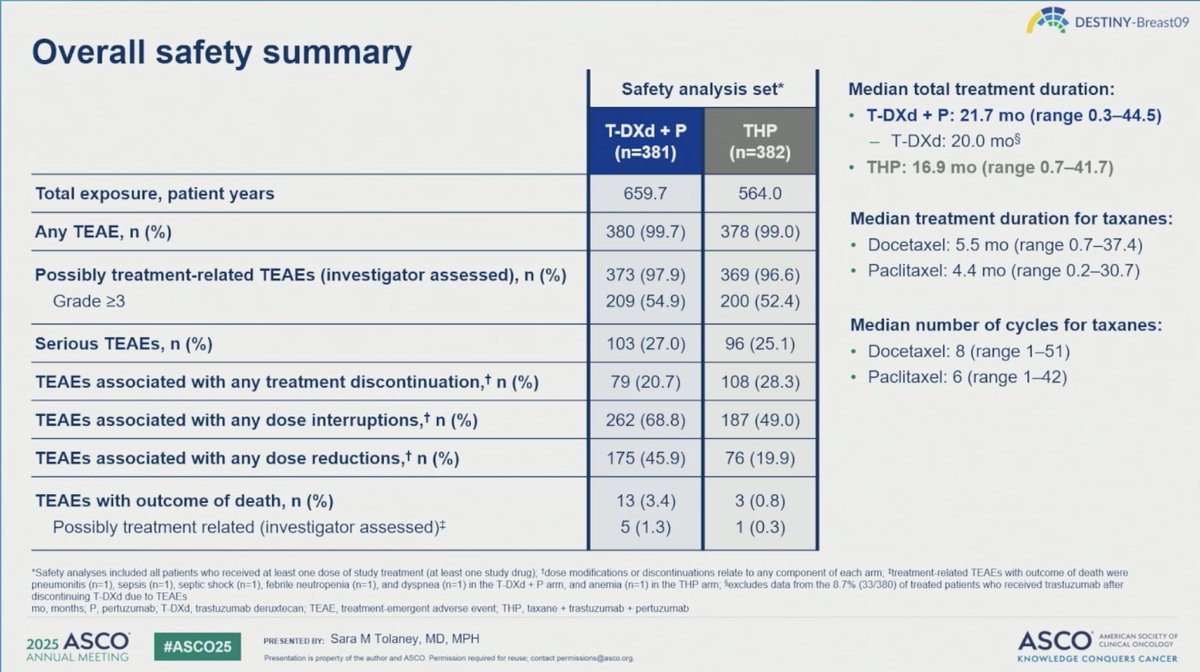
Safety — Adjudicated drug-related ILD/pneumonitis 12.1% (2 fatal, 0.5%); neutropenia 78% all-grade (29% Grade 3/4); nausea 75%. (NEJM)
Regulatory — FDA approved December 15, 2025 for 1L HER2+ metastatic breast cancer; PATHWAY (4B5) companion Dx co-approved. (FDA.gov)
Sponsor / Drug — Daiichi Sankyo / AstraZeneca; T-DXd (Enhertu) ADC + pertuzumab (Perjeta). (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.













Top 10 by impressions - click to view on X
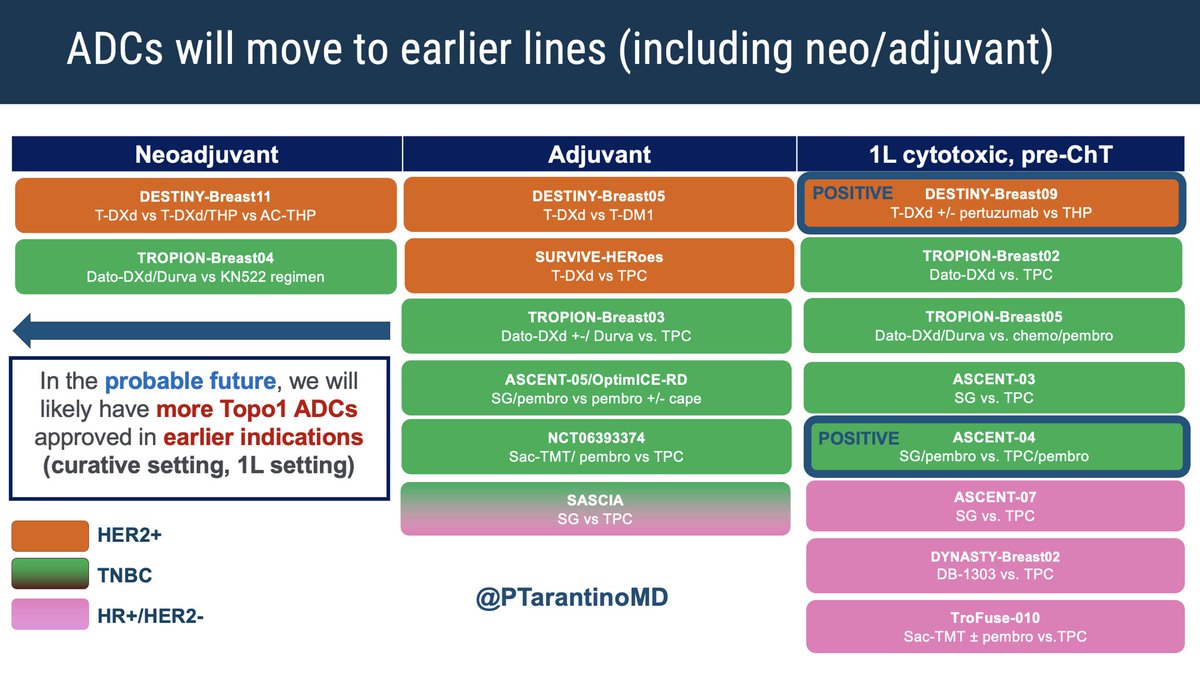
ADCs are rapidly moving to earlier line treatment for breast cancer. Will likely reach the (neo)adjuvant setting soon. Here’s a recap of key ADC phase 3 trials expected to shape practice in the...
< 2 wks to #ASCO25, here is a📝 of 🔑abstracts for general onc that could guide our SoC! - #ATOMIC - #MATTERHORN -...
Another money 💰 slide from #asco25 @ASCO . Treatment algorithm for HR +/ HER 2 -ve mBC @OncoAlert @medicalwatchBC
The curves everybody’s been waiting for. First line T-DXd + pertuzumab significantly prolonged PFS over THP for HER2+ MBC (40.7 vs 26.9 months, HR 0.56, p<0.001), doubled the rate of...
#OncTwitter #regulatory #bcsm 📣 #FDA has approved trastuzumab deruxtecan + pertuzumab for 1st-line tx of adults w/ HER2+...
When you have a packed @ASCO room at 7.30 am, you know that a change in practice is coming. #DESTINYBreast09 @stolaney1 #ASCO25 3 minutes to go

The #ASCO25 #OncoAlertTOP10 Abstracts in #BreastCancer These are some of our picks of TOP abstracts we look forward to be presented at the upcoming...
Destiny-Breast-09 will likely establish a new first-line therapy for HER2+ MBC. Here are my considerations going into #ASCO25 Patient population considerations: 1) De novo patients...
T-DXd + pertuzumab approved for 1st L HER-2+ #bcsm! Now for the debates around induction length, maintenance, re-induction etc. My opinion: I'll induce to...
Recent rationale in metastatic breast cancer for bringing ADCs into the 1st line has quoted very high 1st line attrition rates of patients not making it to second line. This study is likely more...
DESTINY-Breast09 is a clinical trial evaluating Trastuzumab deruxtecan (T-DXd) + pertuzumab in 1L HER2+ metastatic breast cancer. Sponsored by Daiichi Sankyo / AstraZeneca. KOL discussion spans multiple conferences with 106 tracked posts from 54 oncology opinion leaders generating 504.4K total impressions.
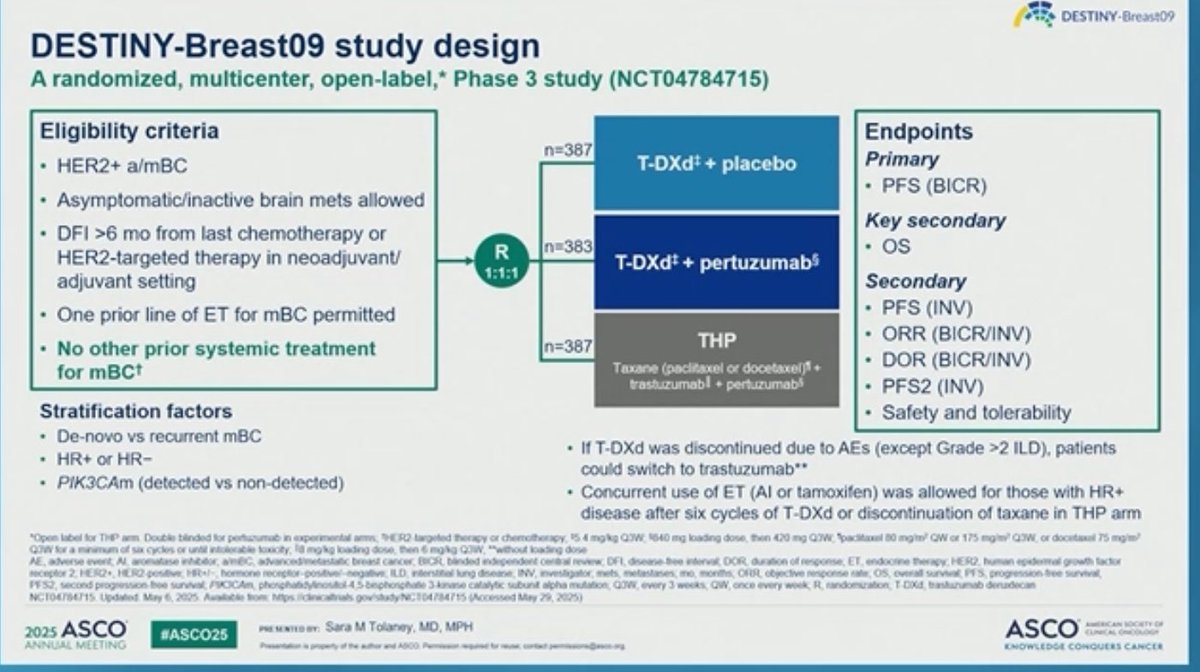
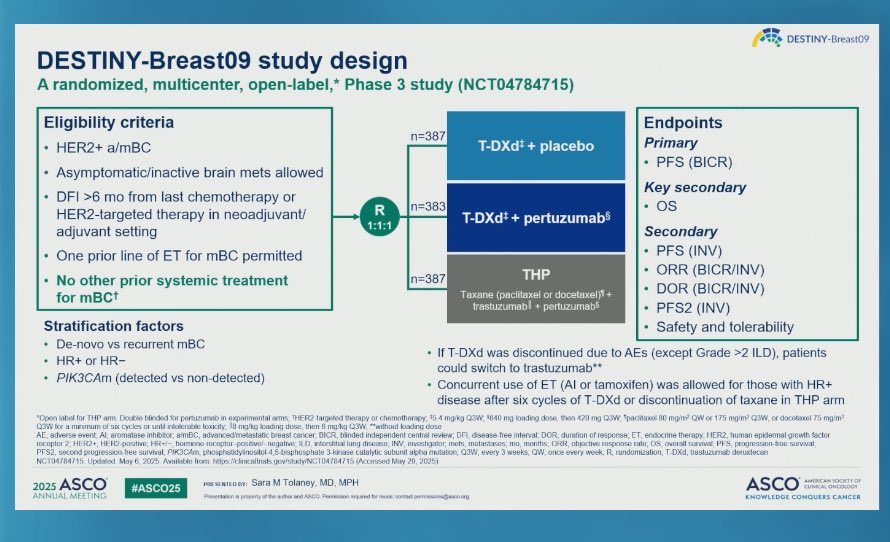
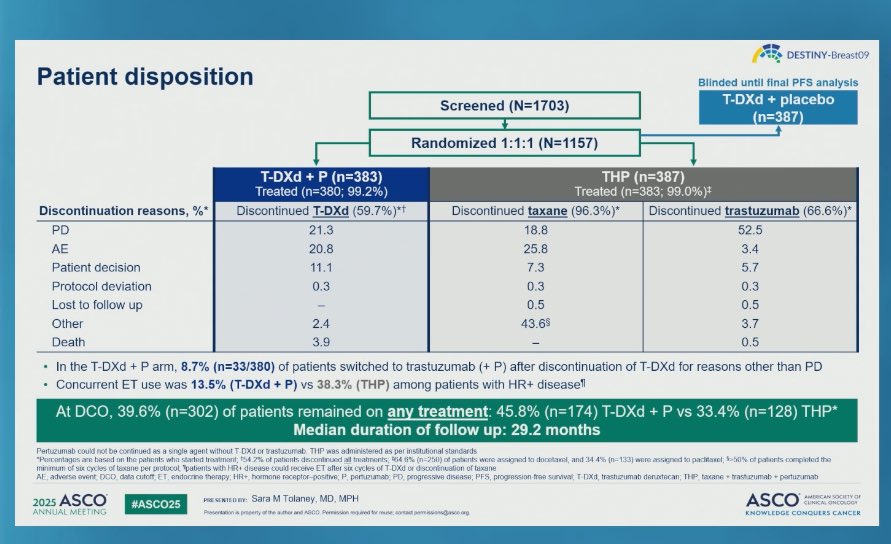
Phase 3, randomized (1:1:1), three-arm, multicenter trial comparing T-DXd (5.4 mg/kg) plus pertuzumab versus taxane plus trastuzumab plus pertuzumab (THP) in treatment-naive HER2-positive advanced/metastatic breast cancer.
Adults with HER2-positive (IHC 3+ or ISH+) unresectable or metastatic breast cancer with no prior chemotherapy or HER2-targeted therapy for advanced disease. A single prior line of endocrine therapy was permitted.
Fam-trastuzumab deruxtecan-nxki (Enhertu) 5.4 mg/kg IV every 3 weeks plus pertuzumab versus taxane (docetaxel or paclitaxel) plus trastuzumab plus pertuzumab (THP).
Primary: progression-free survival (PFS) by blinded independent central review (BICR). Key secondary: overall survival (OS), confirmed objective response rate (ORR).
T-DXd plus pertuzumab demonstrated a 44% reduction in risk of disease progression or death versus THP. Median PFS was 40.7 months (95% CI: 36.5-NE) versus 26.9 months (95% CI: 21.8-NE) (HR 0.56; 95% CI: 0.44-0.71; p<0.0001).
OS data remain immature (16% maturity). Early numerical trend favors T-DXd plus pertuzumab (HR 0.84; 95% CI: 0.59-1.19).
Adjudicated drug-related ILD/pneumonitis occurred in 12.1% of patients, including two fatal (Grade 5) events (0.5%). Neutropenia was common (78% all grades, 29% Grade 3/4). Nausea occurred in 75%. ILD was the leading cause of permanent discontinuation (6.6%).
DESTINY-Breast09 establishes T-DXd plus pertuzumab as a new first-line standard of care for HER2-positive metastatic breast cancer. FDA approved December 15, 2025. ILD risk and immature OS data remain areas of active debate.
DESTINY-Breast09 is a global, randomized, open-label Phase 3 trial (NCT04784715) in previously untreated (first-line) HER2-positive metastatic breast cancer comparing trastuzumab deruxtecan (T-DXd, Enhertu) plus pertuzumab versus the standard taxane + trastuzumab + pertuzumab (THP) regimen.
Yes. On December 15, 2025 the FDA approved Enhertu in combination with pertuzumab (Perjeta) for the first-line treatment of adults with unresectable or metastatic HER2-positive (IHC 3+ or ISH+) breast cancer, based on DESTINY-Breast09. The PATHWAY (4B5) companion diagnostic was co-approved.
T-DXd plus pertuzumab reduced the risk of disease progression or death by 44% versus standard THP: median PFS 40.7 months versus 26.9 months (HR 0.56; 95% CI 0.44-0.71; p<0.0001), with benefit regardless of hormone-receptor status.
No. Overall survival data remain immature (about 16% maturity), with an early numerical trend favoring T-DXd plus pertuzumab (HR 0.84; 95% CI 0.59-1.19). Longer follow-up is needed.
Interstitial lung disease (ILD)/pneumonitis is the key monitored risk: adjudicated drug-related ILD occurred in 12.1% of patients, including two fatal (Grade 5) events (0.5%). ILD was the leading cause of permanent discontinuation; neutropenia and nausea were also common.



















