Perioperative enfortumab vedotin + pembrolizumab (Padcev + Keytruda) is now FDA-approved (July 10, 2026) for adult muscle-invasive bladder cancer patients who are radical-cystectomy candidates, regardless of cisplatin eligibility — based on EV-304/KEYNOTE-B15 (EFS HR 0.53; pCR 55.8% vs. 32.5%), the first platinum-free regimen to beat chemo in ~25 years.
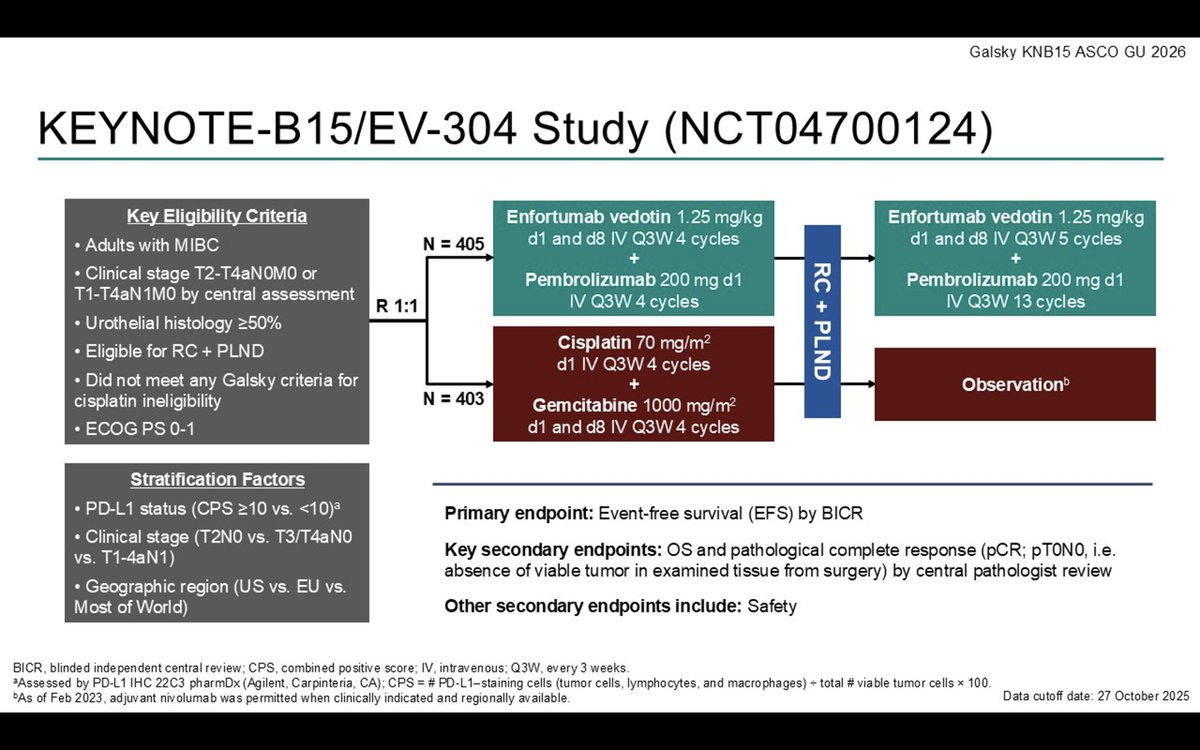
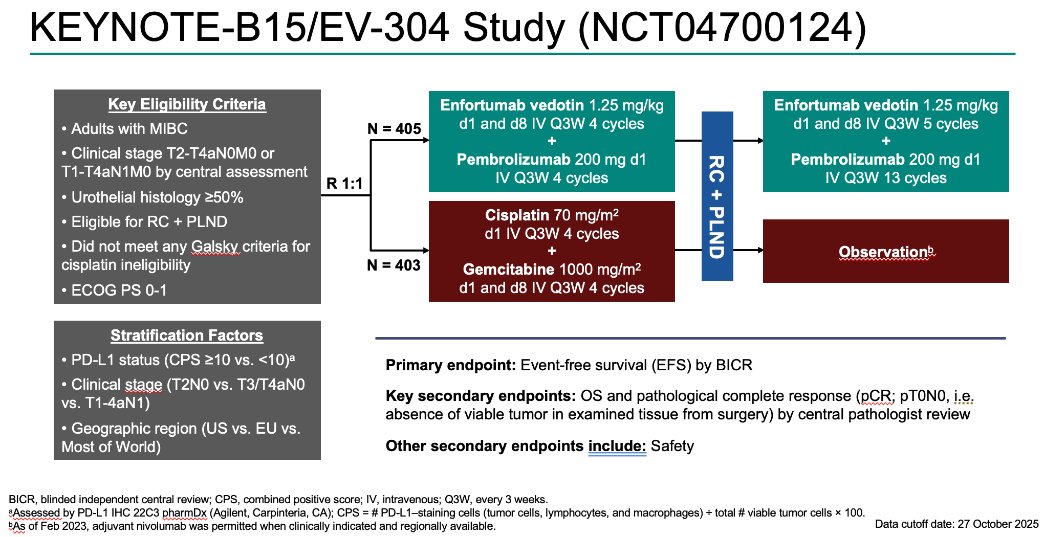
Discover KOL Sentiment on KEYNOTE-B15 →View EV-304 on ClinicalTrials.gov →Design - Phase 3 perioperative enfortumab vedotin + pembrolizumab vs gemcitabine/cisplatin, MIBC radical-cystectomy candidates (NCT04700124 / EV-304).
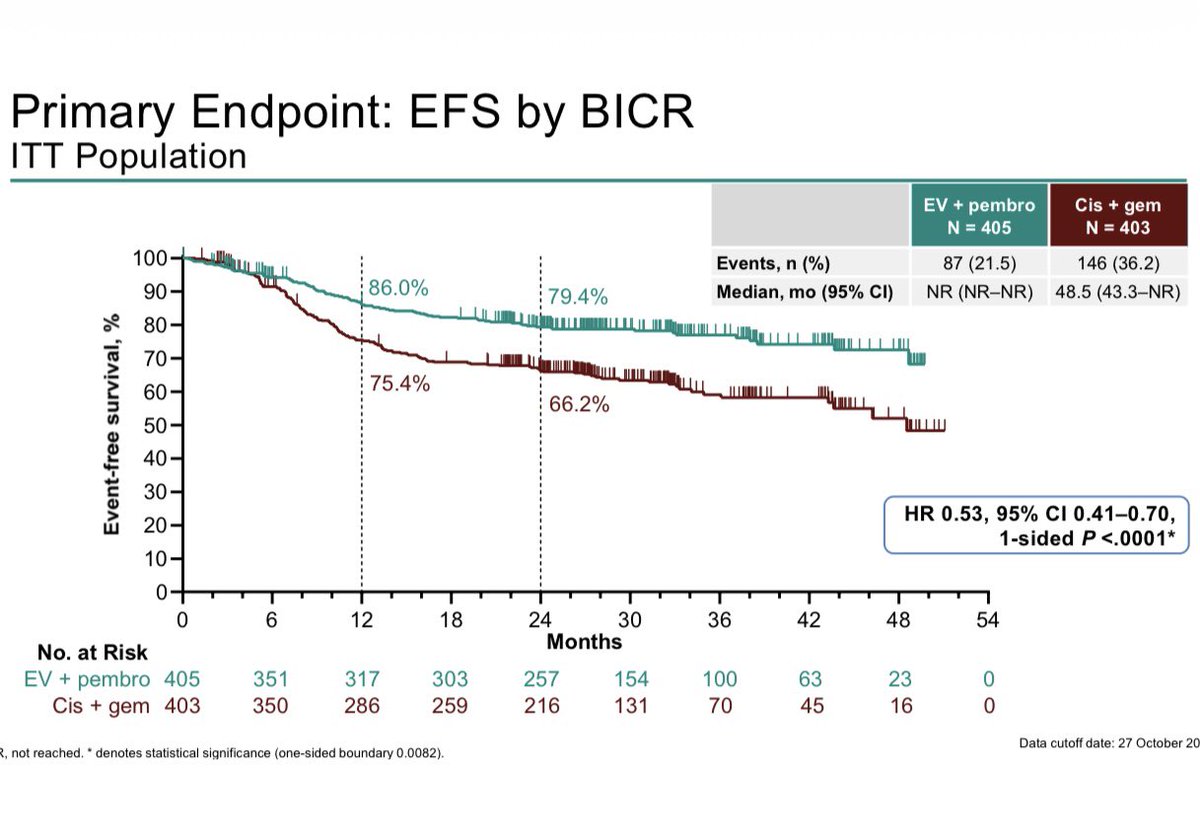
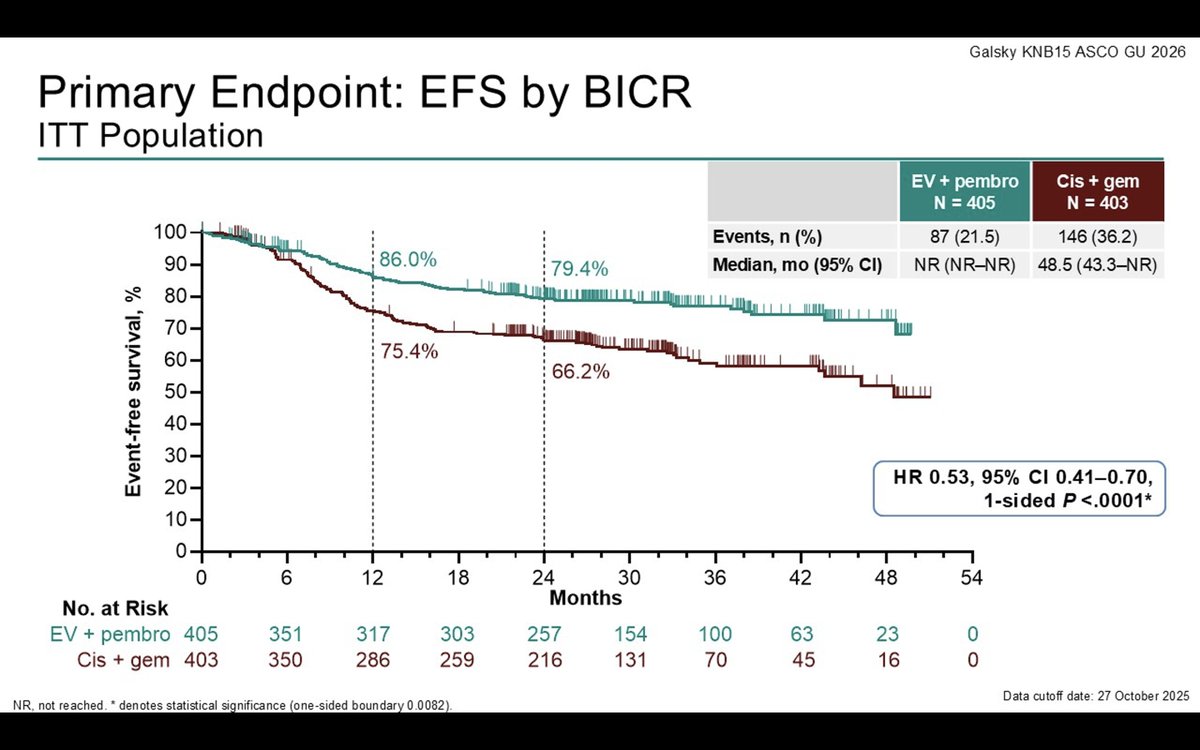
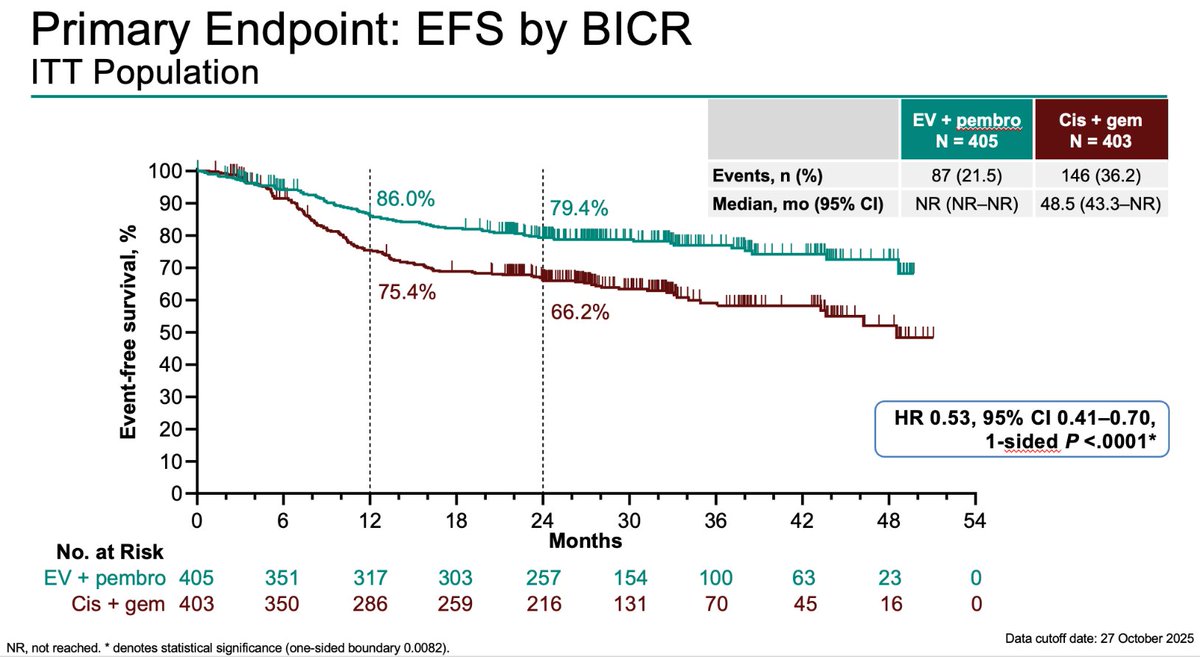
EFS (co-primary) - HR 0.53 (95% CI 0.41-0.70); 24-month EFS 79.4% vs 66.2%.
pCR (co-primary) - 55.8% with EV + pembrolizumab vs 32.5% with chemotherapy.
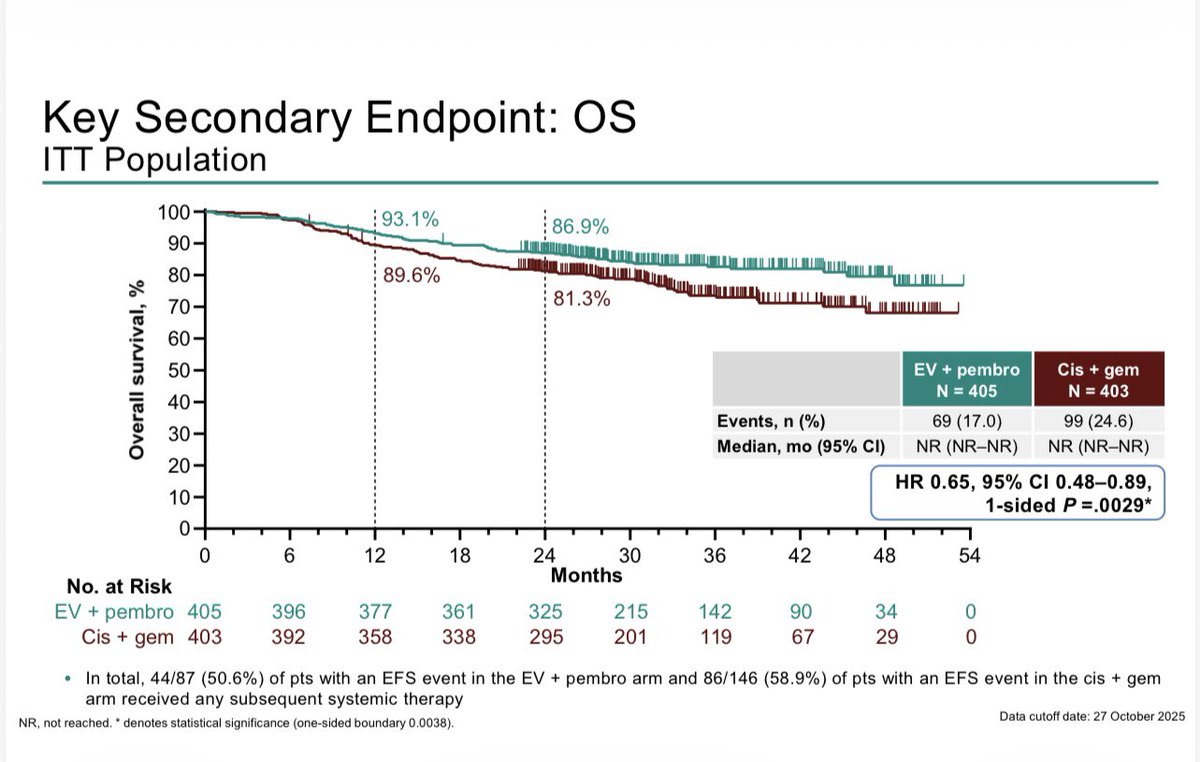
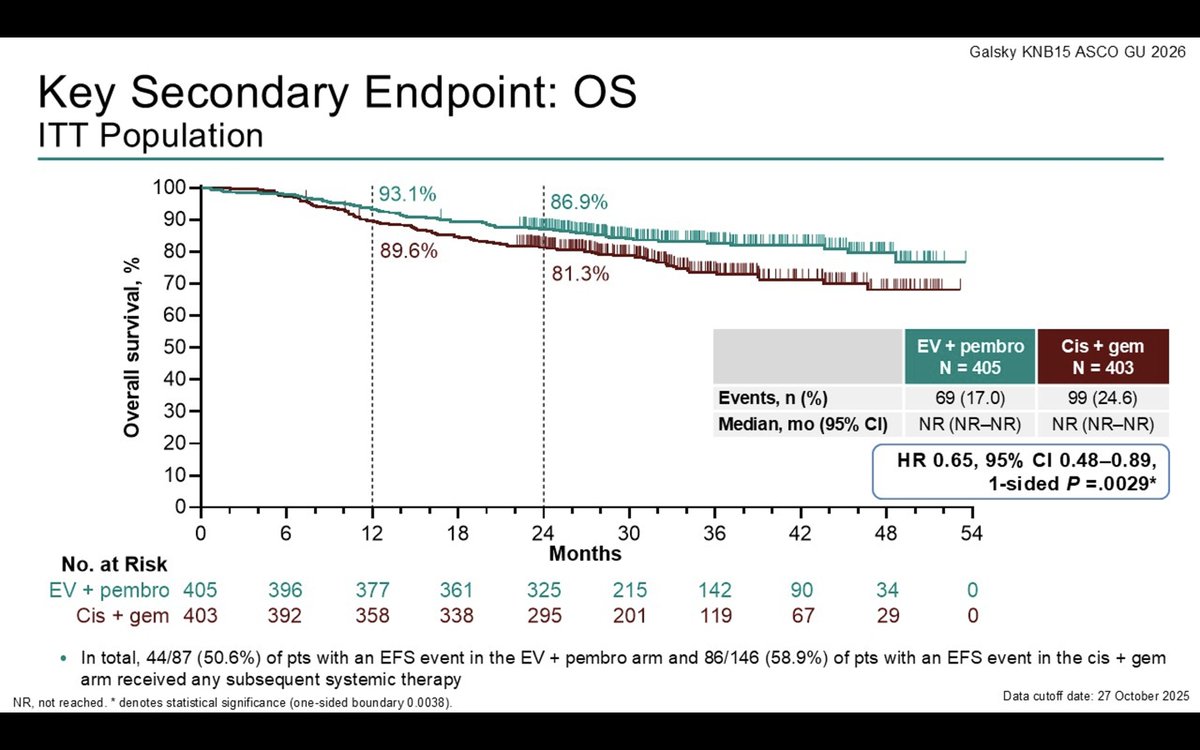
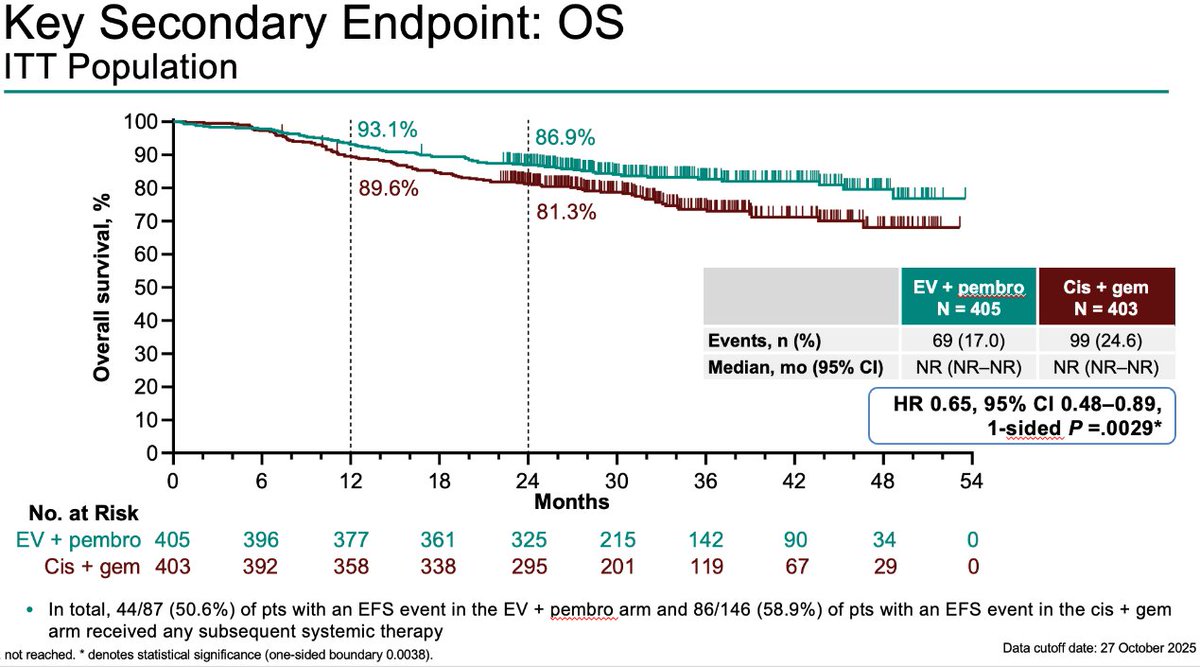
OS - HR 0.65 (95% CI 0.48-0.89) - about a 35% reduction in risk of death; both medians not reached.
Safety - Grade >=3 AEs 75.7% vs 67.2%; profile consistent with the individual agents, no new safety signals.
Regulatory - FDA approved July 10, 2026 - first platinum-free perioperative regimen to beat cisplatin chemotherapy in MIBC in ~25 years.
Sponsor / drug - Astellas + Pfizer (Seagen) + Merck; Padcev + Keytruda.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.






Create a free account, pick the tumor types you cover, and go beyond the tweet — the intelligence pharma teams use to map influence and prepare for engagement:





Top tweets by impressions — click to view on X

Now, the combo of EV-Pembro is @US_FDA approved for all muscle-invasive bladder cancer @OncoAlert @AUC3_Official @Merck @BladderCancerUS @OncoBellmunt @bergsa83 @mouwlab

Perioperative EV plus pembrolizumab is now approved for every MIBC patient headed for cystectomy, cisplatin-eligible or not. The FDA expanded the label today on the strength of a head-to-head win over cisplatin-based chemo, the standard we've used for 20 years.

🚨 Updates for MIBC 🚨 FDA approves neoadjuvant + adjuvant EV+pembro for muscle-invasive bladder cancer — regardless of cisplatin eligibility. The first platinum-free regimen to beat SOC chemo in ~25 yrs. EV-304 (KEYNOTE-B15): 📉 EFS HR 0.53 (47% ↓ recurrence/progression/death)
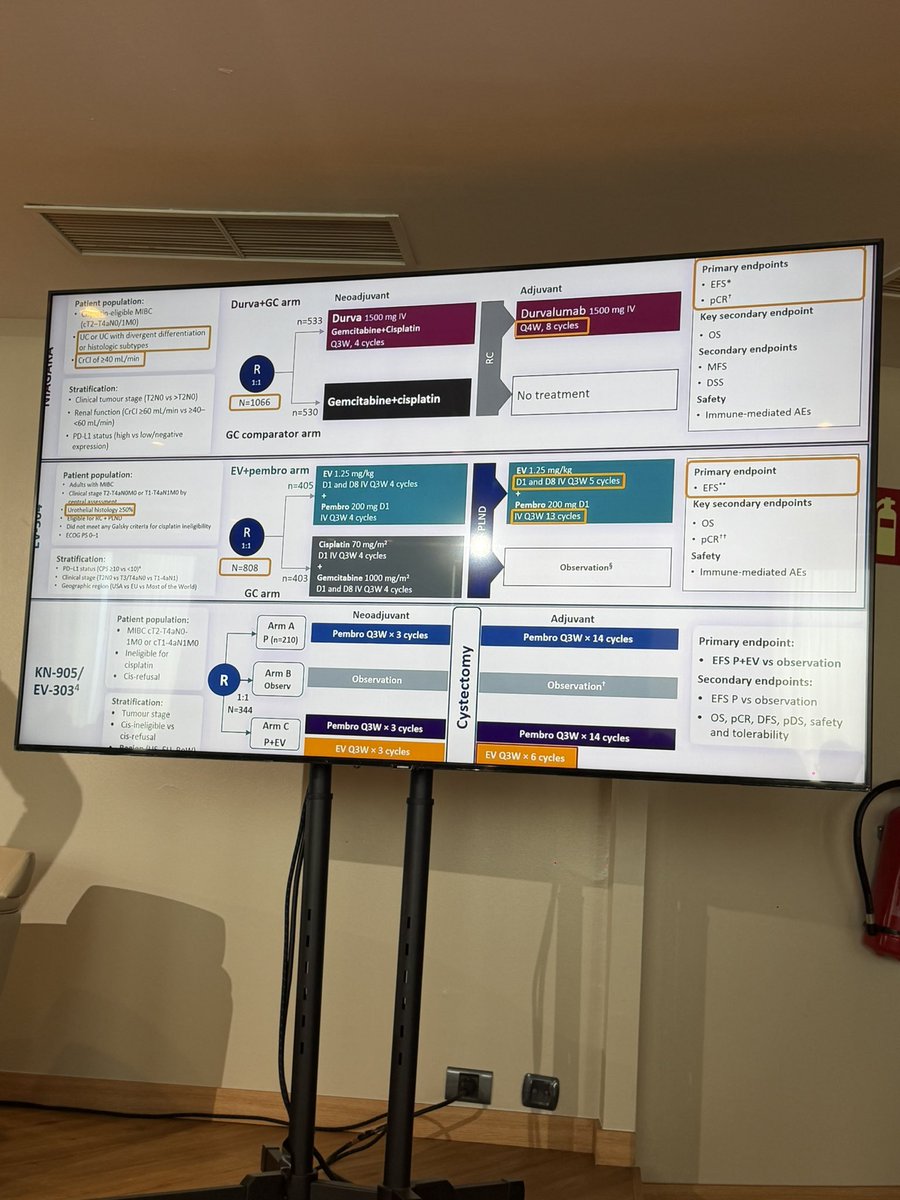
3 studies testing Perioperative immune bases therapy (EVP or Gem/Cis/Durva) in muscle invasive bladder all have shown an OS advantage vs standard of care. KN905 (EVP) is distinct in that it’s in a…
KN-B15/EV303: R3 Perioperative EVP vs Gem/cis in MIBC shows EFS HR 0.53 (0.41–0.70), OS HR 0.65 (0.48-0.89), pCR 56% vs 33%, G3+ tox 76% vs 67% #GU26. About half the patients completed 9 cycles of…
Is this the end of cisplatin in MIBC?
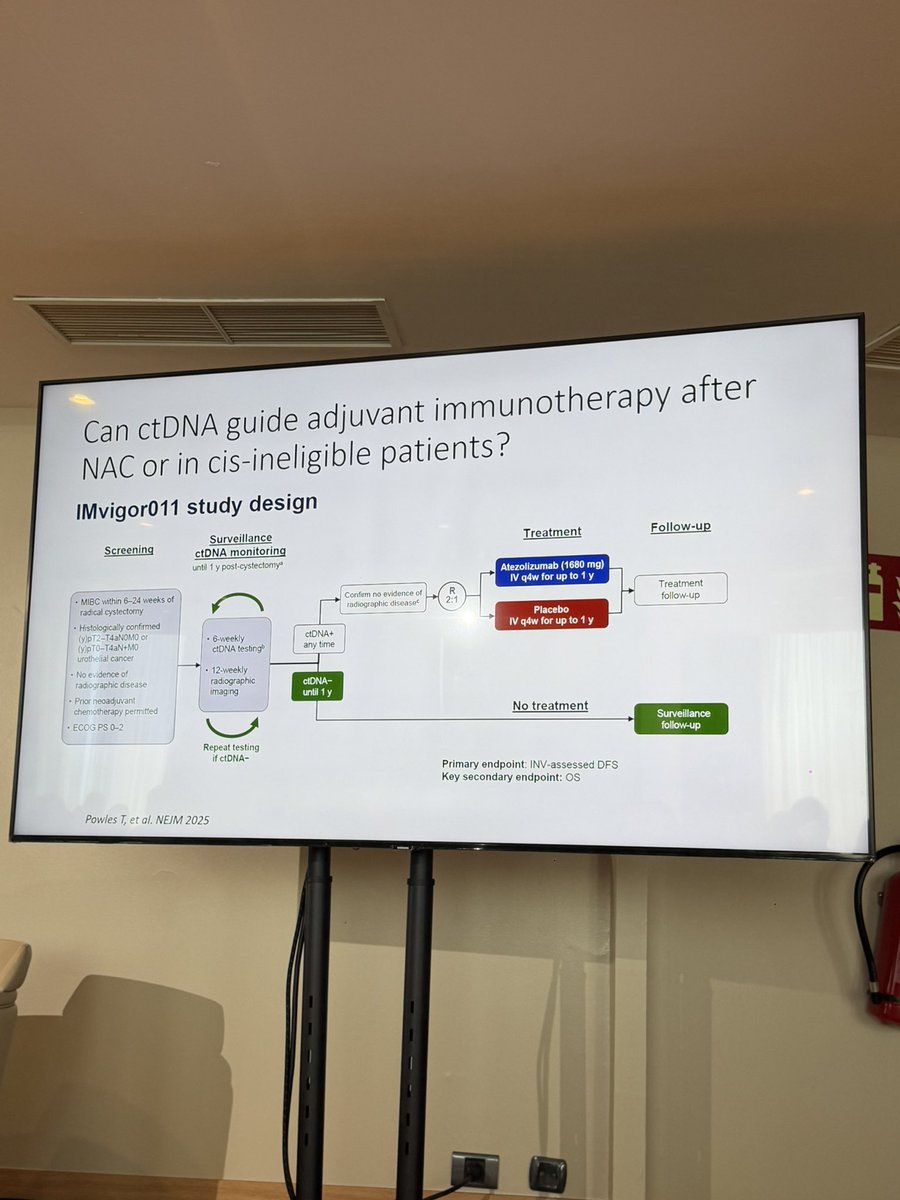
With the results from NIAGARA, KEYNOTE-B15/EV-304, and KEYNOTE-905/EV-303, along with the emergence of ctDNA in IMvigor011, it is becoming increasingly…
KEYNOTE-B15/EV-304 trial is practice-changing: periop EV+ pem:
🔥 47% reduction in risk of events (HR 0.53)
🔥 Significant OS benefit (HR 0.65)
🔥 pCR 55.8% vs 32.5%
A true paradigm shift for…
A "slam-dunk home run" from $PFE $ALPMF Padcev. @ByMadeleineA on #GU26 late-breaking Keynote-B15 data, via @ApexOnco -> https://t.co/O6ynVa4H7H $MRK

🚨 KEYNOTE-B15: Perioperative EV + pembrolizumab significantly improved EFS, OS, & pCR vs cisplatin chemo in cisplatin-eligible MIBC, marking the first regimen in ~25 years to surpass the…

Day 2 (#bladder!) for @ASCO #GU26!!
Really nice discussion by @DrTylerStewart of the KEYNOTE-B15 study
⭐️practice-changing, let's put discussion of ddMVAC to rest https://t.co/0f7ZAfPFOL
UC Takeaways from #ASCOGU26
1) KEYNOTE-B15 is a landmark. Periop EV+pembro vs gem/cis in cis-eligible MIBC: EFS HR 0.53, pCR 55.8% vs 32.5%, OS benefit. First regimen to displace cisplatin in…

🔥 Presented at #EAU2026: new KEYNOTE-B15 / EV-304 data
✅After previously reported survival benefits, new data now also highlight improved pathological downstaging and disease-free survival with…
Cross trial comparison and where we are heading in MIBC @asco #gu26 @DrChoueiri @dr_yakupergun @brunolarvol @OncoAlert @OncBrothers https://t.co/5gzECBkrrf
Practice-changing and now FDA-approved (July 10, 2026). EV+P in cisplatin-eligible MIBC extends the perioperative IO paradigm beyond NIAGARA (durvalumab+GC). Direct competition between ADC+IO (KEYNOTE-B15) and chemo+IO (NIAGARA) for the cisplatin-eligible population. On July 10, 2026 the FDA expanded the perioperative EV+pembro label to cisplatin-eligible patients, making the regimen available for adult MIBC radical-cystectomy candidates regardless of cisplatin eligibility — building on the November 21, 2025 approval in the cisplatin-ineligible population.
Event-free survival HR was 0.53 (95% CI 0.41-0.70, P<0.0001) favoring enfortumab vedotin + pembrolizumab. 24-month EFS rate: 79.4% vs. 66.2%. Median EFS not reached with EV+P vs. 48.5 months with gem/cis. pCR (pathological complete response) rate: 55.8% vs. 32.5%.
OS improvement reported — approximately 35% risk reduction favoring EV+P vs. chemotherapy (OS HR 0.65, 95% CI 0.48-0.89, 1-sided P=0.0029). Both median OS values not reached. FDA approved the perioperative EV+pembro regimen for cisplatin-eligible MIBC on July 10, 2026.
Grade ≥3 adverse events occurred in 75.7% with EV+P vs. 67.2% with gem/cis. Key AEs: EV-related skin reactions (14.1% G≥3), peripheral neuropathy; pembrolizumab-related skin reactions (13.9% G≥3). Profile manageable and consistent with individual agents. Across EV-303 and EV-304, the most common (≥30%) treatment-related adverse events were pruritus, alopecia, diarrhea, and anemia; no new safety signals were observed. Prescribing warnings include immune-mediated reactions, serious skin reactions, hyperglycemia, pneumonitis/interstitial lung disease, peripheral neuropathy, ocular disorders, infusion-site extravasation, and embryo-fetal toxicity.
✅ FDA approved (July 10, 2026) — a paradigm shift in cisplatin-eligible MIBC. Perioperative EV+pembro is now FDA-approved for adult MIBC patients who are radical-cystectomy candidates, regardless of cisplatin eligibility — the first platinum-free perioperative regimen to displace cisplatin-based chemotherapy in ~25 years. EV+P extends the perioperative IO paradigm beyond NIAGARA (durvalumab+GC), with direct competition between ADC+IO (KEYNOTE-B15) and chemo+IO (NIAGARA) for the cisplatin-eligible population. This label expansion builds on the November 21, 2025 approval for cisplatin-ineligible MIBC (EV-303/KEYNOTE-905).
KEYNOTE-B15 / EV-304 (NCT04700124) is a Phase 3 randomized trial of perioperative enfortumab vedotin (Padcev) plus pembrolizumab (Keytruda) versus neoadjuvant gemcitabine-cisplatin chemotherapy in patients with muscle-invasive bladder cancer who are candidates for radical cystectomy. Event-free survival and pathologic complete response were co-primary endpoints.
Event-free survival strongly favored the enfortumab vedotin plus pembrolizumab regimen (HR 0.53; 95% CI 0.41-0.70; 24-month EFS 79.4% vs 66.2%), the pathologic complete response rate was 55.8% versus 32.5% with chemotherapy, and overall survival improved with a hazard ratio of 0.65 (95% CI 0.48-0.89), about a 35% reduction in the risk of death.
Yes. On July 10, 2026 the FDA approved perioperative enfortumab vedotin (Padcev) plus pembrolizumab (Keytruda) for adults with muscle-invasive bladder cancer who are candidates for radical cystectomy, regardless of cisplatin eligibility - the first platinum-free perioperative regimen to displace cisplatin-based chemotherapy in this setting in about 25 years.
Grade >=3 adverse events occurred in 75.7% of patients on enfortumab vedotin plus pembrolizumab versus 67.2% with gemcitabine-cisplatin. Key toxicities included enfortumab-vedotin-related skin reactions and peripheral neuropathy and pembrolizumab-related skin reactions; the profile was consistent with the individual agents, with no new safety signals reported.
KEYNOTE-B15 / EV-304 extends the perioperative immunotherapy paradigm in MIBC beyond NIAGARA (durvalumab plus gemcitabine-cisplatin). It is notable for being a platinum-free antibody-drug-conjugate-plus-immunotherapy regimen that outperformed cisplatin-based chemotherapy, broadening options for radical-cystectomy candidates regardless of cisplatin eligibility.