Phase 3 global, randomized trial of single-agent teclistamab (Tecvayli) versus investigator's choice of PVd or Kd in patients with relapsed/refractory multiple myeloma after 1–3 prior lines, all anti-CD38- and lenalidomide-exposed. Presented at #ASCO26 (Abstract 7507, Mina) and published in NEJM: primary endpoint PFS met with HR 0.29 (18-mo PFS 69.8% vs 26.9%) and a significant OS benefit (HR 0.60).
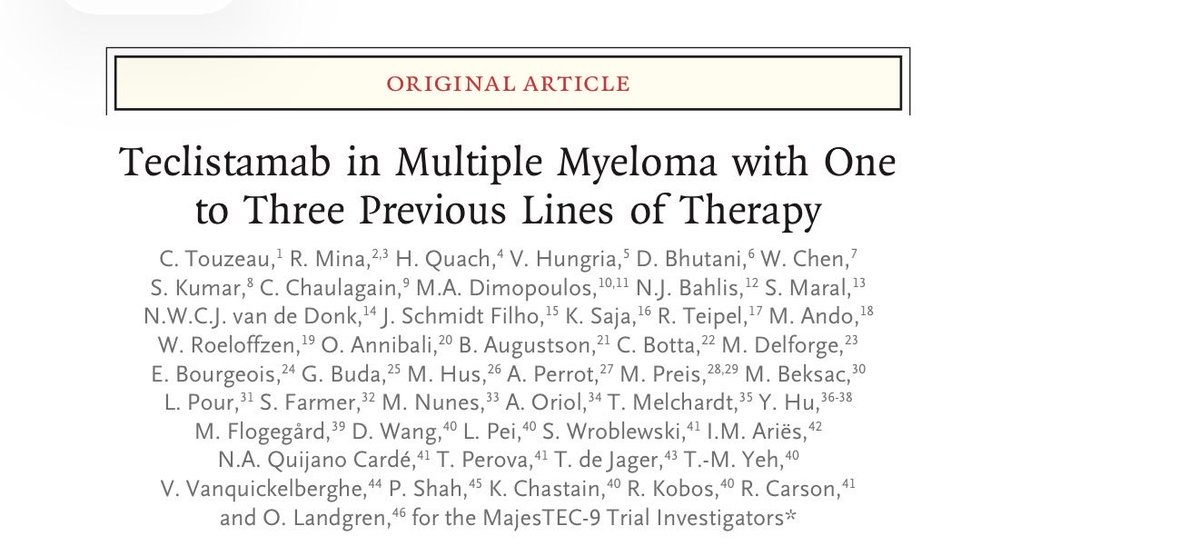
[NEJM title + Table 1, MajesTEC-9] Teclistamab in Multiple Myeloma with One to Three Previous Lines of Therapy (MajesTEC-9 Trial Investigators). Baseline ITT: Teclistamab N=296 / PVd or Kd N=297 / Total N=593. Median age 70; >=75 y 28.4%/30.0%. ECOG 0: 52.7%/45.5%. ISS III 14.2%/15.2%. High cytogenetic risk 35.7%/35.1%. >=1 soft-tissue plasmacytoma 18.2%/21.9%. >=60% BM plasma cells 10.6%/13.6%.
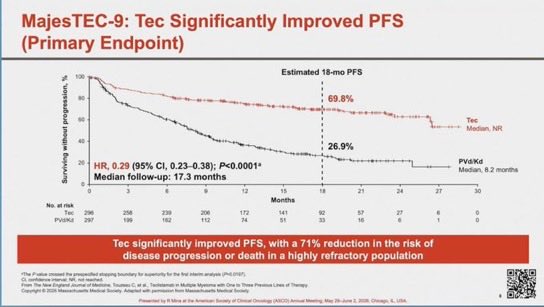
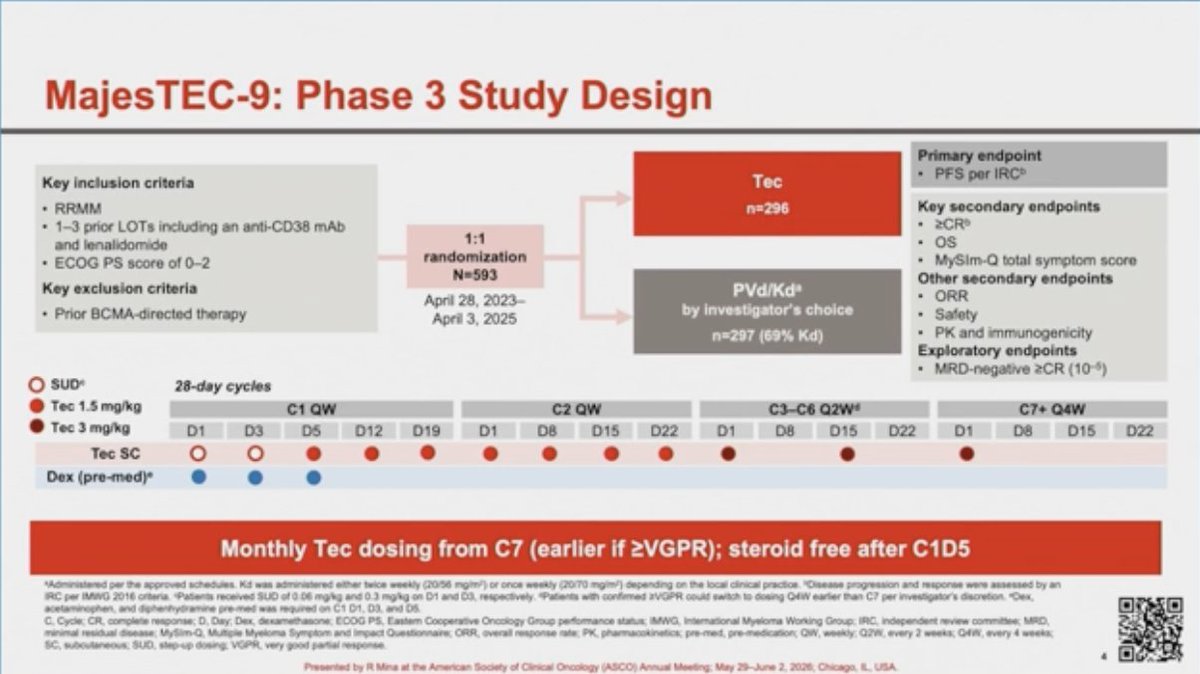
[Slide 1] MajesTEC-9: Phase 3 Study Design
Key inclusion criteria: RRMM; 1-3 prior LOTs including an anti-CD38 mAb and lenalidomide; ECOG PS score of 0-2. Key exclusion criteria: Prior BCMA-directed therapy.
1:1 randomization N=593 (April 28, 2023 - April 3, 2025): Tec n=296 vs PVd/Kd by investigator's choice n=297 (69% Kd).
Primary endpoint: PFS per IRC. Key secondary endpoints: >=CR, OS, MySIM-Q total symptom score. Other secondary endpoints: ORR, Safety, PK and immunogenicity. Exploratory endpoint: MRD-negative >=CR (10^-5).
Monthly Tec dosing from C7 (earlier if >=VGPR); steroid free after C1D5.
Presented by R Mina at ASCO Annual Meeting, May 29-June 2, 2026.
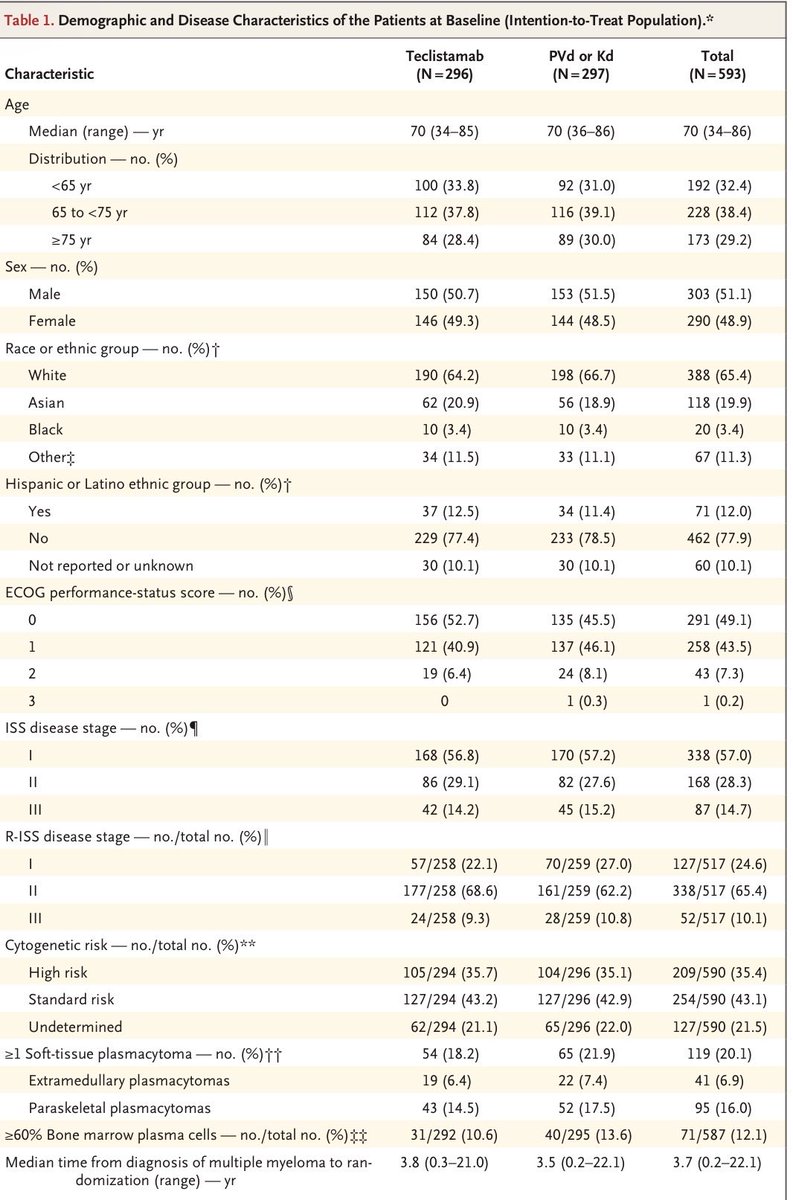
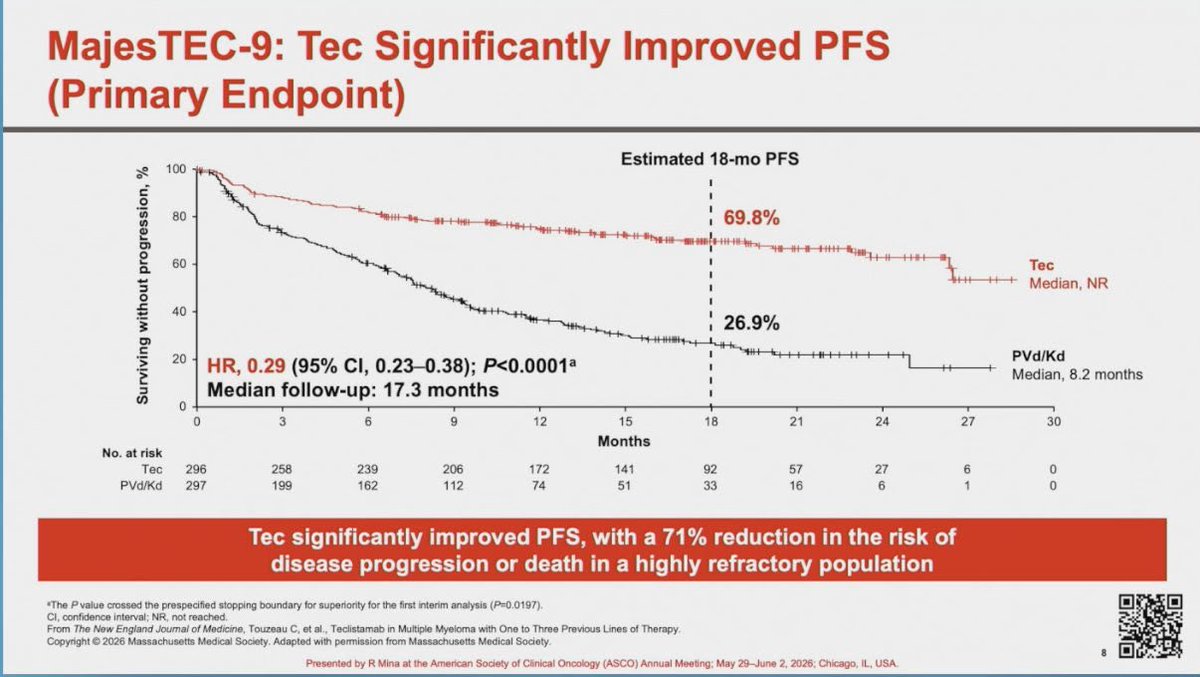
[Slide 2] MajesTEC-9: Tec Significantly Improved PFS (Primary Endpoint)
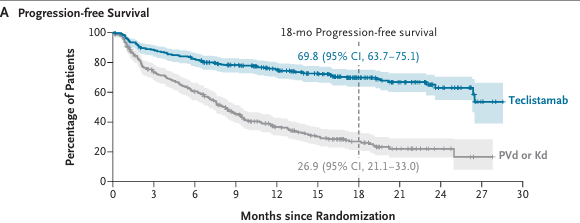
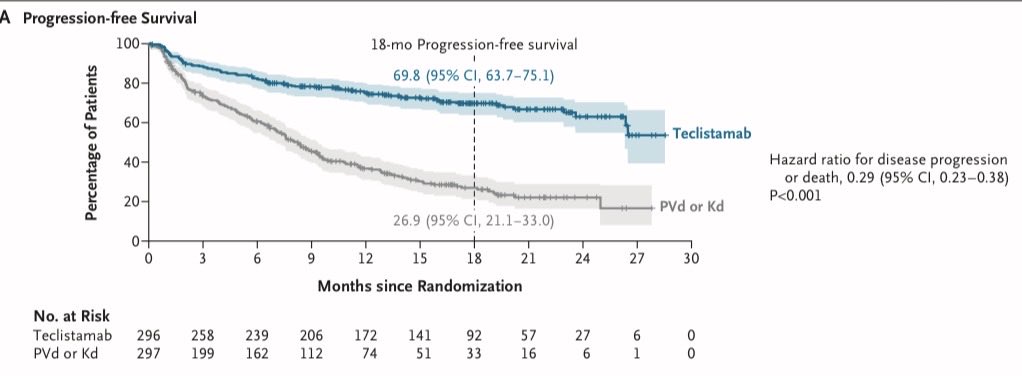
Estimated 18-mo PFS: Tec 69.8%, Median NR; PVd/Kd 26.9%, Median 8.2 months. HR 0.29 (95% CI, 0.23-0.38); P<0.0001. Median follow-up: 17.3 months.
Tec significantly improved PFS, with a 71% reduction in the risk of disease progression or death in a highly refractory population.
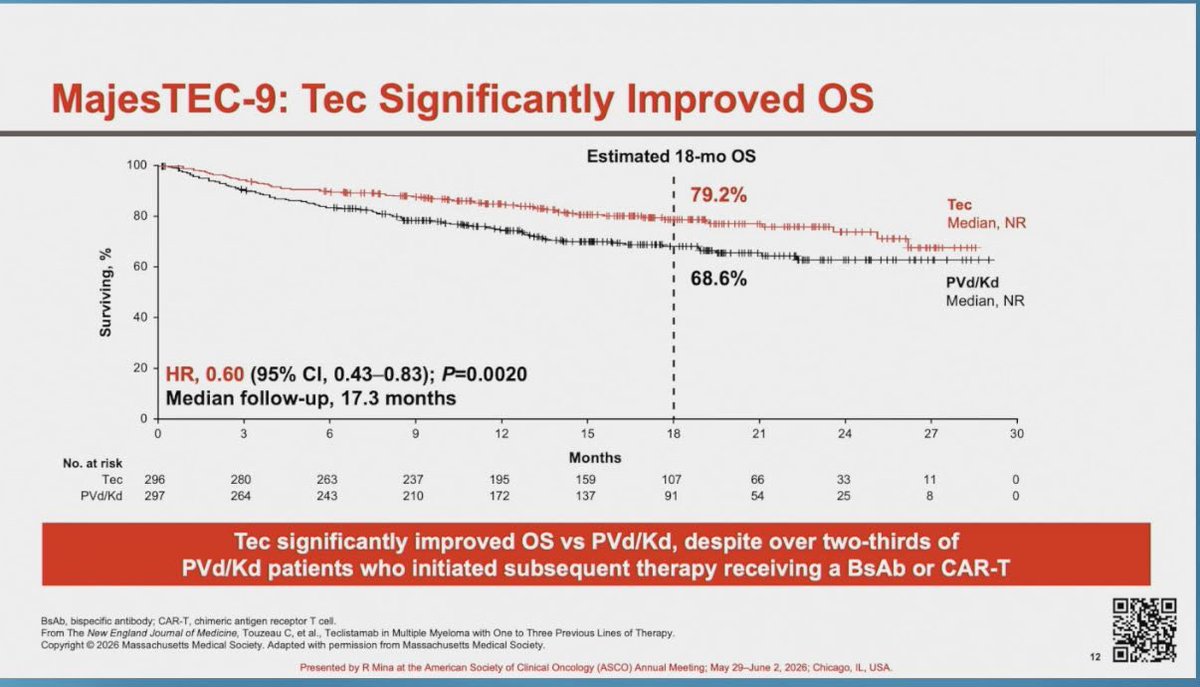
[Slide 3] MajesTEC-9: Tec Significantly Improved OS
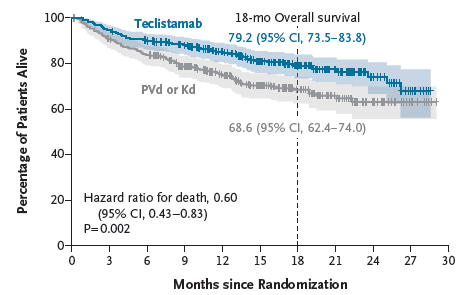
Estimated 18-mo OS: Tec 79.2%, Median NR; PVd/Kd 68.6%, Median NR. HR 0.60 (95% CI, 0.43-0.83); P=0.0020. Median follow-up: 17.3 months.
Tec significantly improved OS vs PVd/Kd, despite over two-thirds of PVd/Kd patients who initiated subsequent therapy receiving a BsAb or CAR-T.
[Slide 4] MajesTEC-9: Overall Safety Profile (Tec n=291, PVd/Kd n=283)
Any TEAE: 290 (99.7%) vs 277 (97.9%); Grade 3/4: 247 (84.9%) vs 216 (76.3%). Neutropenia 182 (62.5%) / G3/4 158 (54.3%) vs 81 (28.6%) / 63 (22.3%). CRS 192 (66.0%) / G3/4 2 (0.7%) vs 0. CRS mostly low grade, all resolved with no discontinuation; Grade 1/2 (48.8%/16.5%), grade 3 (0.7%), no grade 4/5. ICANS infrequent, generally low grade; Grade 1/2 (2.4%/1.4%), grade 3 (0.3%). Discontinuations due to TEAEs 10.7% Tec vs 13.1% PVd/Kd. Death due to PD 8.6% Tec vs 18.7% PVd/Kd. Grade 5 TEAEs 6.5% Tec vs 3.5%. The safety profile was consistent with the known profile of Tec monotherapy.
[MajesTEC-9: TRUTH vs MYTH — Dr. Fun + G / PSNS] MYTHS: (1) MajesTEC-9 was a triple-class refractory study — only ~35% triple-class refractory; (2) all patients were dara-refractory — ~77% anti-CD38 refractory; (3) all patients len-refractory — ~80%; (4) MajesTEC-9 shows Tec superior to CAR-T — CAR-T was never the comparator; (5) GPRC5D unknown. TRUTHS: (1) Teclistamab highly effective — PFS and OS benefit; (2) can be used earlier (1-3 prior lines); (3) many patients were anti-CD38 refractory; (4) infections remain a major concern — Grade 3/4 infections ~41.6%; (5) need dedicated first-relapse studies. Bottom line: MajesTEC-9 is a major advance that moves teclistamab earlier; next frontier is choosing the right therapy for the right patient at the right time.
[MajesTEC-9 infographic, NEJM 2026] Teclistamab Monotherapy Earlier-Line RRMM. After 1-3 prior lines, all exposed to anti-CD38 + lenalidomide. BCMA BISPECIFICS MOVE EARLIER. BETTER SURVIVAL. Phase 3 randomized N=593: Teclistamab SC monotherapy (n=296) vs PVd or Kd investigator's choice (n=297). Primary endpoint PFS by independent review committee. 18-month PFS 69.8% Teclistamab vs 26.9% PVd/Kd, HR 0.29 (95% CI 0.23-0.38), P<0.001. 18-month OS 79.2% vs 68.6%, HR for death 0.60 (95% CI 0.43-0.83), P=0.002. Complete response or better 65.9% vs 16.8%, P<0.001. SAFETY: Grade 3/4 infections 41.6% vs 29.0%; CRS 66.0% mostly grade 1-2; ICANS 4.1% any grade; Grade 3/4 AEs 84.9% vs 76.3%. Takeaway: Teclistamab significantly improved PFS and OS vs PVd or Kd in earlier-line, double-refractory RRMM. Deep responses, meaningful survival benefit, infections common — infection prevention is not optional. @DrRishabhOnco
[Comparative infographic — PSNS Square] MajesTEC-3 vs MajesTEC-9 vs CARTITUDE-4: Different Patients. Different Biology. Different Questions. WHO WAS STUDIED: MajesTEC-3 (Tec+Dara, 1-3 prior lines), MajesTEC-9 (Tec mono, 1-3 prior lines), CARTITUDE-4 (cilta-cel, 1-3 prior lines, len-refractory). DEPTH OF RESPONSE & OUTCOMES (cross-trial, not head-to-head): ORR ~85% (Tec mono) vs ~95% (cilta-cel); >=CR 65.9%; MRD negativity 38.5%. TELISTAMAB vs CAR-T trade-offs: off-the-shelf/immediate vs one-time but manufacturing/bridging. TAKE-HOME: MajesTEC-9 establishes teclistamab monotherapy as an effective off-the-shelf option earlier; CAR-T (CARTITUDE-4) offers one-and-done. The real story: which immunotherapy is best suited for which patient and when.
[Table 1. Demographic and Disease Characteristics at Baseline (ITT), MajesTEC-9] Teclistamab N=296 / PVd or Kd N=297 / Total N=593. Median age 70 (34-85). Age >=75 y 28.4% vs 30.0%. Male 50.7% vs 51.5%. White 64.2%/66.7%; Asian 20.9%/18.9%. ECOG 0: 52.7%/45.5%. ISS stage III 14.2%/15.2%. High cytogenetic risk 35.7%/35.1%. >=1 soft-tissue plasmacytoma 18.2%/21.9% (extramedullary 6.4%/7.4%). >=60% BM plasma cells 10.6%/13.6%. Median time from MM diagnosis to randomization 3.8 vs 3.5 y. No. of prior lines: median 2 (1-3); 1 line 21.6%/21.5%; 2-3 lines 78.4%/78.5%. Prior PI 86.5%/85.5%; prior IMiD 100%; prior anti-CD38 mAb 100%. Refractory: any IMiD 82.8%/84.5% (lenalidomide 79.1%/80.8%); any anti-CD38 85.2%/84.8% (daratumumab 77.4%/75.8%); triple-class refractory 34.5%/33.0%; refractory to last line 92.6%/91.9%.
[MajesTEC-9 NEJM figures thread] PFS (Fig 1A): 18-mo PFS 69.8% (95% CI 63.7-75.1) Teclistamab vs 26.9% (95% CI 21.1-33.0) PVd/Kd; HR 0.29 (0.23-0.38), P<0.001. MRD-negative (10^-5) CR rate (ITT): Teclistamab 38.5% vs PVd/Kd 6.7%; RR 5.76 (95% CI 3.69-9.01), OR 8.56 (95% CI 5.14-14.26). Response (Table 2): ORR, >=VGPR, >=CR markedly higher with teclistamab. OS (Fig 2): 18-mo OS 79.2% (73.5-83.8) vs 68.6% (62.4-74.0); HR for death 0.60 (0.43-0.83), P=0.002; median OS not reached either arm at 17.3 mo follow-up.
[Slide 1] The New England Journal of Medicine — ORIGINAL ARTICLE
Teclistamab in Multiple Myeloma with One to Three Previous Lines of Therapy
C. Touzeau, R. Mina, H. Quach, V. Hungria, D. Bhutani, W. Chen, S. Kumar, C. Chaulagain, M.A. Dimopoulos, N.J. Bahlis, S. Maral, N.W.C.J. van de Donk, J. Schmidt Filho, K. Saja, R. Teipel, M. Ando, W. Roeloffzen, O. Annibali, B. Augustson, C. Botta, M. Delforge, E. Bourgeois, G. Buda, M. Hus, A. Perrot, M. Preis, M. Beksac, L. Pour, S. Farmer, M. Nunes, A. Oriol, T. Melchardt, Y. Hu, M. Flogegard, D. Wang, L. Pei, S. Wroblewski, I.M. Aries, N.A. Quijano Carde, T. Perova, T. de Jager, T.-M. Yeh, V. Vanquickelberghe, P. Shah, K. Chastain, R. Kobos, R. Carson, and O. Landgren, for the MajesTEC-9 Trial Investigators
[Slide 2] A Progression-free Survival
18-mo Progression-free survival: Teclistamab 69.8 (95% CI, 63.7-75.1); PVd or Kd 26.9 (95% CI, 21.1-33.0)
Hazard ratio for disease progression or death, 0.29 (95% CI, 0.23-0.38) P<0.001
No. at Risk Teclistamab 296 258 239 206 172 141 92 57 27 6 0; PVd or Kd 297 199 162 112 74 51 33 16 6 1 0
[Slide 3] B Subgroup Analysis of Progression-free Survival — Hazard Ratio for Disease Progression or Death (95% CI)
Age <65 yr 0.29 (0.19-0.45); >=65 yr 0.29 (0.21-0.40). Sex Male 0.35 (0.24-0.49); Female 0.26 (0.18-0.37). No. of lines of previous therapy 1: 0.34 (0.18-0.64); 2 or 3: 0.29 (0.22-0.38). Refractory to anti-CD38 No 0.16 (0.07-0.35); Yes 0.32 (0.24-0.42). Refractory to lenalidomide No 0.30 (0.16-0.53); Yes 0.30 (0.23-0.40). Cytogenetic risk High risk 0.27 (0.18-0.41); Standard risk 0.34 (0.22-0.52). Teclistamab Better / PVd or Kd Better
[Slide 4] Figure 2. Overall Survival. 18-mo Overall survival: Teclistamab 79.2 (95% CI, 73.5-83.8); PVd or Kd 68.6 (95% CI, 62.4-74.0). Hazard ratio for death, 0.60 (95% CI, 0.43-0.83) P=0.002. At a median follow-up of 17.3 months, the median overall survival was not reached in either trial group.
cancernetwork®
home of the journal ONCOLOGY
3 ABSTRACTS TO WATCH
ASCO 2026 I Multiple Myeloma
Abstract 7507
MajesTEC-9
Phase 3: Teclistamab monotherapy vs PVd/Kd in
relapsed/refractory multiple myeloma (1-3 prior lines)
Presenter: Roberto Mina, MD
Abstract 7510
Optec/Optal
Phase 2: Outpatient teclistamab or talquetamab with prophylactic
tocilizumab in RRMM
Presenter: Peter Forsberg, MD
Abstract LBA7506
SUCCESSOR-2
Phase 3: Mezigdomide + carfilzomib + dexamethasone (Mezikd) vs
Kd in RRMM
Presenter: Paul G. Richardson, MD
Read more on CancerNetwork.com
[MajesTEC-9 visual abstract] Phase 3 Teclistamab Monotherapy vs Standard of Care in Early Relapsed/Refractory Multiple Myeloma. Patients with 1-3 prior lines, anti-CD38- and lenalidomide-exposed/refractory RRMM. STUDY DESIGN: N=593 randomized 1:1. Teclistamab step-up dosing then 3 mg/kg weekly, C3-6 q2-4w, C7+ q4w vs investigator's choice PVd or Kd. Median age 70 y; median prior LOTs 2; len-refractory 80%; anti-CD38-refractory 85%; refractory to last LOT 92%; median follow-up 17.3 mo. Primary endpoint PFS by IRC. KEY EFFICACY: PFS HR 0.29 (95% CI 0.23-0.38), P<0.0001, median PFS not reached vs 8.2 months; 18-mo PFS 69.8% vs 26.9%. OS HR 0.60 (95% CI 0.43-0.83), P=0.0020. >=CR 65.9% vs 16.8%, OR 10.42 (95% CI 6.89-15.76), P<0.0001. Among 174 in PVd/Kd arm with subsequent therapy, 68.4% later received a bispecific or CAR-T. SAFETY: on treatment at cutoff 65.3% vs 24.0%; median treatment duration 13.1 vs 7.0 mo; any TEAE 99.7% vs 97.9%; Grade 3/4 TEAEs 84.9% vs 76.3%; Grade 5 TEAEs 6.5% vs 3.5%; discontinuation due to TEAEs 10.7% vs 13.1%; Grade 3/4 infections 41.6% vs 29.0%. TEC-specific: CRS 66.0% overall (Gr1 48.8%, Gr2 16.5%); ICANS 4.1% overall (Gr1 2.4%, Gr2 1.4%). Grade >=3 infections decreased over time.
MajesTEC-9 (NCT05572515) is a Phase 3, global, randomized, open-label trial of single-agent teclistamab (Tecvayli), a BCMA×CD3 bispecific antibody, versus investigator's choice of pomalidomide-bortezomib-dexamethasone (PVd) or carfilzomib-dexamethasone (Kd) in patients with relapsed/refractory multiple myeloma after 1–3 prior lines of therapy. All patients were exposed to a proteasome inhibitor, an immunomodulatory drug, and an anti-CD38 monoclonal antibody. The trial randomized 593 patients 1:1 (296 teclistamab vs 297 PVd/Kd). The primary endpoint is progression-free survival by independent review committee. Primary results were presented at #ASCO26 (Abstract 7507) and published simultaneously in the New England Journal of Medicine.
Study Design
Phase 3, global, randomized 1:1, open-label. Teclistamab SC step-up dosing then 3 mg/kg weekly (cycles 3–6 every 2–4 weeks by response; cycle 7+ every 4 weeks) vs investigator's choice of PVd or Kd. Median follow-up 17.3 months.
Population
n=593 with RRMM after 1–3 prior lines (median 2). Median age 70 y. Lenalidomide-refractory ~80%, anti-CD38-refractory ~85%, triple-class refractory ~34%, refractory to last line ~92%. All PI-, IMiD-, and anti-CD38-exposed.
Intervention
Experimental: Single-agent teclistamab SC (BCMA×CD3 bispecific), step-up then weekly, with response-adapted de-intensification. Control: Investigator's choice of PVd or Kd.
Endpoints
Primary: PFS by independent review committee. Key secondary: overall survival, ≥CR rate, MRD-negative CR, safety. Hierarchical testing of PFS then OS.
Efficacy & Safety
Primary Results — #ASCO26 (Abstract 7507) / NEJM
INVESTIGATIONALEarlier-line indication not yet FDA-approved · Teclistamab IS FDA-approved in later-line RRMM (MajesTEC-1)
MajesTEC-9 is the first Phase 3 trial moving teclistamab into the earlier-line (1–3 prior) relapsed/refractory setting. Teclistamab (Tecvayli) is FDA-approved as monotherapy for adults with RRMM who have received at least 4 prior lines of therapy (including a PI, an IMiD, and an anti-CD38 antibody), based on MajesTEC-1. The earlier-line use studied here is investigational pending regulatory review.
Single-agent teclistamab produced a statistically significant and clinically meaningful improvement in PFS versus investigator's choice of PVd or Kd, with a hazard ratio of 0.29 (95% CI 0.23–0.38; P<0.001) — a 71% reduction in the risk of disease progression or death. The 18-month PFS rate was 69.8% (95% CI 63.7–75.1) with teclistamab vs 26.9% (95% CI 21.1–33.0) with PVd/Kd; median PFS was not reached vs ~8.2 months. The benefit was consistent across all prespecified subgroups, including lenalidomide-refractory (HR 0.30), anti-CD38-refractory (HR 0.32), high-risk cytogenetics (HR 0.27), and 1 vs 2–3 prior lines. Depth of response also favored teclistamab: ≥CR 65.9% vs 16.8% (OR 10.42) and MRD-negative (10⁻⁵) CR 38.5% vs 6.7% (OR 8.56).
Overall survival also significantly favored teclistamab, with a hazard ratio for death of 0.60 (95% CI 0.43–0.83; P=0.002). The 18-month OS rate was 79.2% (95% CI 73.5–83.8) vs 68.6% (95% CI 62.4–74.0); median OS was not reached in either arm at a median follow-up of 17.3 months. Notably, among the 174 patients in the PVd/Kd arm who received subsequent therapy, 68.4% later received a bispecific antibody or CAR-T — making the OS separation despite substantial crossover-equivalent salvage particularly meaningful.
Safety & Tolerability (Safety Population, n=291 vs 283)
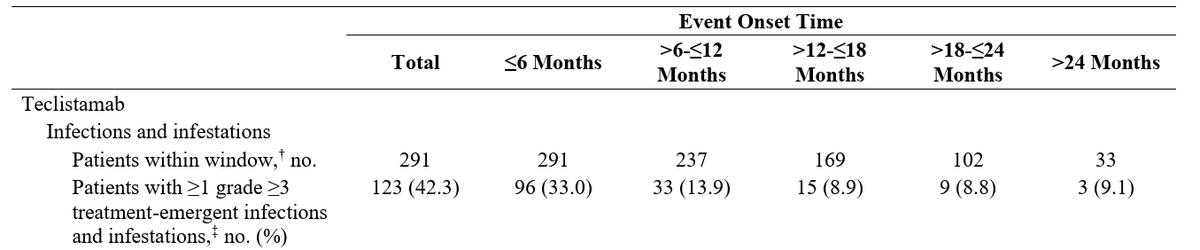
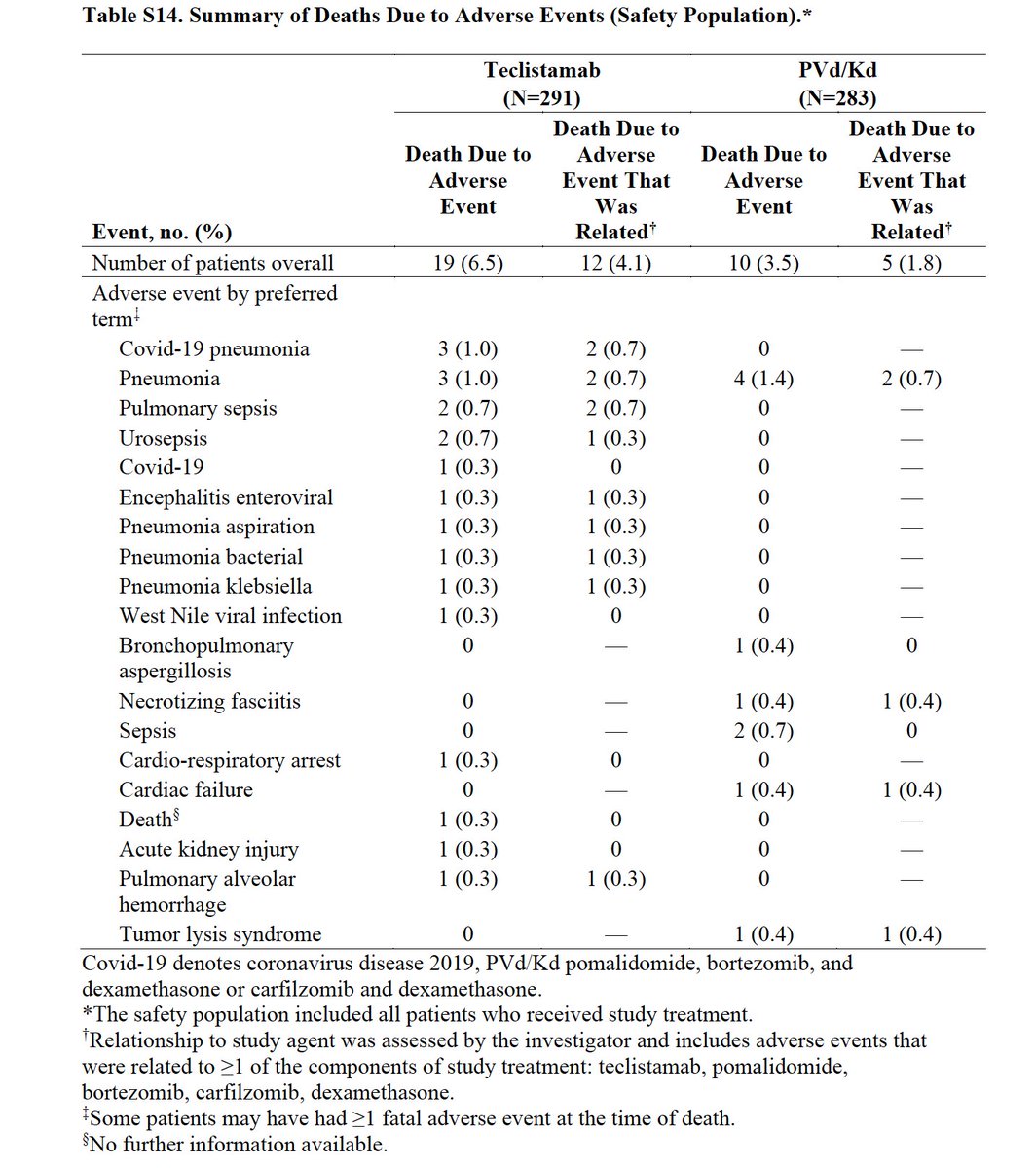
The safety profile was consistent with the established teclistamab experience. Grade 3/4 adverse events occurred in 84.9% of teclistamab patients vs 76.3% with PVd/Kd. Cytokine release syndrome occurred in 66.0% (mostly grade 1–2; grade 3/4 only 0.7%) and ICANS/neurotoxicity in 4.1% (any grade). Hematologic toxicity included neutropenia (62.5%, grade 3/4 54.3%). Grade 3/4 infections were 41.6% vs 29.0% — the dominant safety concern in this BCMA-bispecific population — and deaths due to adverse events were 6.5% vs 3.5% (mostly infections, including COVID-19 pneumonia and sepsis). Per the investigators, grade ≥3 infections decreased over time with prophylaxis, but infection prevention is not optional with this regimen.
MajesTEC-9 is the first Phase 3 trial to move a BCMA bispecific into the earlier-line (1–3 prior) relapsed/refractory setting, where it more than doubled 18-month PFS and improved OS versus standard PI/IMiD triplets and doublets. Several KOLs framed it as practice-defining for double-class–exposed RRMM, while also emphasizing the trade-offs: it was not a head-to-head against CAR-T (CARTITUDE-4), the comparator arms were viewed by some as suboptimal, and the infection burden demands proactive prophylaxis. The result strengthens the case for off-the-shelf, immediately available bispecific therapy earlier in the relapsed course, with sequencing versus CAR-T remaining the central open question.