TALAPRO-3 is a Phase 3, double-blind trial of talazoparib (Talzenna) + enzalutamide (Xtandi) + ADT versus placebo + enzalutamide + ADT in first-line metastatic castration-sensitive prostate cancer with HRR gene alterations. The combination met its primary endpoint (radiographic PFS HR 0.481; median not reached), with overall survival trending but not yet significant. This first-line indication is investigational and not FDA approved. Sponsor: Pfizer (with Astellas).
rPFS (primary) — MET — HR 0.481 (95% CI 0.357-0.647); median rPFS not reached; 3-year rPFS 76.6%. (ASCO GU 2026 slide)
Time to PSA progression — 3-year PSA-progression-free 78.3% vs 62.7%; HR 0.513; p<0.0001. (ASCO GU 2026 slide)
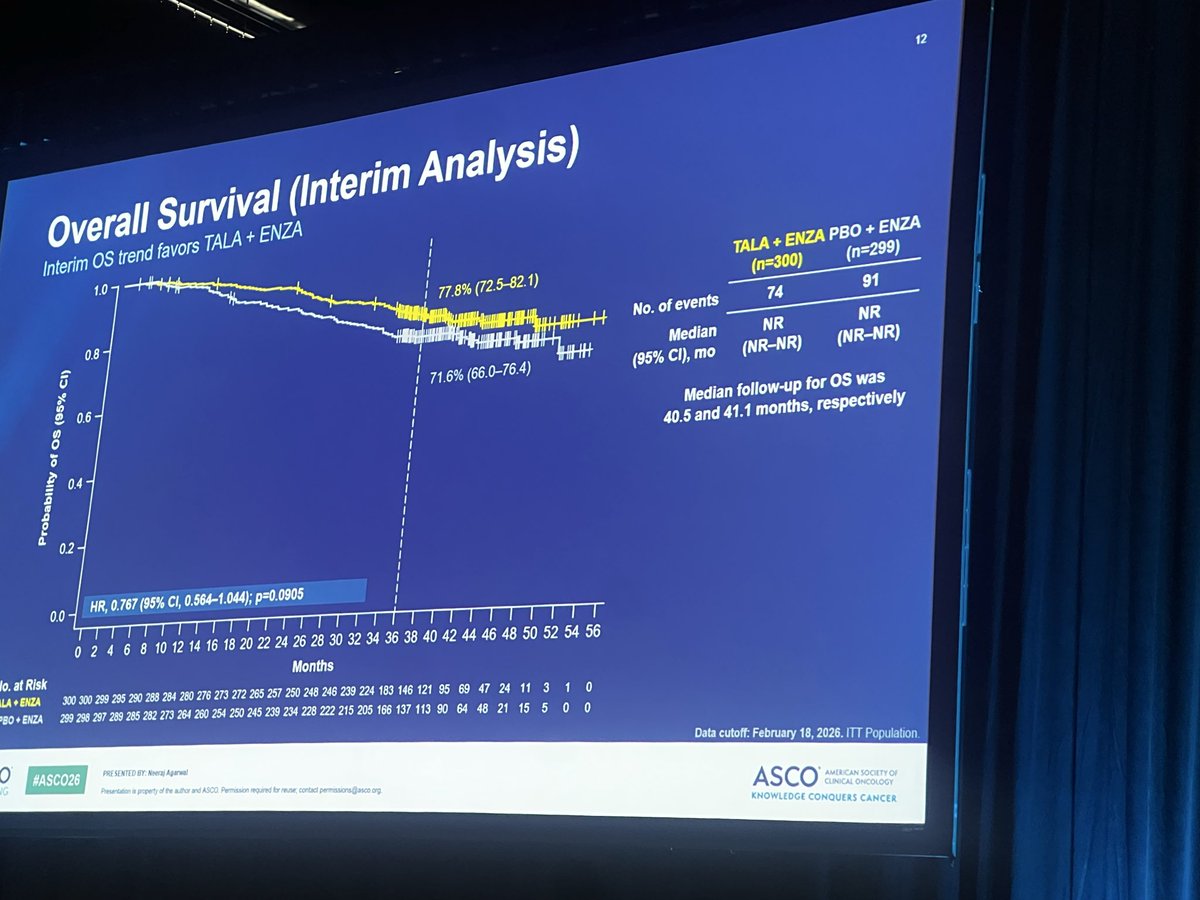
Overall survival — Trending, NOT significant: 3-year OS 77.8% vs 71.6%; HR 0.767 (95% CI 0.564-1.044; p=0.0905). (ASCO GU 2026 slide)
Regulatory — INVESTIGATIONAL for 1L mCSPC — not FDA approved. Talazoparib + enzalutamide is approved only in HRR-mutated mCRPC (TALAPRO-2). (FDA label / TALAPRO-2)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.
UPDATE · First Full Phase 3 Results
Detailed Data from ASCO 2026 LBA5007 · Simultaneous NEJM Publication (May 30, 2026)
TALAPRO-3 builds on the topline results Pfizer announced in March 2026. Today's late-breaking oral presentation at ASCO 2026 (Abstract LBA5007, presented by Neeraj Agarwal, MD FASCO, Huntsman Cancer Institute, University of Utah) delivered the detailed dataset — including subgroup analyses, safety, and patient-reported outcomes — with concurrent publication in the New England Journal of Medicine.
Distinct from TALAPRO-2. TALAPRO-2 was the talazoparib + enzalutamide mCRPC study that received FDA approval in 2023. TALAPRO-3 moves the regimen earlier in the disease course — into first-line metastatic castration-SENSITIVE prostate cancer (mCSPC / mHSPC) with HRR alterations.
Influence Leaders
Top KOLs Discussing TALAPRO-3
Karine Tawagi MD
@drkarinetawagi
4.2K impressions
Toni Choueiri, MD
@drchoueiri
4.1K impressions
Roberto Iacovelli
@DrIacovelli
3.7K impressions
Katy Beckermann
@katy_beckermann
2.5K impressions
Shilpa Gupta
@shilpaonc
1.4K impressions
Yüksel Ürün
@DrYukselUrun
1.4K impressions
Sumanta K. Pal, MD, FASCO
@montypal
836 impressions
Tom Powles
@tompowles1
645 impressions
Conference Presentations
TALAPRO-3 Key Slides & Visuals
Trial slides and infographics shared by KOLs around the ASCO 2026 late-breaking oral presentation (Neeraj Agarwal, Huntsman Cancer Institute, May 30 2026). Click any image to expand.
ASCO®
"In the long term, this [combination
therapy] strategy could help address a
critical gap in care by ensuring that
more patients receive the benefits of
PARP inhibition for mCSPC rather than
relying on later lines of therapy that
many patients may never reach."
Neeraj Agarwal, MD, FASCO
Huntsman Cancer Institute
2026
ASCO
ANNUAL MEETING
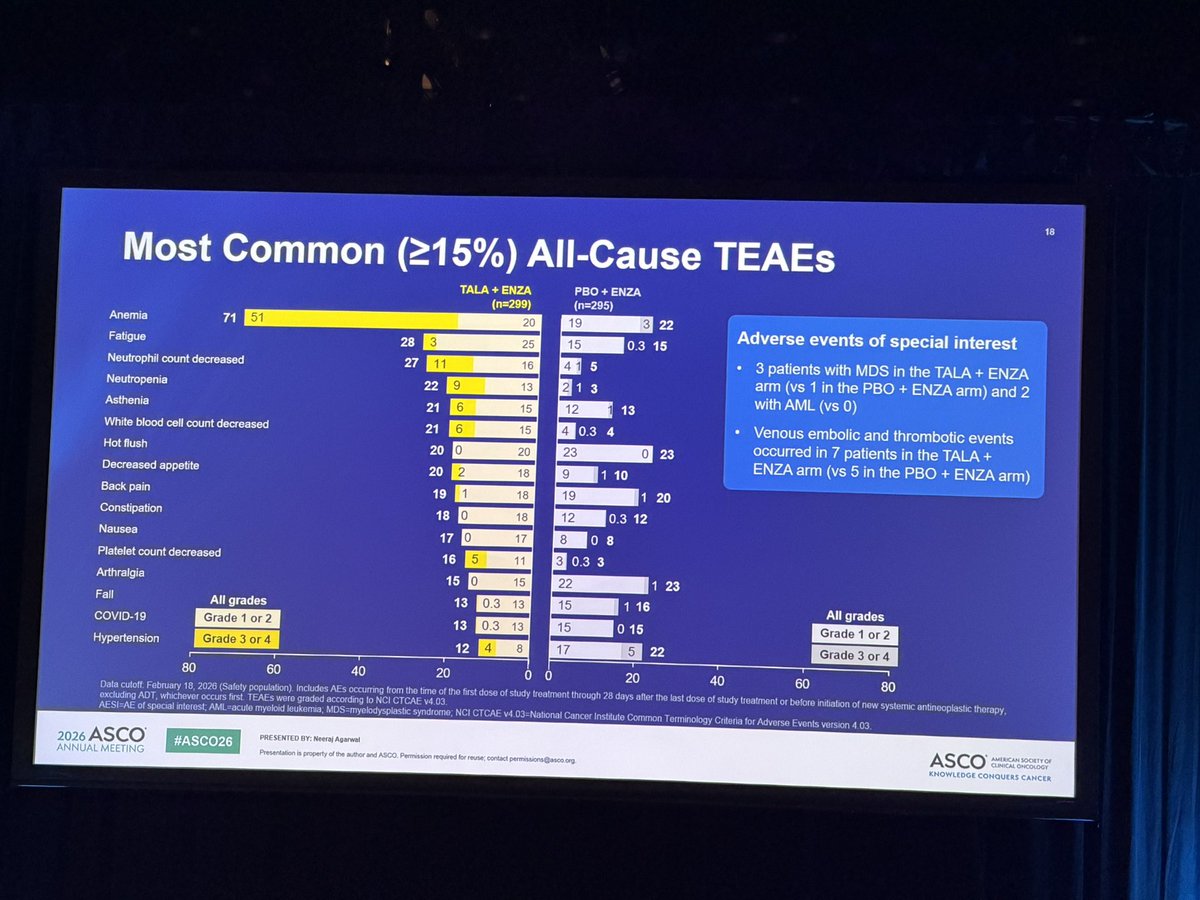
TALAPRO-3: Trial Design
Primary endpoint
Key eligibility criteria
rPFS by investigator assessment
HRR gene-altered mCSPC
Key secondary endpoint
Metastatic disease confirmed by positive
bone scan or metastatic lesion by CT or
TALA 0.5 mg*
ENZA 160 mg QD
OS (alpha-protected)
MRI scan
Other secondary endpoints
ECOG PS 0 or 1
ORR per RECIST v1.1
Ongoing ADT
Duration of soft tissue response
1:1
N=599
PSA response
<3 months of prior ADT with/without ARPI
for mCSPC
Time to PSA progression
Time to subsequent
Prior docetaxel for mCSPC not permitted
PBO + ENZA 160 mg QD
antineoplastic therapy
Stratification factors
Time to first SSE
De novo vs relapsed mCSPC
Safety
Data cutoff: February 18, 2026
PROs
High- vs ow-volume disease
Exploratory endpoint
BRCAm vs non-BRCAm
PFS2
HRRm: ATM, ATR, BRCA1, BRCA2, CDK12, CHEK2, FANCA, MLH1, MRE11A, NBN, PALB2, RAD51C
*0 mg CD the patient has побегия renal payment As per the DROSOCIA amendment Suptember 2021) CiricalTrass gov dentiller CT04925622 EAR lesting using and Foundation kguid
CDa) REARRERCA remputed omography EGOG Cospetative Osralogy Group performance states, gene allerations; Milimagretic resonance magna response cale, OS-overal
vavivit PT S2-teme to second programment or dealh PRO-paters reported ostcomo, PSA entigent, daily RECIST VI 1-Response valuation China 0. Solid Tumors version event
2026 ASCO
#ASCO26
- SENTED BY - Agenes
ASCO
I
ANNUAL MEETING
Preservation property whe - ASCO - voiced " - - -
KNOWLE 1004 CONDUERS CANCER
A-L
2026ASCO
ANNUAL MEETING
ASCO
ASCO
ASCO
ASCO
AS
SCO
AS
Key Takeaways
2
TALAPRO-3 met its primary endpoint: Treatment with talazoparib plus
enzalutamide (TALA + ENZA) prolonged rPFS (HR, 0.48) VS the ENZA
control arm in mCSPC with HRR gene alterations
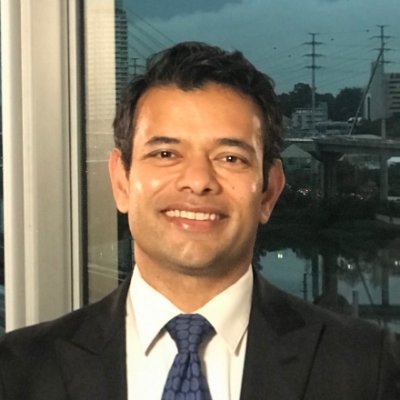
The most common adverse events observed were hematologic (anemia,
decreased neutrophil count) and fatigue
These results support the use of TALA + ENZA as a potential treatment
option for patients with HRR gene-altered mCSPC
PRE SENTED BY: Neeraj Agarwal
ASCO
AMERICAN
CLINICAL OMCOLOGY
2026 ASCO
#ASCO26
KNOWLEDGE CONQUERS CANCE
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco org
18
Most Common (≥15%) All-Cause TEAEs
TALA ENZA
PBO + ENZA
(n=299)
(n=295)
Anemia
71
51
20
19
3
22
Adverse events of special interest
Fatigue
28
3
25
15
0.3 15
Neutrophil count decreased
27
11
16
4
5
3 patients with MDS in the TALA + ENZA
Neutropenia
22
9
13
2
3
arm (vs 1 in the PBO + ENZA arm) and 2
with AML (vs 0)
Asthenia
21
6
15
12
13
White blood cell count decreased
21
6
15
4
0.3 4
Venous embolic and thrombotic events
Hot flush
20
0
20
23
0
23
occurred in 7 patients in the TALA +
ENZA arm (vs 5 in the PBO + ENZA arm)
Decreased appetite
20
2
18
9
1 10
Back pain
19
1
18
19
1 20
Constipation
18
0
18
12
0.3 12
Nausea
17
0
17
8
0 8
Platelet count decreased
16
5
11
3033
Arthralgia
15
0
15
22
1 23
Fall
All grades
13
0.3 13
15
1 16
All grades
COVID-19
Grade 1 or 2
13 0.3 13
15
0 15
Grade 1 or 2
Hypertension
Grade 3 or 4
12
4
8
17
5
22
Grade 3 or 4
80
60
40
20
0
0
20
40
60
80
Data cutoff. February 18, 2026 (Safety population). Includes AEs occurring from the time of the first dose of study treatment through 28 days after the last dose of study treatment or before initiation of new systemic antineoplastic therapy,
excluding ADT, whichever occurs first. TEAEs were graded according to NCI CTCAE v4.03.
AESI=AE of special interest; AML acute myeloid leukemia; MDS=myelodysplastic syndrome; NCI CTCAE v4. 03=National Cancer Institute Common Terminology Criteria for Adverse Events version 4.03.
2026 ASCO
PRESENTED BY: Neeraj Agarwal
ASCO
AMERICAN SOCIETY OF
#ASCO26
CLINICAL CHCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
TALAPRO-3: Trial Design
Primary endpoint
Key eligibility criteria
rPFS by investigator assessment
HRR gene-altered mCSPC
Key secondary endpoint
Metastatic disease confirmed by positive
OS (alpha-protected)
bone scan or metastatic lesion by CT or
TALA 0.5 mg*
ENZA 160 mg QD
Other secondary endpoints
MRI scan
ORR per RECIST v1.1
ECOG PS 0 or 1
Duration of soft tissue response
Ongoing ADT
1:1
N=599
PSA response
33 months of prior ADT with/without ARPI
Time to PSA progression
for mCSPC
Time to subsequent
Prior docetaxel for mCSPC not permitted
PBO
+ ENZA 160 mg QD
antineoplastic therapy
Time to first SSE
Stratification factors
Safety
De novo vs relapsed mCSPC
Data cutoff: February 18, 2026
PROs
High- vs low-volume disease
Exploratory endpoint
BRCAm vs non-BRCAm
PFS2
HRRm ATM, ATR. BRCA1, BRCA2, CDK12, CHEK2, FANCA, MLH1, MRE11A, NBN, PALB2, RAD51C
CEME 5.B. 1 - - - - bes - - shopsery - 1000 per the - - environment Compensive / Oberagy 2021) Group - NC104821022 - - - Foundations and - real
performance
I
- n - X - - CO- dary REGIST as - - - has - majing, - 11 SSE - - - - -
I
magning
|
/
2026 ASCO
#ASCO26
- BURDED " - -
ANNUAL MILLERING
Personal
-
ASCO
-
I
CARRIER
Friday, May 29
2:15-5:45PM - GU Oral Abstracts - RCC +
Bladder
-A phase 2 randomized trial of radium-223
dichloride and cabozantinib in patients (pts) with
renal cell carcinoma (RCC) with bone metastases
(BM) - dr. Rana McKay
-A prospective, multi-center, phase 1b/II 1L
cadonilimab + axitinib in non-clear-cell RCC - Dr. Xu
Hu
-ctDNA analysis in KN-564 - Dr. Toni Choueiri
-Is the Best Yet to Come in Kidney Cancer? Dr.
Martin Voss
-Intravesical recombinant BCG combined with
chemo-immunotherapy (chemo-IO) as perioperative
therapy for patients with MIBC - Dr. Richard
Cathomas
-HRQOL in AMBASSADOR MIBC - Dr. Ronald
Chen
-Curing Early Bladder Cancer with MultiD
Approaches - Dr. Melissa Reimers
-Perioperative SHR-A2102, a novel
nectin-4-targeted antibody-drug conjugate, in
combination with adebrelimab for patients (pts) in
MIBC - Dr. Yijun Shen
-3.5 year f/u for EV-302 - Dr. Tom Powles
-Initial results from NEXUS01 ph1 LY4052031 ADC
targeting Nectin-4 - Dr. Gopa lyer
-Nectin-4 ADCs: Past, Present, Future - Dr. Andrea
Apolo
TALAPRO-3 (NCT04821622) is a Phase 3, randomised, double-blind, placebo-controlled trial of talazoparib + enzalutamide + ADT versus placebo + enzalutamide + ADT in patients with first-line metastatic castration-sensitive prostate cancer (mCSPC / mHSPC) harboring homologous recombination repair (HRR) gene alterations. The trial enrolled 599 patients globally and tested whether moving the PARP inhibitor + AR-pathway inhibitor combination — already approved in mCRPC via TALAPRO-2 — into an earlier line of therapy can extend radiographic progression-free survival in a biomarker-selected population.
The trial is being discussed by KOLs as the first prospective Phase 3 demonstration that an HRR-selected PARPi + ARPI intensification strategy improves rPFS in the castration-sensitive setting. The headline numbers are large — an rPFS hazard ratio of 0.48 and a 3-year rPFS of 76.6% vs 56% — but KOLs are also flagging the cost: a 19% talazoparib discontinuation rate, two treatment-related deaths in the talazoparib arm versus zero on placebo, and an overall survival curve that is trending in favor of the experimental arm but has not yet reached statistical significance (3-yr OS 77.8% vs 71.6%, HR 0.767, P=0.0905). The clinical debate now centers on patient selection within the HRR-altered subgroup — how much additional benefit is enough to justify the added toxicity, particularly outside of BRCA-altered disease.
Global PI Neeraj Agarwal (Huntsman Cancer Institute, University of Utah) presented at the ASCO 2026 Bladder/Genitourinary oral session (May 30 2026, Abstract LBA5007), with simultaneous publication in NEJM. The trial sits alongside earlier mCRPC programs — TALAPRO-2 (the registrational mCRPC study for the same combination), PROpel (olaparib + abiraterone), and MAGNITUDE (niraparib + abiraterone) — and now extends the PARPi + ARPI question into the upfront, hormone-sensitive setting.
Phase 3, multicenter, randomised, double-blind, placebo-controlled trial (NCT04821622). Patients with HRR-altered 1L mCSPC randomised 1:1 to talazoparib 0.5 mg/day (or 0.35 mg/day for renal impairment) + enzalutamide 160 mg/day + ADT versus placebo + enzalutamide 160 mg/day + ADT. Stratification by high-volume vs low-volume disease and BRCA vs non-BRCA HRR alteration.
Population
N=599 patients with metastatic castration-sensitive prostate cancer and at least one HRR gene alteration per the HRR12 panel (ATM, ATR, BRCA1, BRCA2, CDK12, CHEK2, FANCA, MLH1, MRE11A, NBN, PALB2, RAD51C). Eligibility required ≤3 months of ADT before randomisation and no brain metastases. Enrolment spanned US, Canada, Europe, South America, and Asia-Pacific sites.
Drug Regimen
TALZENNA (talazoparib) + XTANDI (enzalutamide) + ADT. Pfizer is the talazoparib sponsor; enzalutamide is co-developed by Pfizer and Astellas. The combination is already FDA-approved in mCRPC (via TALAPRO-2, 2023). TALAPRO-3 is the first prospective Phase 3 test of the same regimen earlier in the disease course.
Endpoints
Primary: radiographic progression-free survival (rPFS) by blinded independent central review. Key secondary: overall survival, time to PSA progression, time to cytotoxic chemotherapy, objective response rate, safety, and patient-reported outcomes (EORTC QLQ-C30).
Primary Endpoint — rPFS Met (HR 0.481 (95% CI 0.357-0.647); median NOT reached)
Talazoparib + enzalutamide + ADT delivered an rPFS hazard ratio of 0.48 versus placebo + enzalutamide + ADT, with the median rPFS not reached at >3 years of follow-up. The 3-year rPFS was 76.6% (TALA + ENZA) vs 56% (placebo + ENZA), a ~20-point absolute improvement at the 3-year landmark. Benefit was reported as consistent across pre-specified subgroups, including both BRCA-altered and non-BRCA HRR populations.
rPFS met · median not reached · consistent across BRCA and non-BRCA HRR subgroups
Secondary — Time to PSA Progression Strongly in Favor of TALA
At 3 years, 78.3% of TALA + ENZA patients were free of PSA progression versus 62.7% on placebo + ENZA, hazard ratio 0.513, P<0.0001. This is the cleanest secondary signal supporting the rPFS result and reinforces that the experimental combination is delaying biochemical progression as well as radiographic progression.
Overall Survival — Trending, NOT Statistically Significant
3-year OS was 77.8% on TALA + ENZA versus 71.6% on placebo + ENZA, hazard ratio 0.767 (95% CI 0.564–1.044), P=0.0905. The OS curve is trending in favor of the experimental arm but has not crossed the threshold for statistical significance at this readout, and OS data remain immature. Multiple KOLs flagged the immature OS as the key open question driving how widely the regimen will be adopted in mCSPC.
The TALAPRO-3 safety profile is the focal point of the KOL nuance. The most clinically significant toxicity is hematologic: Grade ≥3 anemia in 51% of talazoparib-arm patients, with 40% requiring transfusions. Permanent discontinuation of talazoparib occurred in 19% of patients; 5% discontinued specifically because of anemia. There were 2 treatment-related deaths in the talazoparib arm and 0 in the placebo arm. Patient-reported outcomes on the EORTC QLQ-C30 "generally did not show clinically meaningful differences between the two arms, except for appetite loss." This is the toxicity envelope that KOLs (Yüksel Ürün, Suyog Cancer, and others) are weighing against the rPFS benefit when discussing which HRR-altered patients should receive upfront PARP intensification — particularly outside of BRCA-altered disease, where the rPFS benefit is smaller (HR 0.57) and the hematologic cost is the same. Sources: Agarwal ASCO 2026 oral · OncoDaily TALAPRO-3 coverage · Fierce Pharma May 30 2026 · KOL slide OCR.
Endpoint values verbatim from Neeraj Agarwal's ASCO 2026 oral presentation (LBA5007, May 30 2026) as captured by attending KOLs (@shilpaonc, @DrChoueiri, @tompowles1, @DrYukselUrun) and reconciled with simultaneous NEJM publication and the Pfizer / Astellas joint press release. See OncoDaily TALAPRO-3 detail and Pfizer press release.
Frequently Asked Questions
TALAPRO-3 FAQ
What is the TALAPRO-3 trial?
TALAPRO-3 is a Phase 3, randomized, double-blind, placebo-controlled trial (NCT04821622) of talazoparib (Talzenna) + enzalutamide (Xtandi) + androgen deprivation therapy (ADT) versus placebo + enzalutamide + ADT in 599 patients with first-line metastatic castration-sensitive prostate cancer (mCSPC) harboring homologous recombination repair (HRR) gene alterations.
Is talazoparib + enzalutamide FDA approved for first-line mCSPC?
No. The first-line metastatic castration-sensitive prostate cancer (mCSPC) indication studied in TALAPRO-3 is investigational and not FDA approved. Talazoparib (Talzenna) plus enzalutamide (Xtandi) is FDA approved only for HRR gene-mutated metastatic castration-resistant prostate cancer (mCRPC), based on the separate TALAPRO-2 trial.
Did TALAPRO-3 meet its primary endpoint?
Yes. TALAPRO-3 met its primary endpoint of radiographic progression-free survival: the combination delivered an rPFS hazard ratio of 0.481 (95% CI 0.357-0.647) versus placebo plus enzalutamide plus ADT, with median rPFS not reached and a 3-year rPFS of 76.6%.
What did TALAPRO-3 show for overall survival?
Overall survival is trending in favor of the combination but is not statistically significant: 3-year OS was 77.8% with talazoparib + enzalutamide versus 71.6% with placebo + enzalutamide (HR 0.767; 95% CI 0.564-1.044; p=0.0905). Longer follow-up is needed.
Who develops talazoparib and enzalutamide?
Talazoparib (Talzenna), a PARP inhibitor, is developed by Pfizer. Enzalutamide (Xtandi), an androgen-receptor pathway inhibitor, is co-developed by Astellas Pharma and Pfizer.
Major Media & Publications
TALAPRO-3 in the News
Competitive Context — PARPi + ARPI Battle in 1L mCSPC
Pfizer's TALAPRO-3 vs J&J's AMPLITUDE (niraparib + abi / Akeega): the two head-to-head Phase 3 reads in HRR-altered 1L mCSPC tell very different stories outside of BRCA.
BRCA2: 54% rPFS improvement (driver of overall benefit per FDA exploratory analysis)
Non-BRCA: only 12% better than control
FDA approval: narrow label restricted to BRCA2
Fierce Pharma (May 30 2026): “Pfizer appears to have one-upped Johnson & Johnson again in their PARP inhibitor battle in prostate cancer… Talzenna and Xtandi showed a robust 43% radiographic PFS improvement in the non-BRCA-mutated group, compared with 63% among BRCA-mutated patients.”
Primary publications, sponsor & institutional press releases, and major oncology media coverage around the Agarwal/Huntsman ASCO 2026 late-breaking oral presentation.
Huntsman Cancer Institute, University of Utah · TALAPRO-3 Global PI
“These data are unprecedented in their depth and have the potential to change clinical practice for first-line metastatic castration-sensitive prostate cancer with HRR alterations. TALAPRO-3 demonstrates that combining a PARP inhibitor with enzalutamide and ADT can meaningfully delay disease progression in this earlier-line setting.”
All 40 curated TALAPRO-3 tweets from #ASCO26 and pre-conference commentary — sorted positive → neutral → cautious. Text is verbatim from each KOL (leading reply-to @mentions and trailing media URLs trimmed for readability). Distribution: 4 positive · 29 neutral · 7 cautious.
























 ↗
↗
 ↗
↗
 ↗
↗