I-SPY 2.2 (NCT01042379) is the latest evolution of the I-SPY 2 adaptive neoadjuvant platform trial for high-risk, stage 2-3 early breast cancer. It uses a SMART sequential-randomization, MRI- and residual-cancer-burden-guided Block A/B/C design that enables both treatment de-escalation and escalation. Its first major readouts are the investigational datopotamab deruxtecan (Dato-DXd) plus-or-minus durvalumab arms (Nature Medicine 2024). Sponsor: Quantum Leap Healthcare Collaborative.
Discover KOL Sentiment on I-SPY 2.2 →Design — Phase 2 adaptive neoadjuvant platform (I-SPY 2 TRIAL, since 2010); SMART sequential-randomization Blocks A->B->C with MRI/pre-RCB-guided de-escalation and escalation; MammaPrint/receptor-subtype stratified, high-risk stage 2-3 early breast cancer (NCT01042379). (Nature Medicine 2024)
Primary endpoint — Pathological complete response / low residual cancer burden (RCB), used as an early adaptive readout. (platform design)
First readouts — Datopotamab deruxtecan (Dato-DXd) plus-or-minus durvalumab arms — the first major I-SPY 2.2 results (Nature Medicine 2024; Shatsky et al. for Dato-DXd + durvalumab, Khoury et al. for Dato-DXd alone). (Nature Medicine 2024)
Survival — Overall survival and event-free survival are not yet mature for the I-SPY 2.2 arms; the pCR-to-EFS relationship underpins the platform's design. (platform design)
Platform track record — I-SPY has tested 22 agents since 2010, with 12 completed and 7 graduated in at least one subtype; the 'seamless Phase 2/3' framework was developed with the FDA. (platform design)
Regulatory / Sponsor — INVESTIGATIONAL — I-SPY 2.2 neoadjuvant arms are not FDA approved in this setting. Quantum Leap Healthcare Collaborative with an academic consortium (UCSF, U. Penn, MD Anderson, others; NCI-funded). (FDA / trial design)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.








Top tweets by impressions — click to view on X
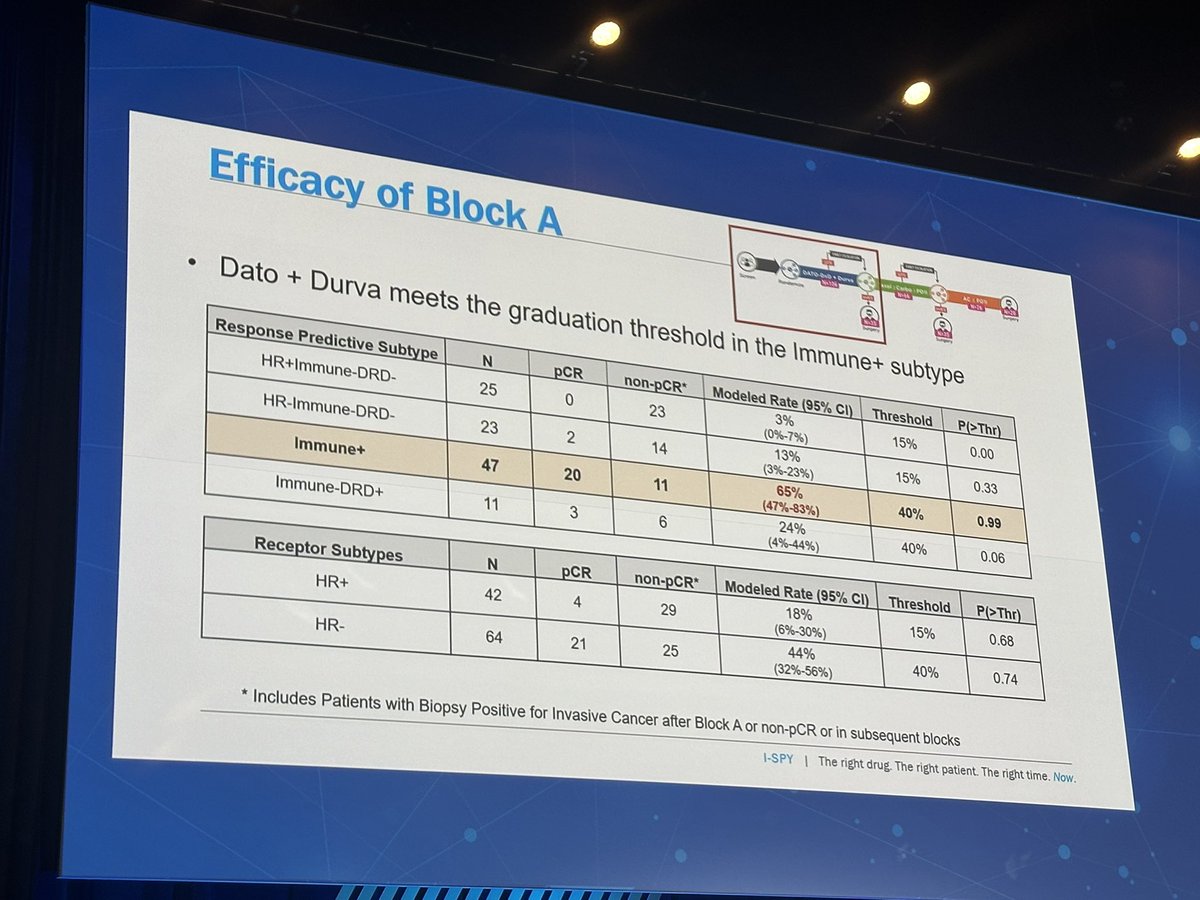
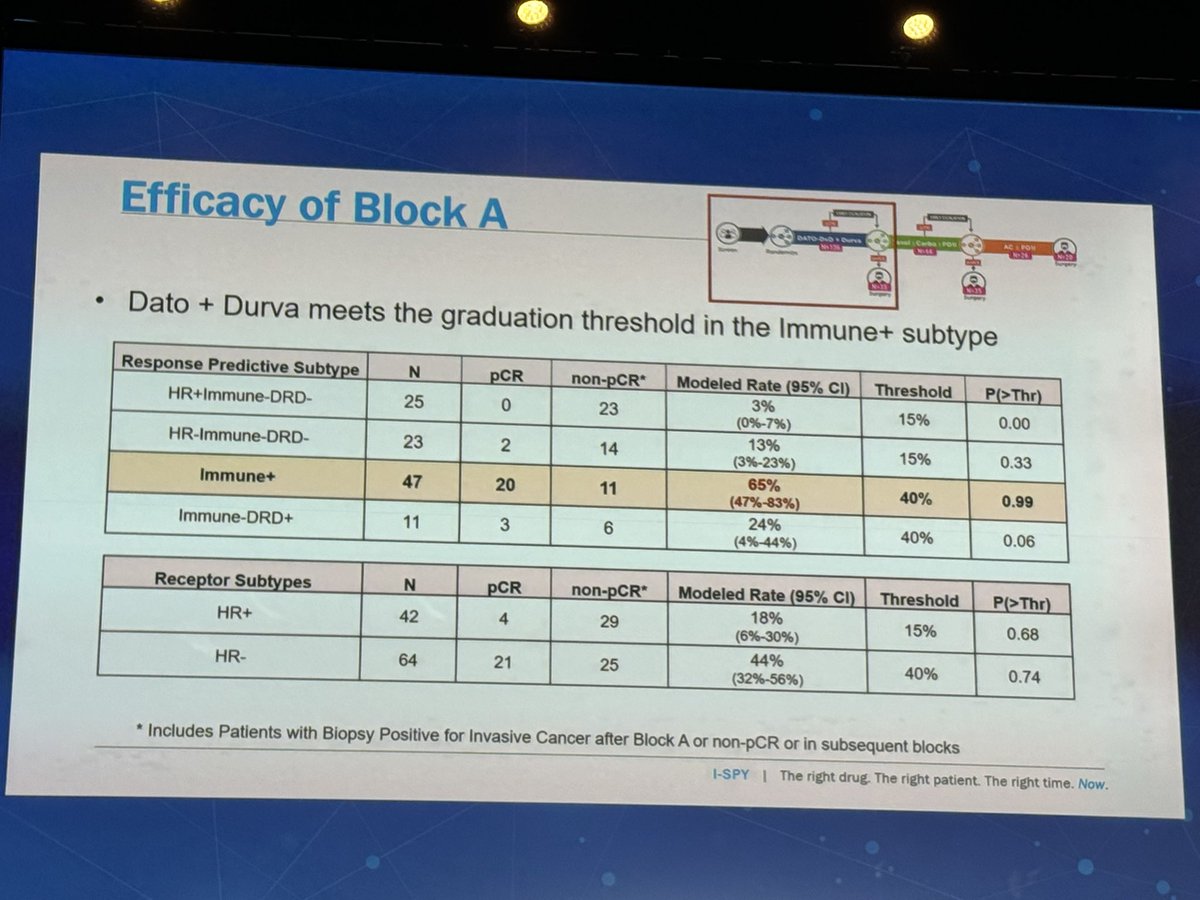
ISPY2.2 Dato-DXd + durvalumab beautifully presented by @Dr_RShatsky. After 4 cycles neoadj Dato/durva, 4/42 pts w/ HR+ and 21/64 pts w/ HR- stage II/III EBC achieved pCR. 43% pCR in immune+ subtype,…
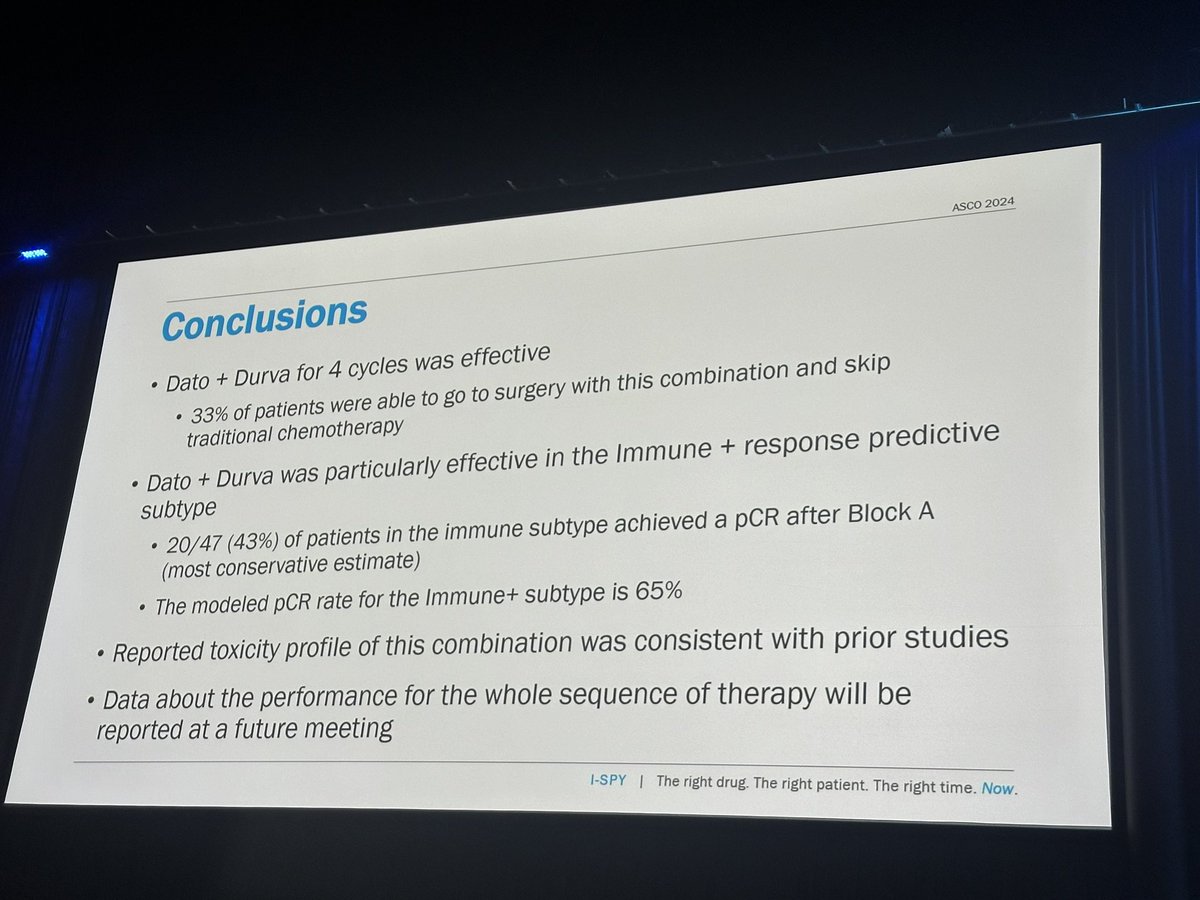
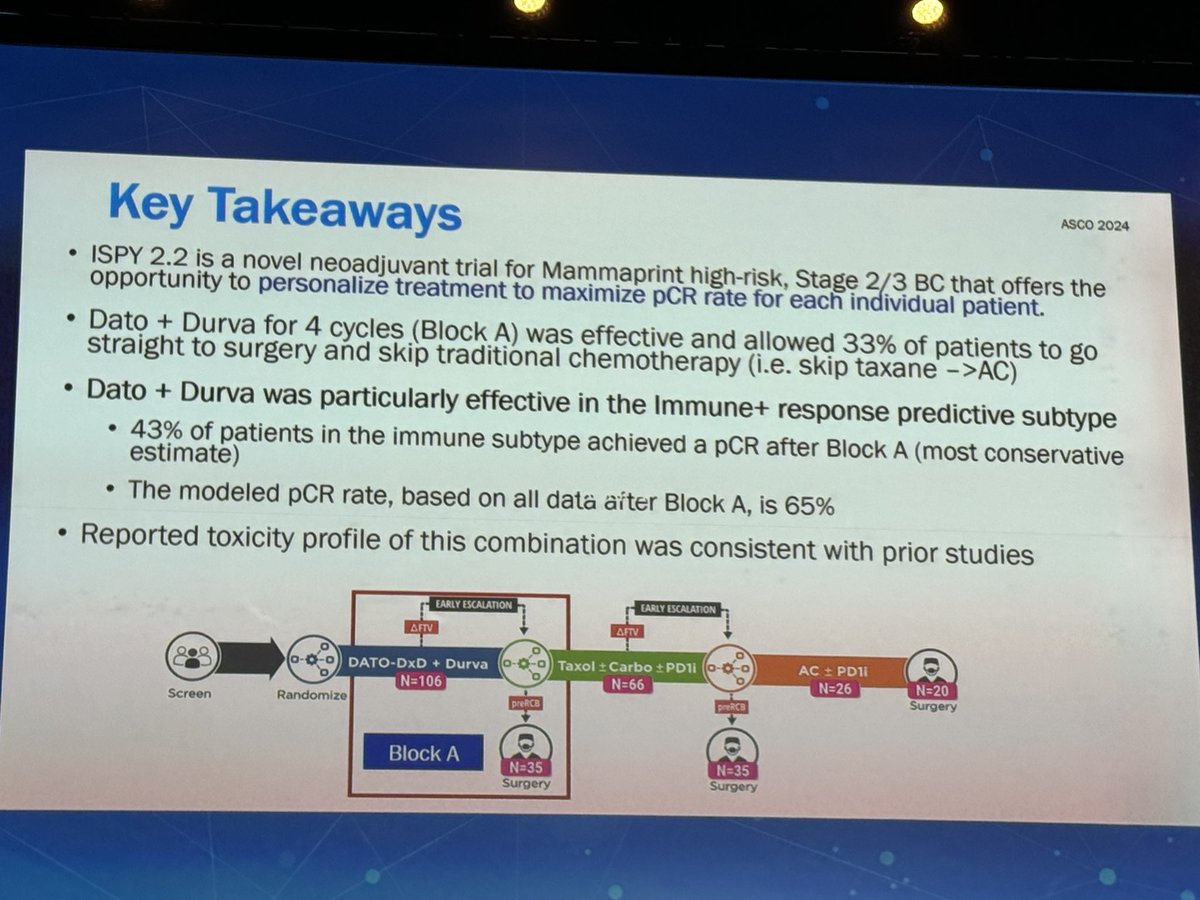
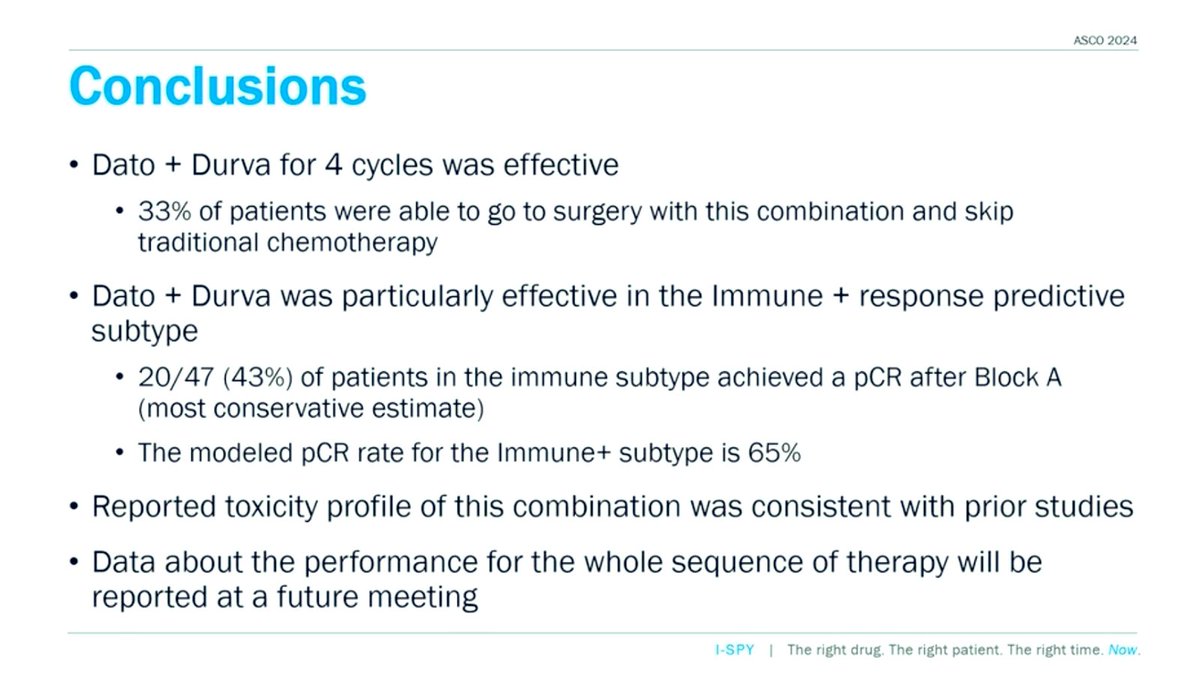
Data from ISPY2.2 demonstrated 32% of pts were able to skip chemo and go to surgery after 4 cycles of Dato-DXd, but did not meet the threshold to graduate
@jane_meisel #ASCO24 @OncoAlert #bcsm
@Dr_RShatsky presents dato+ durva in ISPY2.2
After just 4 cycles of combo, 1/3 pts able to go straight to surgery and spare more chemo
Immune + subtype had a 43% pCR rate (modeled to be…
📌Rates of pathologic complete response (pCR) after datopotamab deruxtecan (Dato) plus durvalumab (Durva) in the neoadjuvant setting: Results from the I-SPY2.2 trial‼️presented by @Dr_RShatsky…
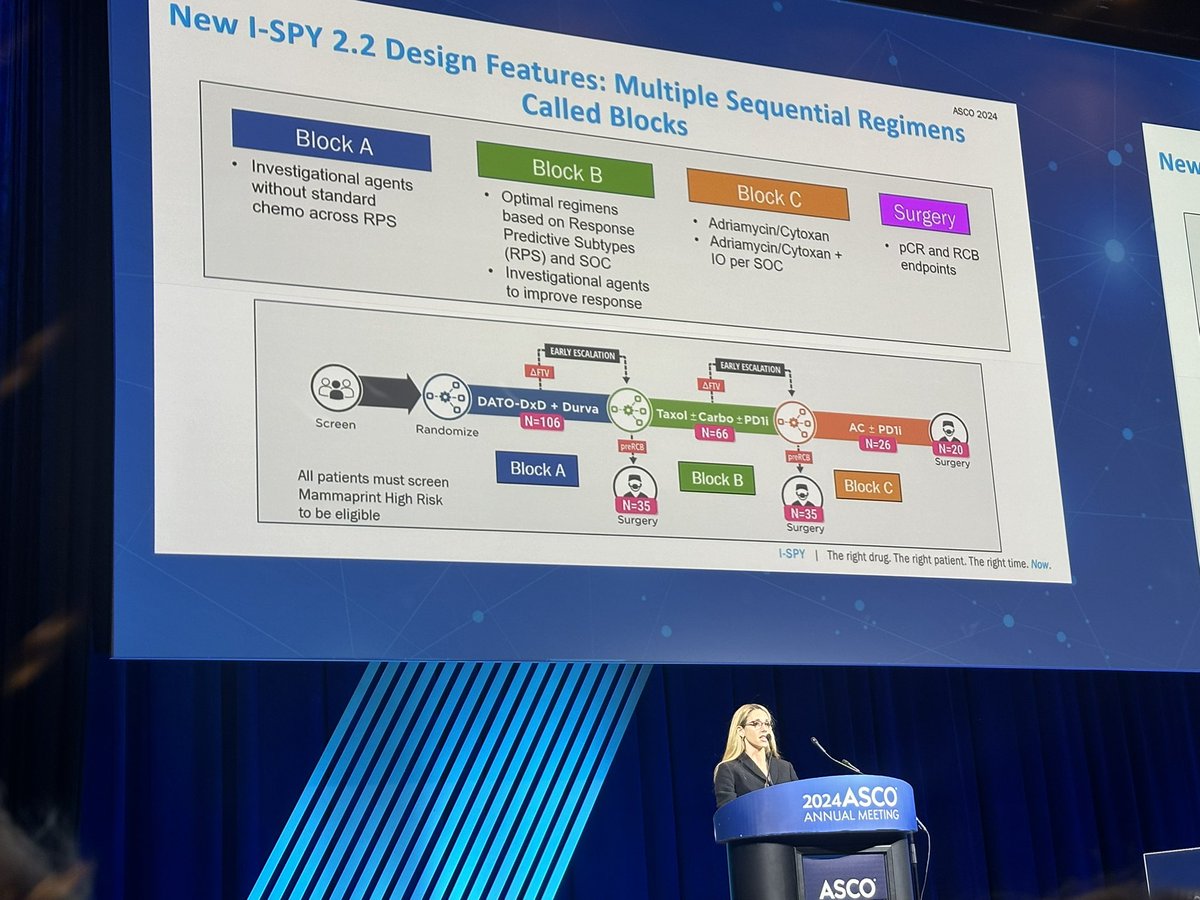
ISPY2.2: Preop Dato-DXd + durva, n=106 (n=35, or 33% went to surgery after 4 cycles)
43% of pts in immune subtype achieved pCR
HR+ :Modeled pCR rate 18%
TNBC: Modeleled pCR 44%
39.6% HR+ (4/42…
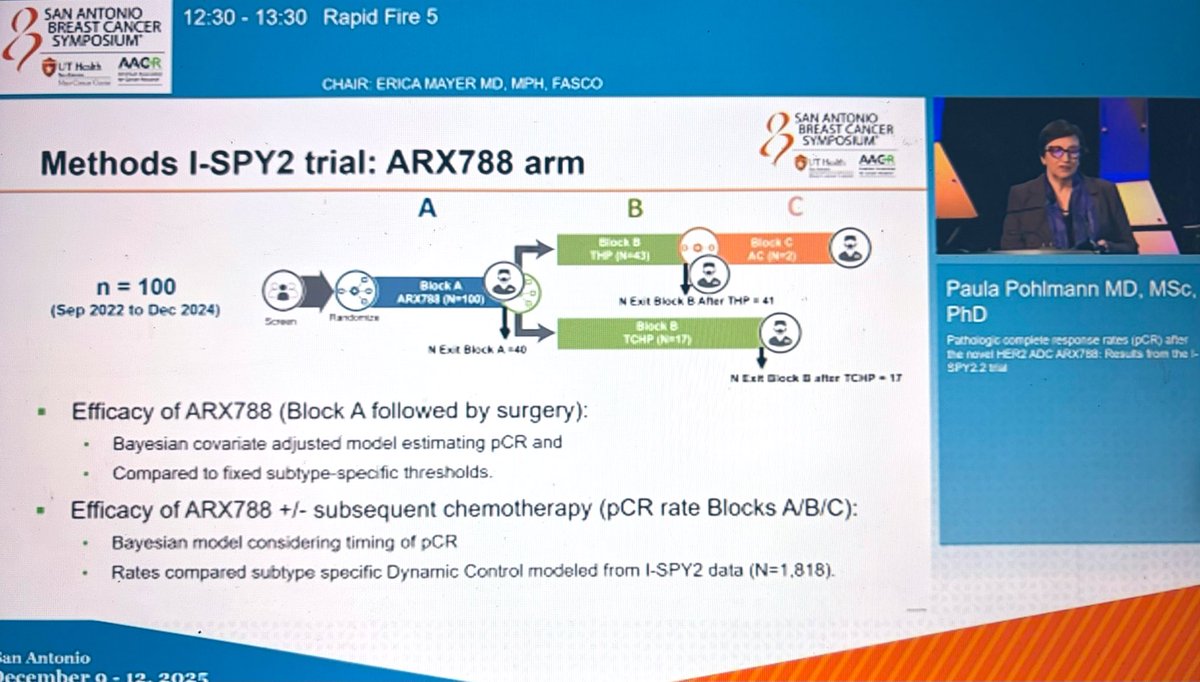
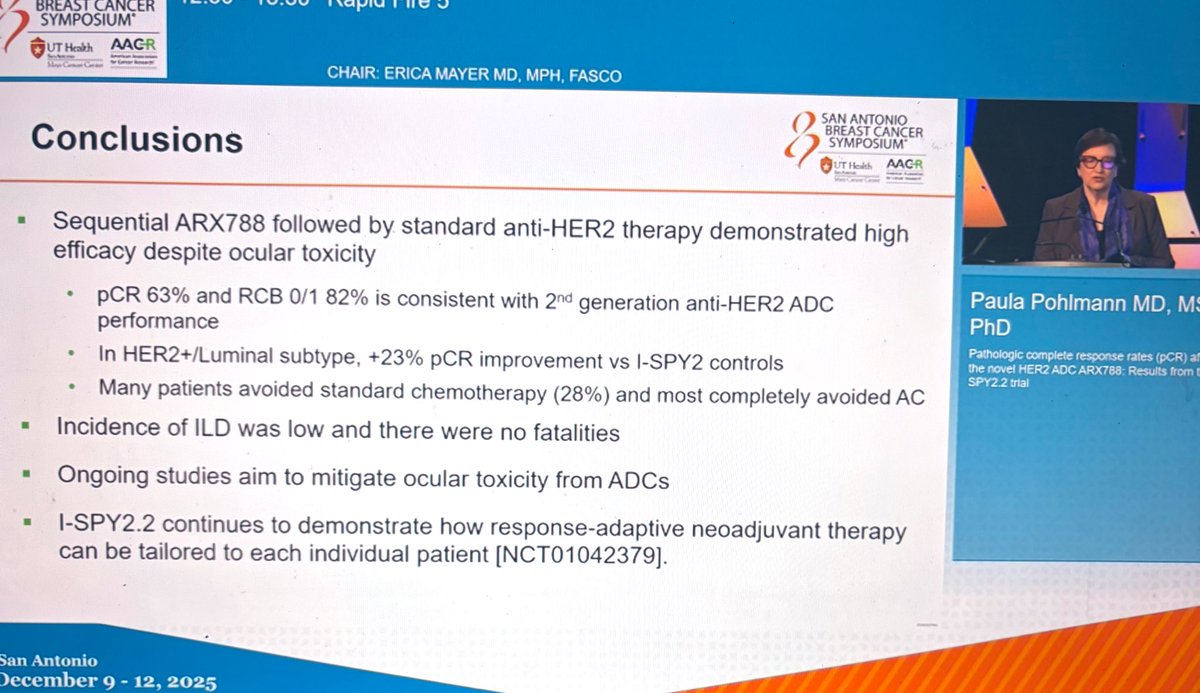
ISPY2.2 trial: pCR after preop ARX788 followed by stnd anti-HER2 therapy
(70% HR+ HER2+)
pCR: 63%
RCB 0/1: 82%
No RCB 3s
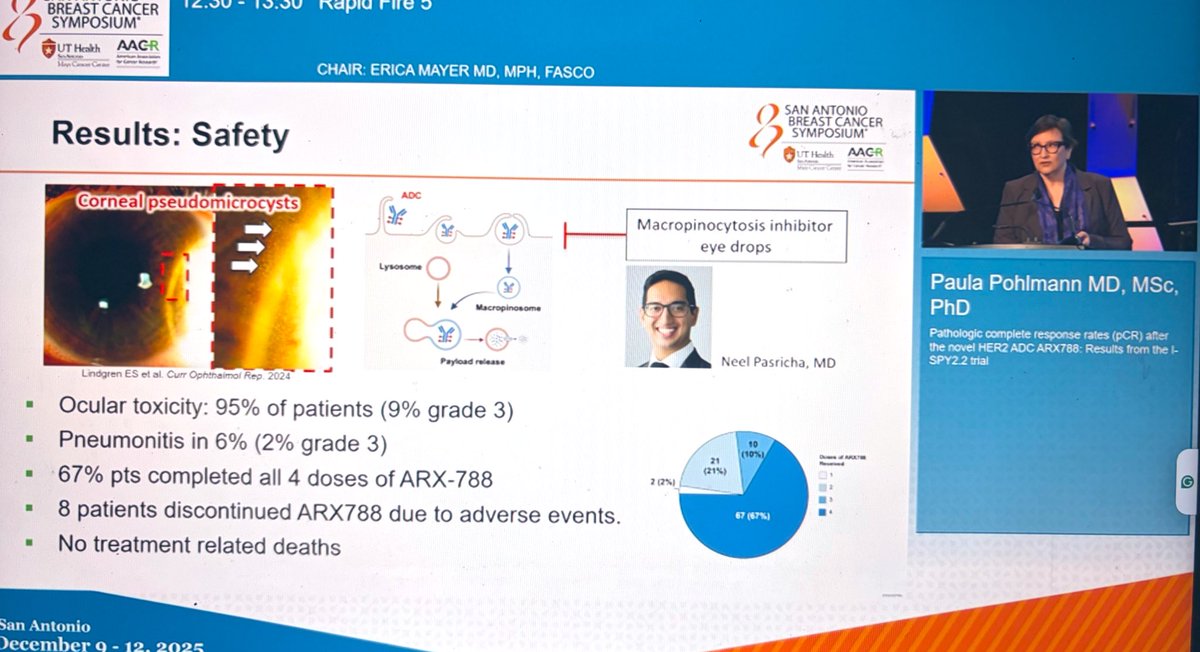
Safety: 95% ocular tox, 6% pneumonitis
67% completed all 4 doses of…
#ISPY2 D-Dxd buddies!! The incredible @jane_meisel who did an phenomenal job presenting Dato alone data on Friday! She set a pretty high bar! So lucky to call her a friend! ❤️#ASCO24 #bcsm…
📌 RF5-06 Pathologic complete response rates (pCR) after the novel HER2 ADC ARX788:
Results from the I-SPY2.2 trial✨
Presented by Paula Pohlmann
@OncoAlert #OncoAlertAF #SABCS25…
Congratulations, @Dr_RShatsky at #ASCO24! Thank you for sharing your knowledge on optimizing neoadjuvant strategies in breast cancer during this morning’s education session, and exciting updates on…

Learn about the I-SPY2.2 trial for neoadjuvant breast cancer treatment in this video with @Dr_RShatsky of @UCSDHealth from #ASCO24.
https://t.co/FY7KT5qEai
I-SPY 2.2 is the latest evolution of the I-SPY platform (running since 2010; 22 agents tested, 12 completed, 7 graduated in ≥1 subtype). The SMART sequential-randomization design and MRI-based pre-RCB strategy enable BOTH de-escalation (skip AC for predicted CR) AND escalation (add Block B/C for non-responders). Extends original I-SPY 2 with a "seamless Phase 2/3" regulatory framework designed with FDA. Dato-DXd ± durvalumab arms (Nature Medicine 2024) are the first major readouts. Broader implications for accelerated drug development paradigms, validated by adoption in other cancers.
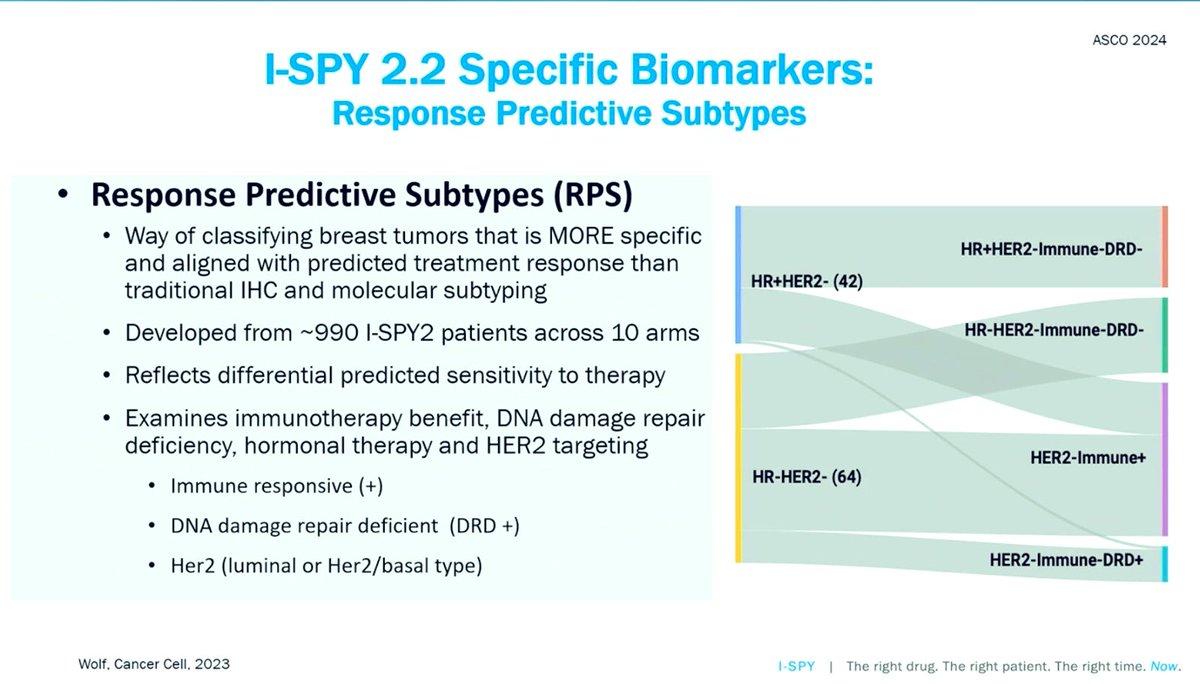
I-SPY 2.2 is a Phase 2 adaptive platform trial using a Sequential Multiple Assignment Randomized Trial (SMART) design with Blocks A → B → C. Block A: up to 4 novel experimental therapies without standard paclitaxel; patients predicted to have complete response (pre-RCB 0/1 by MRI + biopsy) proceed directly to surgery (de-escalation), while poor-responders proceed to Block B. Block B: subtype-specific best-in-class regimens. Block C: rescue with anthracycline chemotherapy (AC). Biomarker subtypes defined by HR/HER2/MammaPrint (70-gene signature). Specific pCR rates per arm/subtype not fully summarized in available sources; individual arm publications in Nature Medicine 2024 (Dato-DXd ± durvalumab). Prognostic pCR ↔ EFS/DRFS relationship validated from original I-SPY 2.
OS/EFS not yet mature for I-SPY 2.2 arms (recent trial evolution). Prognostic relationship between pCR and event-free survival / distant recurrence-free survival is a foundational assumption of the platform design.
Grade ≥3 TRAE rates are arm-specific and reported in individual Nature Medicine publications (Shatsky et al. for Dato-DXd + durva; Khoury et al. for Dato-DXd alone). Overall safety framework: adaptive de-escalation aims to reduce toxicity by allowing patients with imaging-confirmed complete response to skip further treatment blocks including anthracyclines.
🔬 Paradigm-shifting adaptive platform for accelerated neoadjuvant breast cancer drug development. I-SPY 2.2 is the latest evolution of the I-SPY platform (running since 2010; 22 agents tested, 12 completed, 7 graduated in ≥1 subtype). The SMART sequential-randomization design and MRI-based pre-RCB strategy enable BOTH de-escalation (skip AC for predicted CR) AND escalation (add Block B/C for non-responders). Extends original I-SPY 2 with a "seamless Phase 2/3" regulatory framework designed with FDA. Dato-DXd ± durvalumab arms (Nature Medicine 2024) are the first major readouts. Broader implications for accelerated drug development paradigms, validated by adoption in other cancers.
I-SPY 2.2 (NCT01042379) is the latest evolution of the I-SPY 2 adaptive neoadjuvant platform trial, which has evaluated novel regimens for high-risk, stage 2-3 early breast cancer since 2010. It stratifies patients by MammaPrint and receptor subtype and uses a Sequential Multiple Assignment Randomized Trial (SMART) design. It is sponsored by Quantum Leap Healthcare Collaborative with an academic consortium.
I-SPY 2.2 introduces a SMART sequential-randomization design with Blocks A, B and C and an MRI-based pre-residual-cancer-burden strategy. This lets the trial both de-escalate therapy (for example, omitting anthracycline chemotherapy for predicted responders) and escalate it (adding subsequent blocks for non-responders), individualizing neoadjuvant treatment within a 'seamless Phase 2/3' framework developed with the FDA.
The first major I-SPY 2.2 readouts were the datopotamab deruxtecan (Dato-DXd) arms, with and without durvalumab, published in Nature Medicine in 2024. These reported pathological complete response and residual-cancer-burden outcomes by subtype; overall survival and event-free survival for these arms are not yet mature.
No. I-SPY 2.2 is a platform trial that evaluates investigational neoadjuvant regimens, which are not FDA approved in the neoadjuvant early-breast-cancer setting. Some agents are separately FDA approved in other settings (for example, datopotamab deruxtecan is approved for certain metastatic breast cancer), but their use within I-SPY 2.2 is investigational.
I-SPY 2.2 is viewed as a paradigm-shifting platform for accelerating neoadjuvant breast cancer drug development. Its adaptive, biomarker-guided design lets multiple agents be tested efficiently, supports both de-escalation and escalation of therapy, and has influenced adaptive-trial approaches adopted in other cancers.
