LITESPARK-011 is a Phase 3 trial of belzutifan (Welireg) + lenvatinib versus cabozantinib in advanced clear cell renal cell carcinoma (ccRCC) after prior PD-1/PD-L1 therapy. The combination improved median PFS to 14.8 vs 10.7 months (HR 0.70; p=0.00007), with overall survival trending but not yet significant. This belzutifan + lenvatinib combination is investigational in this setting. Sponsor: Merck (with Eisai).
Discover KOL Sentiment on LITESPARK-011 →Design — Phase 3, open-label; belzutifan (Welireg) + lenvatinib vs cabozantinib, advanced ccRCC after PD-1/PD-L1 therapy (NCT04586231). (pivotal presentation)
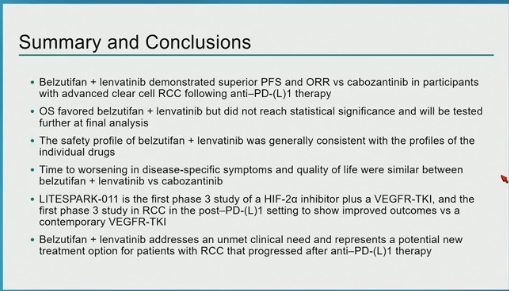
PFS (primary) — Median 14.8 vs 10.7 months; HR 0.70 (95% CI 0.59-0.84; p=0.00007); median follow-up 29.0 mo. (pivotal slide)
Overall survival — Trend at interim: HR 0.85 (95% CI 0.68-1.05; p=0.06075) — not statistically significant; final OS pending. (interim)
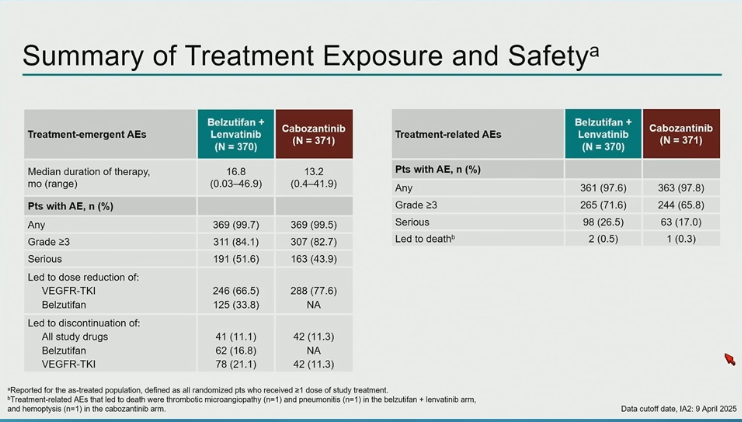
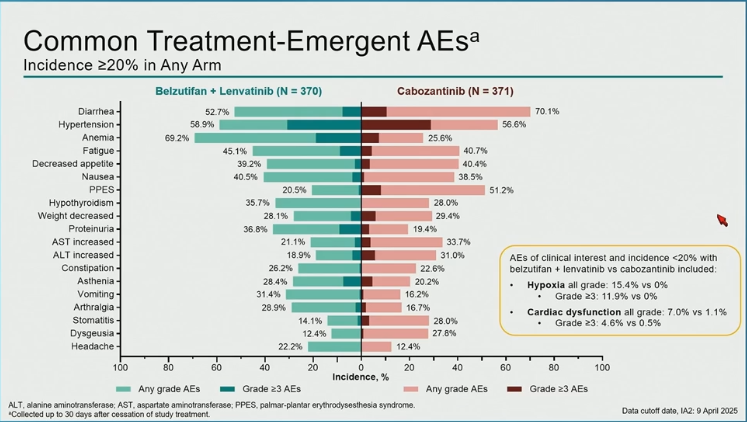
Safety — Consistent with individual agents: belzutifan-related anemia/hypoxia + lenvatinib-related hypertension, diarrhea, fatigue; full Grade >=3 rates pending publication. (pivotal presentation)
Regulatory — INVESTIGATIONAL combination — not FDA approved in this setting. Belzutifan (Welireg) is approved as monotherapy for advanced RCC after PD-1/PD-L1 + VEGF-TKI. (FDA label)
Sponsor / Drug — Merck (with Eisai); belzutifan (HIF-2-alpha inhibitor) + lenvatinib (multikinase VEGFR TKI). (sponsor)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.










Top tweets by impressions — click to view on X
Phase 3 LITESPARK-011: Belzutifan + Lenvatinib vs Cabozantinib in pretreated metastatic clear cell renal cancer #GU25 shows +ve PFS HR 0.75 , OS HR 0.85 (non-significant), ⬆️ RR 53% vs 40%, G3+…
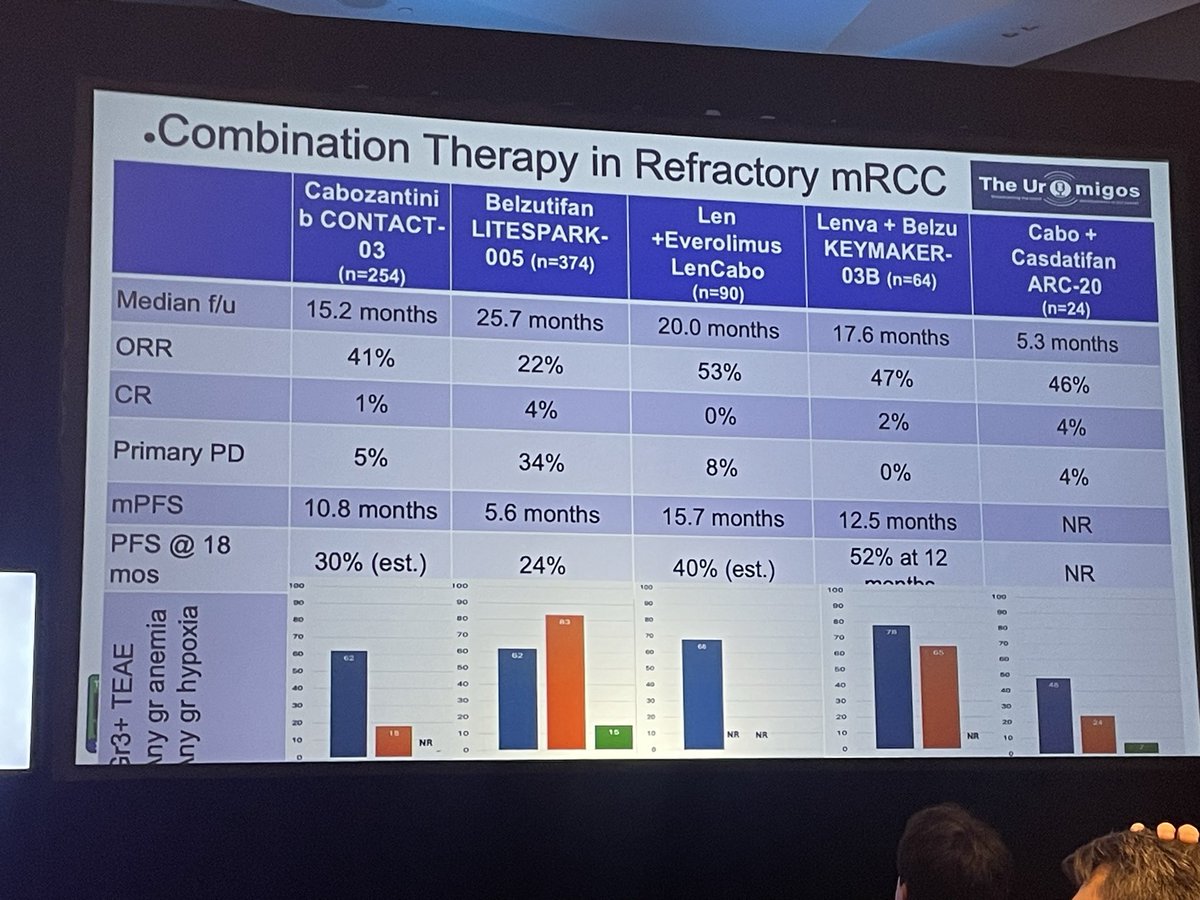
Combination therapy is emerging as a standard in refractory RCC. Combos increase tumor shrinkage endpoints. TKI provides early disease control. CRs are possible but is cure? Toxicity consideration is…
Summary of combination therapy in advanced RCC. Hard to compare phase II trials but clearly multiple options are emerging. #uromigoslive @Uromigos https://t.co/KspHdha2SJ
LITESPARK-011 | Phase III | #ASCOGU26 #GU26
Belzutifan + Lenvatinib vs Cabozantinib in advanced clear-cell RCC post anti–PD-(L)1
A pivotal study redefining the post-IO VEGFR-TKI landscape.
@motzermd …
More from #ASCODailyNews: Phase 3 LITESPARK-011 results support belzutifan + lenvatinib as alt to cabozantinib for pts with aRCC after disease progression on anti–PD-L1/anti–PD-1 therapy. Read the…

Thoughtful discussion by Dr. Katy Beckermann @katy_beckermann on the rationale for HIF-2α inhibitor–based combinations in LITESPARK-011 and -022, and the need to balance efficacy with quality of…

GU @ASCO highlights from #GU26 with @PGrivasMDPhD
✅ CREST/POTOMAC (update)
✅ EV304/KeynoteB15 (new SoC)
✅ LITESPARK-011 & 022
✅ CAPItello-281
Full 🗣️:
⭐️ On OncBrothers & @OncUpdates…

Big morning for Belzutifan🎉#ASCOGU26
#LITESPARK011 combo w/ Lenva vs Cabo in 2L+ s/p IO in mRCC (55% prior TKI)
➕ PFS, ORR, immature OS, 20 pts w/ CR
⚠️15% hypoxia, 2/3 DR TKI, 1/3 DR…

Kidney cancer trial breakdown 🎧
Brian, Tom, and @motzermd analyze the phase 3 LITESPARK-011 trial comparing belzutifan + lenvatinib vs cabozantinib—covering efficacy, safety, and implications for…
Nice slide to show take home message for Monday morning clinic after new RCC data 🙂 @ASCO #GU26 @OncoAlert https://t.co/R4hzBSrbuH
Positions belzutifan + lenvatinib as a potential new standard in advanced ccRCC after PD-1/PD-L1 inhibitor therapy — directly challenging single-agent cabozantinib (current SOC in this setting). Expands role of HIF-2α inhibition beyond VEGF-TKI-refractory monotherapy.
Median PFS was 14.8 months with belzutifan + lenvatinib (95% CI 11.2-16.6) vs. 10.7 months with cabozantinib (9.2-11.1); HR 0.7 (0.59-0.84, P=0.00007). Median follow-up 29.0 months.
Trend toward OS benefit at interim analysis: HR 0.85 (95% CI 0.68-1.05, P=0.06075). Not yet statistically significant; final OS pending further follow-up.
Safety profile consistent with individual agents — belzutifan-related anemia/hypoxia plus lenvatinib-related hypertension, diarrhea, and fatigue. Detailed Grade ≥3 AE rates pending full publication.
Under regulatory review — potential new option in post-IO advanced ccRCC. Positions belzutifan + lenvatinib (investigational in this setting; not FDA approved) as a potential new standard in advanced ccRCC after PD-1/PD-L1 inhibitor therapy — directly challenging single-agent cabozantinib (current SOC in this setting). Expands role of HIF-2α inhibition beyond VEGF-TKI-refractory monotherapy.
LITESPARK-011 is a Phase 3, randomized trial (NCT04586231) of belzutifan (Welireg) plus lenvatinib versus cabozantinib in patients with advanced clear cell renal cell carcinoma (ccRCC) whose disease progressed after PD-1/PD-L1 checkpoint inhibitor therapy.
No. The belzutifan (Welireg) + lenvatinib combination studied in LITESPARK-011 is investigational in this setting. Belzutifan is separately FDA approved as monotherapy for advanced RCC following a PD-1/PD-L1 inhibitor and a VEGF-targeted therapy; the combination with lenvatinib and the head-to-head positioning versus cabozantinib are not approved.
Belzutifan plus lenvatinib improved median progression-free survival to 14.8 months versus 10.7 months with cabozantinib (HR 0.70; 95% CI 0.59-0.84; p=0.00007), at a median follow-up of 29.0 months.
Not yet. At the interim analysis, overall survival trended in favor of belzutifan plus lenvatinib (HR 0.85; 95% CI 0.68-1.05; p=0.06075) but did not reach statistical significance. Final overall survival results are pending further follow-up.
Belzutifan (Welireg), a HIF-2-alpha inhibitor, is developed by Merck. Lenvatinib (Lenvima), a multikinase VEGFR inhibitor, is developed by Eisai; the two companies collaborate on this program.