FDA APPROVED June 24, 2026 — first-line metastatic TNBC not candidates for PD-(L)1 inhibitors
The FDA approved sacituzumab govitecan (Trodelvy, Gilead) as monotherapy for first-line unresectable locally advanced or metastatic triple-negative breast cancer in patients who are not candidates for PD-(L)1 inhibitors — based on the Phase 3 ASCENT-03 trial.
Source: Oncology Nursing News — FDA approval (June 24, 2026)ASCENT-03 at a Glance (TL;DR)
- Design: sacituzumab govitecan (Trodelvy) monotherapy vs physician's-choice chemotherapy, first-line metastatic TNBC not eligible for PD-(L)1 inhibitors.
- PFS: 9.7 vs 6.9 months — HR 0.62 (~38% reduction in progression or death), PD-L1-negative (ASCENT-03).
- Regulatory: FDA approved June 24, 2026 (first-line mTNBC, not candidates for PD-(L)1 inhibitors); EU approved; NCCN category-1 preferred.
- Drug: sacituzumab govitecan (Trodelvy, Gilead) — a Trop-2 antibody-drug conjugate.
- Trial: Phase 3 ASCENT-03; sponsor Gilead Sciences; NCT05382299.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated June 24, 2026.
KOL Reaction to the FDA Approval


KOLs Discussing ASCENT-03







ASCENT-03 Key Slides & Visuals
Presentation figures and KOL infographics, grouped by congress and readout. The #ASCO26 PFS2 / subsequent-therapy deep-dive (Abstract 1001, Tolaney) is called out first, followed by the cross-trial PFS2 context (ASCENT-03 vs ASCENT-04 vs TROPION-Breast02) that anchored the ASCO 2026 discussion, then the TROP2 biomarker-subgroup analysis (Abstract 1014, Barrios); the ESMO 2025 primary PFS readout (LBA20, Cortes) follows. Click any image to expand.
PFS2 & Subsequent Therapies#ASCO26 · ABSTRACT 1001
The ASCO 2026 update (Tolaney, Abstract 1001): progression-free survival after the next line of treatment (PFS2) and subsequent therapies. PFS2 18.2 vs 14.0 mo (HR 0.70) held up despite 82% of the chemo arm crossing over to sacituzumab govitecan.










PFS2 Across Trials#ASCO26 · CROSS-TRIAL CONTEXT
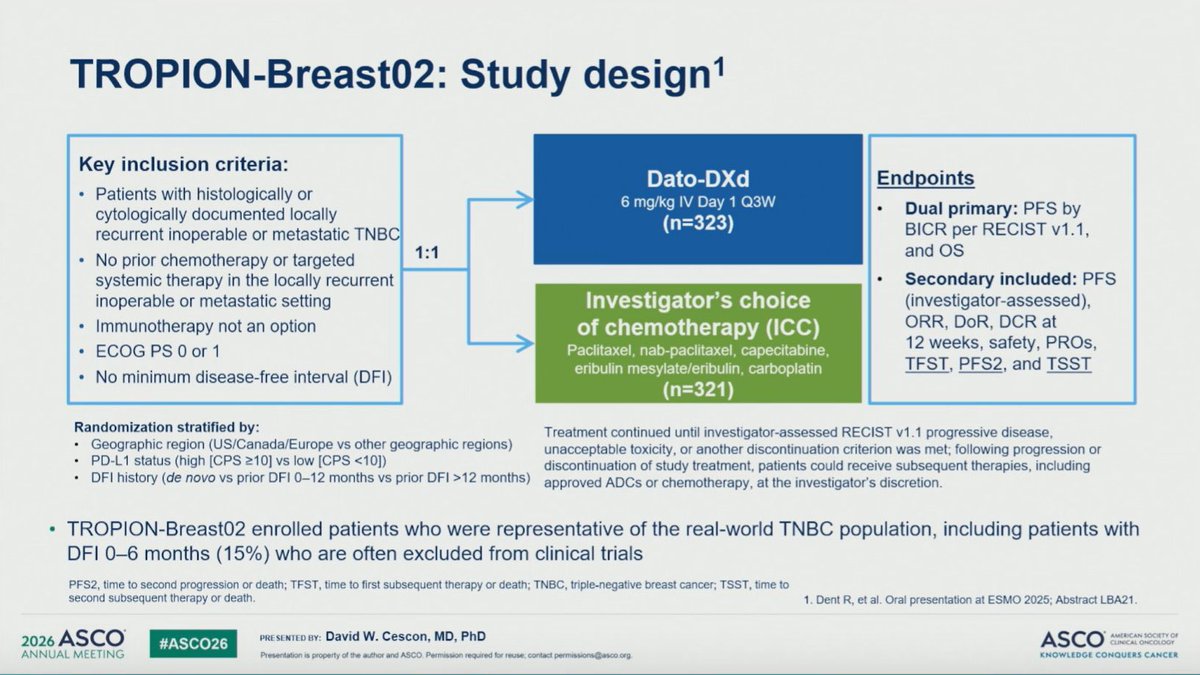
A defining ASCO 2026 conversation: PFS2 emerged as the key endpoint for first-line ADCs in mTNBC because overall survival is confounded by extensive crossover. The benefit held across all three pivotal 1L Trop-2 ADC trials — ASCENT-03 (SG mono, PD-(L)1-ineligible): PFS2 18.2 vs 14.0 mo, HR 0.70; ASCENT-04 (SG + pembro, PD-L1+): PFS2 NR vs 21.0 mo, HR 0.67; and TROPION-Breast02 (datopotamab deruxtecan vs chemo): PFS2 15.6 vs 11.8 mo, HR 0.61. KOLs noted the ASCENT trials allowed crossover (~79-82% of control patients later received SG) while TROPION-Breast02 did not, and that PFS2 lacks a standardized definition across trials — so the side-by-side designs (below) matter when interpreting the numbers. ASCENT-04 and TROPION-Breast02 are distinct trials shown for context; do not conflate their figures with ASCENT-03.


TROP2 Biomarker Subgroups#ASCO26 · ABSTRACT 1014
The ASCENT-03 biomarker analysis (Barrios, Abstract 1014): sacituzumab govitecan extended median PFS versus chemotherapy across all Trop-2 expression subgroups (Trop-2 quartile HRs 0.54–0.84 among ~499 Trop-2-evaluable patients), and the benefit was consistent regardless of tumor BRCA (tBRCA) mutation status and HER2 IHC0/IHC-low status — supporting SG for the broad 1L PD-(L)1-ineligible mTNBC population without the need for biomarker selection. Slides showing PFS by Trop-2 quartile from the companion PD-L1+ ASCENT-04 analysis (Abstract 1013) are deliberately excluded here to avoid conflation.



Primary PFS ReadoutESMO 2025 · LBA20
The ESMO 2025 primary analysis (Cortes, LBA20; simultaneous NEJM publication): the registrational PFS, OS, response, and safety data that established the first-line benefit.











Top ASCENT-03 Tweets
Day 3 & 4 #ASCO26 highlights: 1. #evERA: Giredestrant in mHR+ BC 2. #ASCENT03/04: Saci 1L mTNBC 3. #CIRCULATE: ctDNA in CRC 4. #EPISODE3: Adj Aspirin in CRC 5. #EMERALD3: STRIDE + TACE + Len in HCC 6. #DeLLphi304: Tarla in SCLC @ASCO #OncTwitter @OncoAlert 1/7
#ASCO26 ASCENT-03 PFS2 analysis PFS2 difference was 4.2 mo✅️ This is notable because 82% of patients in the chemo arm received SG as subsequent therapy. Despite this crossover, earlier SG still maintained a PFS2 advantage. This strengthens the argument for using SG in 1L

#ASCO26 🎗️ Sacituzumab govitecan (SG) keeps extending its lead in 1L metastatic TNBC. 📈 ASCENT-03 showed improved PFS2 despite heavy crossover to SG after progression. 🔄 📌 mTNBC not eligible for PD-(L)1 inhibitors 📌 1L SG vs physician’s choice chemo 💉 📌 Median PFS2: 18.2
#ASCO26 🚨 ASCENT-03 reinforces the durability of first-line sacituzumab govitecan in PD-L1–negative mTNBC. Even after crossover and subsequent therapies, the PFS2 benefit persisted. 🔹 PFS2: 18.2 vs 14.0 mo 🔹 HR 0.70 (P=.0051) 🔹 18-mo PFS2: 52% vs 41% This matters because

PFS2 in Metastatic Breast Cancer: What Does It Really Mean? Great review!! (1) PFS2 lacks a standardized definition and varies across trials, making cross-study comparisons difficult. (2) In studies such as ASCENT-03/04 and TROPION-Breast02, PFS2 was defined differently and may

ASCENT-03(PD-L1陰性またはICI不適応TNBC) PFS 9.7 vs 6.9か月 HR 0.62が既報でした。 PFS2中央値は SG群18.2か月 抗がん剤群14.0か月HR0.70 P値0.0051
#ASCO26 Biomarker analysis from ASCENT-03 showed that SG improved PFS versus chemotherapy across all evaluated subgroups in previously untreated advanced TNBC patients who were not candidates for PD-(L)1 inhibitors. Benefit was consistent regardless of Trop-2 expression level,
#ASCO26 🚨 ASCENT-03 reinforces the case for frontline sacituzumab govitecan in PD-L1–ineligible mTNBC. Despite heavy crossover (82% of chemo arm later received SG), SG still improved PFS2: 🔹 PFS2: 18.2 vs 14.0 mo 🔹 HR 0.70 🔹 30% lower risk of progression after next-line

#ASCO26 Practice-Changing: The ASCENT-03 Trial, presented by @stolaney1 establishes Sacituzumab Govitecan as the new first line standard of care for PD-(L)1-ineligible metastatic TNBC, delivering superior and durable disease control beyond chemotherapy. @OncoAlert #bcsm

ASCENT 03 binaries analysis 🚨 SG ➡️ improved PFS > chemo as 1L in TNBC 📌Benefit observed in variable TROP2 expression, BRCA mutation and HER2 expression subgroups!! 🔪The bystander effect with SG—benefit in low TROP2 expression! @OncoAlert #ASCO2026 #MBC #TNBC

ASCENT-03: Efficacy by biomarker subgroup with sacituzumab govitecan vs chemotherapy in participants with previously untreated advanced triple-negative #breastcancer who are not candidates for PD-(L)1 inhibitors Carlos H. Barrios #ASCO26 @OncoAlert #OncoAlert
#ASCO26 Abstract 1001 - ASCENT-03: PFS2 and subsequent therapies with sacituzumab govitecan vs chemotherapy in previously untreated mTNBC.
Overview
ASCENT-03 (NCT05382299) is a Phase 3, international, open-label, randomized trial of the Trop-2 antibody-drug conjugate sacituzumab govitecan (SG; Trodelvy) versus physician's-choice chemotherapy (paclitaxel, nab-paclitaxel, or gemcitabine + carboplatin) in patients with previously untreated locally advanced unresectable or metastatic triple-negative breast cancer who are not candidates for PD-(L)1 inhibitors — i.e., PD-L1-negative (CPS < 10), or PD-L1-positive but ineligible due to prior immunotherapy or comorbidity. This PD-(L)1-ineligible group represents roughly 60% of first-line mTNBC. 558 patients were randomized 1:1 (279 SG vs 279 chemo); crossover to SG was permitted at progression. The primary endpoint is progression-free survival by blinded independent central review (BICR). Primary PFS was presented at ESMO 2025 (LBA20, Javier Cortes) with simultaneous publication in the New England Journal of Medicine; a dedicated PFS2 / subsequent-therapy analysis (Abstract 1001) and a TROP2 biomarker-subgroup analysis (Abstract 1014) were presented at #ASCO26 by Sara Tolaney.
Study Design
Phase 3, international, open-label, randomized 1:1 (279 SG vs 279 chemo). SG 10 mg/kg IV days 1 & 8 of 21-day cycles vs physician's-choice chemo. Crossover to 2L SG allowed after BICR-verified progression. Median follow-up 13.2 mo. Sponsor: Gilead Sciences.
Population
N=558 with previously untreated locally advanced or metastatic TNBC, not candidates for PD-(L)1 inhibitors (PD-L1-negative CPS < 10 by 22C3, or CPS ≥ 10 but ineligible). ~99% PD-L1-negative; stable treated CNS metastases allowed.
Intervention
Experimental: sacituzumab govitecan (Trop-2 ADC). Control: physician's-choice chemo — paclitaxel, nab-paclitaxel, or gemcitabine + carboplatin. Chemo type selected before randomization.
Endpoints
Primary: PFS by BICR. Secondary: OS, ORR, DOR, TTR, safety, QOL, and PFS2 (progression on next-line therapy). OS remains immature.
Results — ESMO 2025 Primary & #ASCO26 Update
Progression-Free Survival (Primary Endpoint — MET)
First-line SG produced a statistically significant and clinically meaningful improvement in PFS by BICR: median 9.7 months vs 6.9 months with chemo, HR 0.62 (95% CI 0.50-0.77), P < 0.0001 — a 38% reduction in the risk of progression or death (investigator-assessed HR 0.64; 9.6 vs 6.8 mo). The 12-month PFS rate was 41% vs 24%. Objective response rates were similar (ORR 48% vs 46%), but responses were far more durable with SG: median DOR 12.2 vs 7.2 months.
Median PFS 9.7 vs 6.9 mo · HR 0.62 (0.50-0.77), P<0.0001 · ORR 48% vs 46% · DOR 12.2 vs 7.2 moSources: ESMO 2025 LBA20 (Cortes) · NEJM 2025 (DOI 10.1056/NEJMoa2511734) · ClinicalTrials.gov NCT05382299Overall Survival (Secondary — Immature) & Safety
At the primary analysis, overall survival was immature (37% maturity): median 21.5 vs 20.2 months, HR 0.98 (95% CI 0.75-1.30) — no separation yet, with interpretation complicated by extensive crossover (the study continues to a formal OS analysis). On safety, grade ≥ 3 TEAEs were similar (66% vs 62%), as was grade 3 neutropenia (43% vs 41%); SG carried more grade 3 diarrhea (9% vs 1%). Notably, treatment discontinuation was lower with SG (4% vs 12%). There were 7 deaths in the SG arm; 6 were treatment-related infections and 5 were secondary to neutropenia in high–febrile-neutropenia-risk patients who did not receive G-CSF prophylaxis — underscoring the importance of growth-factor support.
OS HR 0.98 (0.75-1.30) — immature · G≥3 TEAE 66% vs 62% · neutropenia G3 43% vs 41% · discontinuation 4% vs 12% · G-CSF prophylaxis criticalSources: ESMO 2025 LBA20 (Cortes, safety/OS slides) · NEJM 2025PFS2 & Subsequent Therapy (ASCO 2026 — Tolaney)
Because OS remains immature, ASCO 2026 reported PFS2 (time to progression on the next line of therapy) to capture durable benefit across treatment sequences. Median PFS2 was 18.2 months with SG vs 14.0 months with chemo — a 4.2-month difference — stratified HR 0.70 (95% CI 0.55-0.90), P = 0.0051; the 18-month PFS2 rate was 52% vs 41%. Critically, this benefit persisted despite extensive crossover: among chemo-arm patients who started a subsequent therapy, ~82% received SG. Time to first subsequent therapy was also longer with SG (11.2 vs 7.9 months). A companion TROP2 biomarker analysis (Abstract 1014) showed SG's PFS benefit was maintained across all TROP2 expression subgroups (Trop-2 quartile HRs 0.54-0.84; benefit also independent of tBRCA and HER2-IHC status).
PFS2 18.2 vs 14.0 mo · HR 0.70 (0.55-0.90), P=0.0051 · benefit persists despite ~82% chemo-arm crossover to SG · consistent across TROP2 subgroupsSources: ASCO 2026 Abstract 1001 (Tolaney, PFS2) & Abstract 1014 (TROP2 biomarker) · JCO DOI 10.1200/JCO.2026.44.16_suppl.1001Clinical Implications
ASCENT-03 establishes first-line sacituzumab govitecan as an effective new option for PD-(L)1-ineligible mTNBC — a setting where physician's-choice chemotherapy has been the default and where about 60% of 1L patients fall. The near-doubling of durable responses (DOR 12.2 vs 7.2 mo) and the sustained PFS2 benefit despite heavy crossover argue that giving SG up front is better than reserving it for later lines. Open questions KOLs are watching: overall survival remains immature (and crossover may blunt any separation), the 1L indication is now FDA approved (June 24, 2026), and how SG compares with the other 1L Trop-2 ADC datopotamab deruxtecan (TROPION-Breast02), which reported an OS benefit in an overlapping population. G-CSF prophylaxis and infection management are central to safe delivery.
New 1L option for ~60% of mTNBC (PD-(L)1-ineligible) · durable responses & sustained PFS2 · OS immature · 1L FDA approved (Jun 24, 2026)Sources: ESMO 2025 LBA20 / NEJM · ASCO 2026 Abstract 1001 & 1014 · ClinicalTrials.gov NCT05382299Key KOL Sentiments — ASCENT-03
See how oncologists are reacting across the Trodelvy program: Physician Sentiment on TRODELVY® →











ASCENT-03: Frequently Asked Questions
What is the ASCENT-03 trial?
ASCENT-03 is a Phase 3 randomized trial comparing sacituzumab govitecan (Trodelvy) monotherapy with physician's-choice chemotherapy in first-line metastatic triple-negative breast cancer in patients who are not candidates for PD-(L)1 inhibitors.
What were the ASCENT-03 results?
Sacituzumab govitecan improved median progression-free survival to 9.7 versus 6.9 months, an approximately 38% reduction in the risk of progression or death versus chemotherapy.
Is sacituzumab govitecan FDA approved for first-line TNBC?
Yes. In June 24, 2026 the FDA approved sacituzumab govitecan (Trodelvy) as monotherapy for first-line metastatic triple-negative breast cancer in patients not candidates for PD-(L)1 inhibitors, based on ASCENT-03.
What is the drug and how does it work?
Trodelvy (sacituzumab govitecan) is a Trop-2-directed antibody-drug conjugate developed by Gilead Sciences.
Who sponsored ASCENT-03 and what is its identifier?
ASCENT-03 was sponsored by Gilead Sciences; its ClinicalTrials.gov identifier is NCT05382299.