DeLLphi-304 Key Takeaways
Design - Phase 3 tarlatamab (DLL3 bispecific T-cell engager) vs chemotherapy, second-line SCLC after platinum-based therapy (NCT05740566).
OS (primary, met) - Median 13.6 vs 8.3 mo, HR 0.60 (95% CI 0.47-0.77; p<0.001).
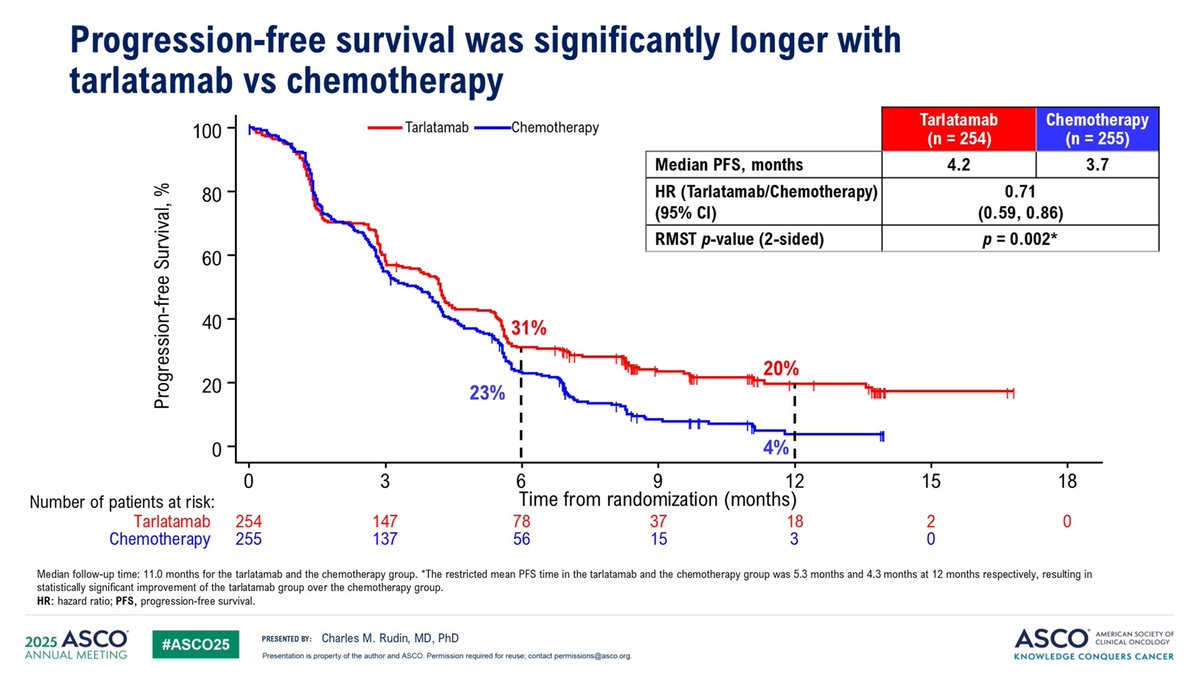
PFS / response - PFS 4.2 vs 3.2 mo (HR 0.72); objective response rate 27% vs 9%.
CNS (ASCO 2026 post hoc, Abstract 8006) - First CNS-efficacy data for a T-cell engager in SCLC: ITT CNS PFS HR 0.54; among baseline brain-mets patients CNS PFS HR 0.40.
Safety - Grade >=3 AEs 54% vs 80% (chemo); cytokine release syndrome 56% (Grade >=3 only 1.2%), concentrated around step-up dosing.
Regulatory / drug - FDA approved (relapsed SCLC); Amgen; tarlatamab (Imdelltra).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.
KOLs Discussing DeLLphi-304



DeLLphi-304 Key Slides & Visuals
CNS post hoc slides shared by KOLs at the #ASCO26 oral abstract session (Abstract 8006, presented by Giannis Mountzios, MD), plus the ASCO 2025 primary overall-survival readout. Click any image to expand.




















































Top DeLLphi-304 Tweets

Day 3 & 4 #ASCO26 highlights: 1. #evERA: Giredestrant in mHR+ BC 2. #ASCENT03/04: Saci 1L mTNBC 3. #CIRCULATE: ctDNA in CRC 4. #EPISODE3: Adj Aspirin in CRC 5. #EMERALD3: STRIDE + TACE + Len in HCC 6. #DeLLphi304: Tarla in SCLC @ASCO #OncTwitter @OncoAlert 1/7

🚨 #ASCO26 | DeLLphi-304 post hoc analysis #️⃣Abstr 8006 🧠 Tarlatamab vs chemotherapy in 2L SCLC with brain metastases ✅ All patients Tarlatamab delayed CNS progression/death CNS PFS: NE vs 7.2 mo, HR 0.54 🧠 Patients with brain metastases ・Median CNS PFS: 6.5 vs 4.2 mo,

Dr. @g_mountzios #ASCO26 presents CNS outcomes with 2L tarlatamab in DeLLphi-304. Improved time to CNS progression overall (HR 0.54). In pts with brain nets, tarlatamab vs chemo CNS CR rate 15% vs 5% with DCR 78% vs 71% and time to CBS progression 6.5m vs 4.2m, HR 0.40

What a happy coincidence! While presenting intracranial efficacy data from DeLLphi-304 in #ASCO26, #Tarlatamab was officially approved in EU!! ✅ In ITT: CNS mPFS NR vs 7.8 m, HR=0.54 ✅ In BM per mRANO: CNS mPFS 6.5 vs 4.2m, HR=0.4 ✅ mOS=13.9 vs 6.8, HR=0.51, independent

ASCO26 DeLLphi-304 CNS post hoc: #tarlatamab delayed CNS progression/death vs chemo in 2L ES-SCLC. CNS PFS HR 0.54 overall; HR 0.40 with brain mets. Also improved OS in pts with brain mets: 13.9 vs 6.8 mo; HR 0.51. Strong CNS signal here.

#ASCO26 One of the most clinically relevant SCLC updates of the meeting. In DeLLphi-304, tarlatamab not only improved OS versus chemotherapy, but also showed meaningful intracranial activity: • CNS progression/death HR 0.54 overall • HR 0.40 in patients with brain metastases

🔥🚨@OncoAlert Hot off the press. Just presented @ASCO #ASCO26 by Dr. @g_mountzios ⭐️#PostHoc Analysis Results of #Intracranial 🧠 #Efficacy of: ❇️#Tarlatamab 🆚 #Chemotherapy in #2nd line treatment for #SmallCell #LungCancer in the #DeLLphi304 Trial. ‼️‼️#Exciting &

DeLLphi-304: Tarlatamab vs Chemo for Brain Mets in Relapsed SCLC ▫️Median CNS PFS 6.5 vs 4.2 mos ▫️Intracranial CR: 14.9% vs 5.4% @g_mountzios #ASCO26

Tarlatamab n=254 vs chemo n=255. 🧠Takeaway: meaningful CNS benefit. CNS PFS, all patients (RECIST, ITT): 🧠median NE (95% CI 13.7–NE) with tarlatamab vs 7.2 mo with chemo. 🧠HR 0.54 (0.39–0.75) 🧠a 46% lower risk of CNS progression or death. #ASCO26 @SclcSMASHERS @ASCO
In patients WITH baseline brain mets (mRANO-BM/BICR, tarlatamab n=67 vs chemo n=56): median CNS PFS 6.5 vs 4.2 mo, HR 0.40 (0.24–0.66) 6-mo CNS PFS 53.9% vs 27.0% Small subsets but a 60% risk reduction @ASCO #ASCO26 #LCSM @SclcSMASHERS

DeLLphi-304: 🫁 Tarlatamab Redefines CNS Control in Relapsed SCLC, Cutting Intracranial Progression Risk by 60% @ASCO @OncoAlert #Lcsm #ASCO26
OS in patients with brain mets: 13.9 vs 6.8 mo, HR 0.51 (0.34–0.74) 🧠tarlatamab cut risk of death by 49% vs chemo. 🧠Intracranial CR rate and duration of intracranial disease control also favored tarlatamab. #ASCO26 @ASCO #LCSM @SclcSMASHERS #medED
Overview
DeLLphi-304 (NCT05740566) is a Phase 3, global, randomized, open-label trial of tarlatamab (Imdelltra) versus investigator's choice of standard chemotherapy (topotecan, lurbinectedin, or amrubicin) in patients with small-cell lung cancer that has relapsed after one prior platinum-based regimen. Tarlatamab is a first-in-class DLL3 × CD3 bispecific T-cell engager (BiTE). The pivotal results — a statistically significant overall-survival benefit — were presented at ASCO 2025 and simultaneously published in the New England Journal of Medicine. At #ASCO26, Dr. Giannis Mountzios presented a prespecified CNS post hoc analysis (Abstract 8006) characterizing intracranial efficacy, including in the subgroup with baseline brain metastases.
Study Design
Phase 3, global, randomized 1:1, open-label. Tarlatamab IV (1 mg step dose, then 10 mg Q2W) vs investigator's choice chemotherapy. Primary endpoint: overall survival. CNS endpoints assessed by post hoc analysis.
Population
Adults with relapsed SCLC after exactly one prior platinum-based line; 44% platinum-resistant (chemotherapy-free interval <90 days; 223/509). Patients with treated/stable brain metastases were eligible, enabling the intracranial efficacy analysis.
Intervention
Experimental: Tarlatamab (DLL3 BiTE), Q2W after step-up dosing. Control: Topotecan, lurbinectedin, or amrubicin per investigator choice.
Endpoints
Primary: Overall survival. Key secondary: PFS, ORR, safety, PROs. Post hoc (ASCO 2026): time to CNS progression/death, intracranial response, and OS in patients with brain metastases.
Results — CNS Post Hoc (#ASCO26) & Primary OS Readout
CNS Post Hoc — Intracranial Efficacy (#ASCO26, Abstract 8006)
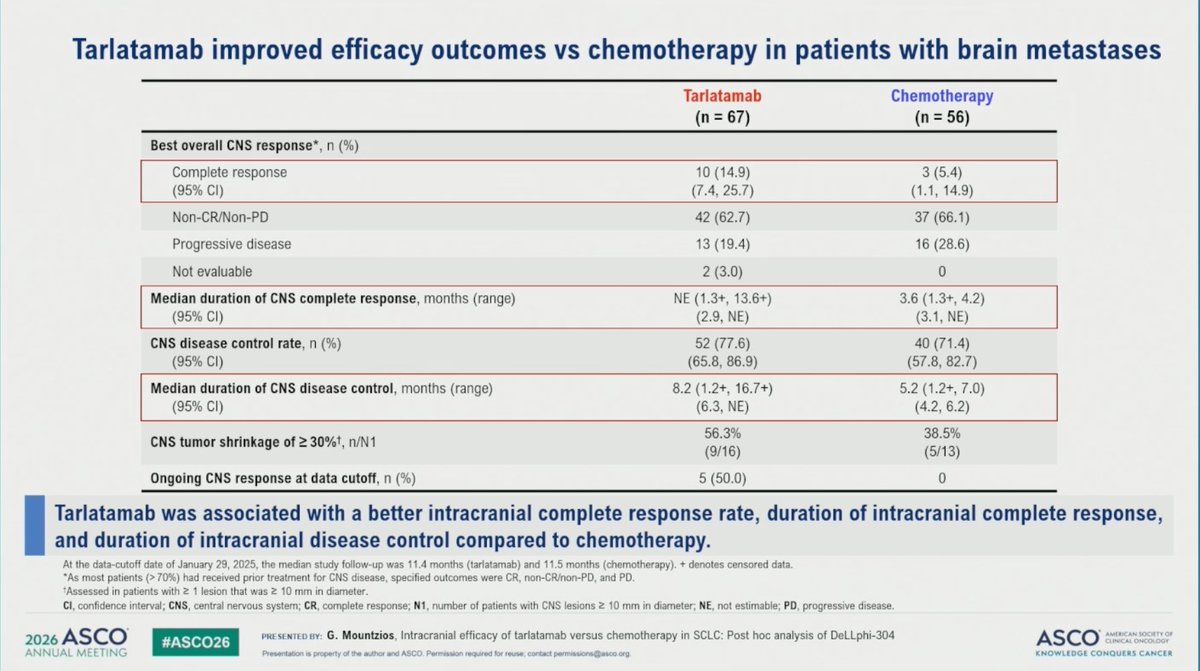
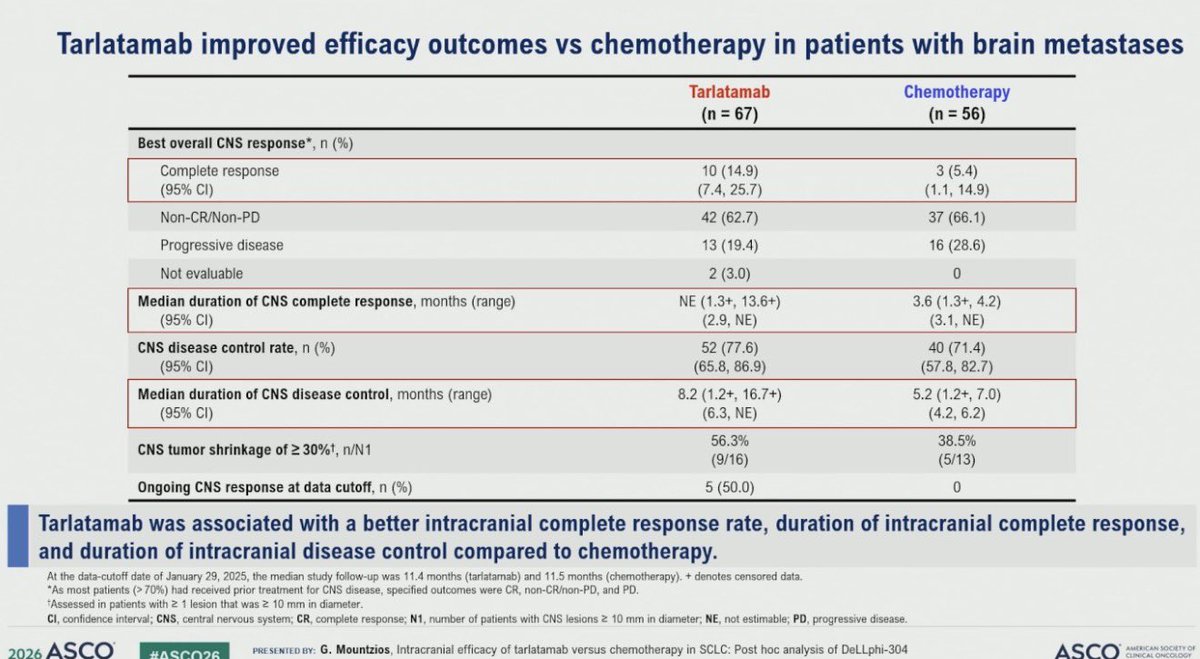
In this post hoc analysis — the first CNS-efficacy data for a T-cell engager in SCLC — tarlatamab delayed time to CNS progression/death versus chemotherapy across the overall (ITT) population — median CNS PFS not reached vs 7.2 months (HR 0.54; 95% CI 0.39–0.75). Among patients with baseline brain metastases (39% of each arm), the intracranial benefit was more pronounced: median CNS PFS 6.5 vs 4.2 months (HR 0.40; 95% CI 0.24–0.66); intracranial complete response 15% vs 5%; CNS tumor shrinkage (≥30%) 56% vs 38%; CNS duration of disease control 8.2 vs 5.2 months; and overall survival 13.9 vs 6.8 months (HR 0.51; 95% CI 0.34–0.74) favoring tarlatamab.
Brain-mets pts: CNS PFS 6.5 vs 4.2 mo · HR 0.40 · iCR 15% vs 5% · OS 13.9 vs 6.8 mo (HR 0.51) · ITT CNS PFS NR vs 7.2 mo · HR 0.54 (0.39–0.75)Sources: Mountzios et al., DeLLphi-304 CNS post hoc, ASCO 2026 Abstract 8006 (J Clin Oncol 44, suppl) · The ASCO Post · OncLive ASCO 2026 coverageOverall Survival (Primary Endpoint — MET, ASCO 2025 / NEJM)
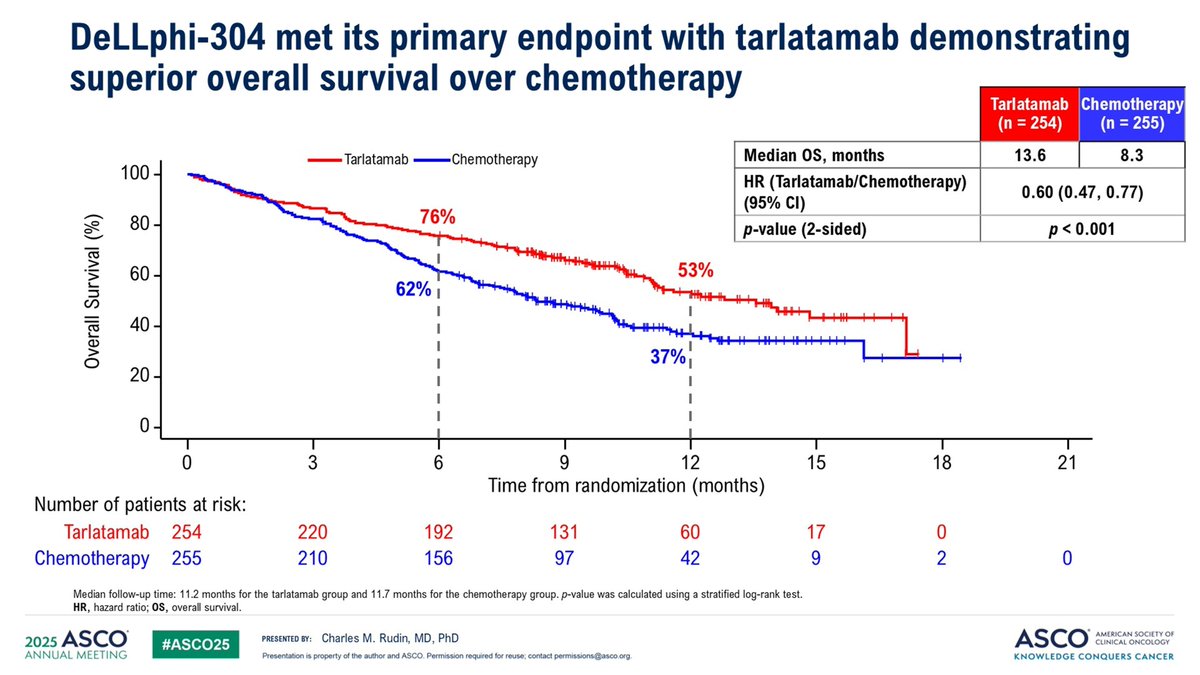
In the pivotal analysis presented at ASCO 2025 and published in NEJM, tarlatamab produced a statistically significant overall-survival benefit versus chemotherapy in 2L SCLC: median OS 13.6 vs 8.3 months (HR 0.60; 95% CI 0.47–0.77; p<0.001). The benefit was consistent regardless of platinum-free interval (OS HR 0.60 for CFI <90 days, 0.65 for ≥90 days).
Median OS 13.6 vs 8.3 mo · HR 0.60 (0.47–0.77) · p<0.001Sources: Mountzios et al., N Engl J Med 2025;393(4):349-361 (doi:10.1056/NEJMoa2502099) · ASCO 2025 oral presentationProgression-Free Survival & Response (ASCO 2025 / NEJM)
Tarlatamab also improved progression-free survival — median PFS 4.2 vs 3.2 months (HR 0.72; 95% CI 0.59–0.88; p<0.001) — and roughly tripled the objective response rate (ORR 27% vs 9%) versus chemotherapy, with more durable responses. Patient-reported dyspnea also improved significantly at week 18 with tarlatamab.
PFS 4.2 vs 3.2 mo · HR 0.72 (0.59–0.88) · ORR 27% vs 9%Sources: DeLLphi-304, N Engl J Med 2025;393(4):349-361 · FDA Imdelltra prescribing informationSafety & Tolerability
Tarlatamab was associated with fewer severe (Grade ≥3) adverse events than chemotherapy (54% vs 80%), largely reflecting reduced hematologic toxicity. The characteristic tarlatamab toxicities are cytokine release syndrome (CRS, 56% — predominantly Grade 1–2; Grade ≥3 only 1.2%), concentrated around the step-up dosing period, and immune effector cell–associated neurotoxicity syndrome (ICANS) — both carry boxed warnings and are managed with monitoring and supportive care. Serious adverse reactions occurred in 52% of patients; 6% discontinued tarlatamab due to an adverse reaction.
Grade ≥3 AEs 54% vs 80% chemo · CRS 56% (Gr≥3 1.2%) · 6% discontinuedSources: DeLLphi-304, N Engl J Med 2025;393(4):349-361 · FDA Imdelltra prescribing information (rev. 11/2025)Clinical Implications
DeLLphi-304 establishes tarlatamab as a standard second-line option in relapsed SCLC, an area with historically poor outcomes. The ASCO 2026 CNS data are especially meaningful because brain metastases are common in SCLC and have been difficult to control with chemotherapy — multiple KOLs called the intracranial signal one of the most clinically relevant SCLC updates of the meeting. The findings support tarlatamab use in patients with CNS involvement and reinforce the confirmatory Phase 3 basis for its regulatory standing.
Standard 2L SCLC option · Meaningful intracranial control in brain-mets ptsSources: ASCO 2026 Abstract 8006 discussion · The ASCO Post · KOL commentary (#ASCO26)Key KOL Sentiments — DeLLphi-304




















DeLLphi-304 FAQ
What is the DeLLphi-304 trial?
DeLLphi-304 is a Phase 3 randomized trial (NCT05740566) comparing tarlatamab (Imdelltra), a DLL3-targeting bispecific T-cell engager, with standard chemotherapy in patients with relapsed small cell lung cancer after platinum-based therapy. Overall survival was the primary endpoint.
What overall survival benefit did DeLLphi-304 show?
Tarlatamab produced a statistically significant overall-survival benefit: median OS was 13.6 versus 8.3 months (HR 0.60; 95% CI 0.47-0.77; p<0.001). It also improved progression-free survival (4.2 vs 3.2 months; HR 0.72) and roughly tripled the objective response rate (27% vs 9%) versus chemotherapy.
What did the ASCO 2026 CNS analysis of DeLLphi-304 find?
At ASCO 2026 (Abstract 8006), a post hoc analysis - the first CNS-efficacy data for a T-cell engager in SCLC - showed tarlatamab delayed intracranial progression versus chemotherapy across the overall population (CNS PFS HR 0.54) and, among patients with baseline brain metastases, an even larger benefit (CNS PFS HR 0.40). Brain metastases are common in SCLC, which is why KOLs highlighted this signal.
Is tarlatamab FDA approved for small cell lung cancer?
Yes. Tarlatamab (Imdelltra) is FDA approved for extensive-stage small cell lung cancer that has progressed on or after platinum-based chemotherapy. It initially received accelerated approval in May 2024, and on November 19, 2025 the FDA converted it to traditional approval in the relapsed setting, based on the DeLLphi-304 overall-survival benefit.
What is the safety profile of tarlatamab in DeLLphi-304?
Tarlatamab caused fewer severe (Grade >=3) adverse events than chemotherapy (54% vs 80%), largely reflecting less hematologic toxicity. Its characteristic toxicity is cytokine release syndrome, which occurred in 56% of patients but was predominantly Grade 1-2 (Grade >=3 only 1.2%) and concentrated around the step-up dosing period; immune effector cell-associated neurotoxicity syndrome (ICANS) can also occur, so monitoring during initiation is required.