Giredestrant (oral SERD) + palbociclib vs letrozole + palbociclib in 1L ER+/HER2- advanced breast cancer — Roche/Genentech
Discover KOL Sentiment on PERSEVERA →Read Roche Press Update →Design - Phase 3 giredestrant (oral SERD) + palbociclib vs letrozole + palbociclib, 1L ER+/HER2- advanced breast cancer (NCT04546009), N~992, 1:1; primary investigator-assessed PFS (ASCO 2026 LBA1006).
PFS (primary, NOT MET) - Median 33.1 vs 28.2 mo; HR ~0.89 - did not reach statistical significance; the primary endpoint was not met.
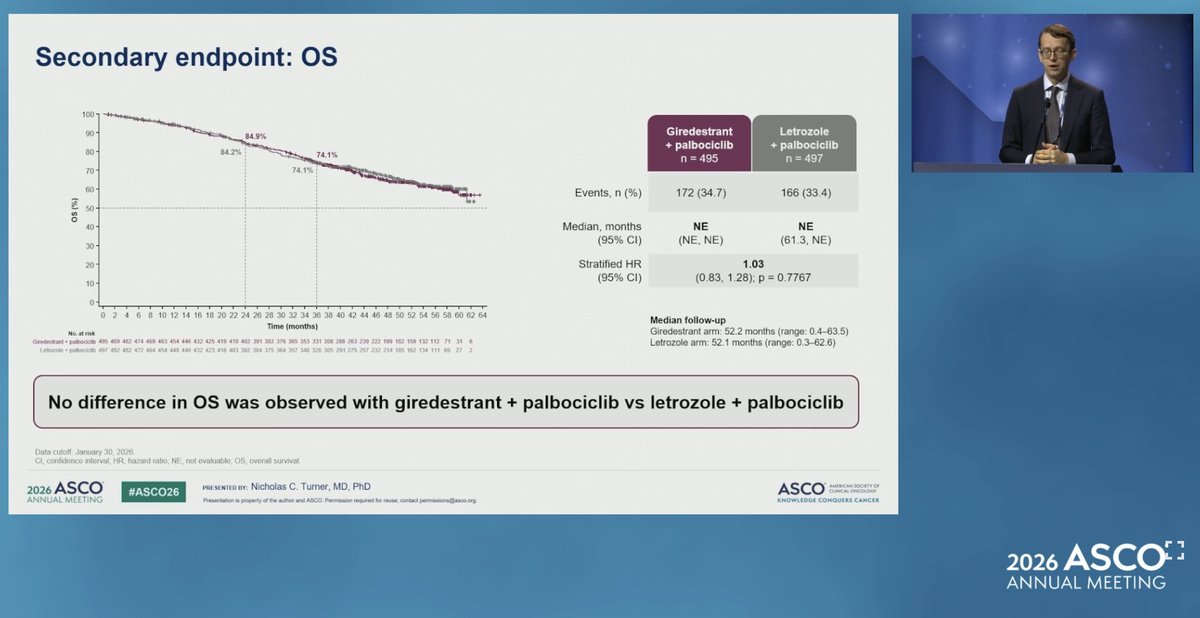
OS (secondary) - No difference at the Jan 30, 2026 cut - events 172/495 vs 166/497; median OS not estimable in both arms.
Response - Similar - ORR 60.2% vs 59.9%; clinical benefit rate 82.6% vs 82.1%; duration of response numerically longer with giredestrant (38.5 mo).
Regulatory - Investigational / negative - giredestrant not FDA approved; PERSEVERA did not establish oral SERD + CDK4/6i in the 1L setting.
Sponsor / drug - Roche/Genentech; giredestrant + palbociclib (Ibrance).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.






PERSEVERA (persevERA) is a randomized, double-blind, placebo-controlled Phase 3 trial evaluating giredestrant (oral SERD) + palbociclib vs letrozole + palbociclib in patients with 1L ER+/HER2-negative locally advanced or metastatic breast cancer. ~992 patients were randomized. The trial tested whether an oral selective estrogen receptor degrader (SERD) could replace aromatase inhibitors as the endocrine backbone alongside CDK4/6 inhibition in the front-line setting. Companion programs in the giredestrant development program — lidERA (early breast cancer), evERA (advanced post-endocrine resistance), and pionERA (post-CDK4/6 resistant) — remain ongoing.
ER+/HER2-negative locally advanced or metastatic breast cancer; no prior systemic therapy for advanced disease (frontline setting). Approximately 992 patients randomized 1:1.
Experimental: Giredestrant 30 mg PO once daily + Palbociclib 125 mg PO (Days 1–21 of a 28-day cycle).
Control: Letrozole 2.5 mg PO once daily + Palbociclib 125 mg PO (Days 1–21 of a 28-day cycle).
The primary investigator-assessed PFS (INV-PFS) endpoint was not met. Full data presented at ASCO 2026 (Abstract LBA1006, Nicholas C. Turner) showed median PFS of 33.1 months (95% CI 30.2–38.3) with giredestrant + palbociclib vs 28.2 months (95% CI 25.0–33.1) with letrozole + palbociclib — stratified HR 0.89 (95% CI 0.76–1.05), p = 0.1553. The pre-specified significance boundary (HR 0.85, 2-sided p < 0.0456) was not crossed: a numerical benefit only, with no demonstrated superiority over the letrozole + palbociclib standard. Median follow-up ~52 months; data cutoff January 30, 2026.
OS, a key secondary endpoint, showed no difference between arms at the January 30, 2026 data cutoff. Events: 172/495 (34.7%) with giredestrant + palbociclib vs 166/497 (33.4%) with letrozole + palbociclib. Median OS was not estimable (NE) in both arms (control 95% CI 61.3–NE). Stratified HR 1.03 (95% CI 0.83–1.28), p = 0.7767.
Tumor response was similar between arms: objective response rate (ORR) 60.2% with giredestrant + palbociclib vs 59.9% with letrozole + palbociclib; clinical benefit rate (CBR) 82.6% vs 82.1%. Duration of response (DoR) was numerically longer with giredestrant — median 38.5 months (95% CI 30.4–48.7) vs 30.4 months (95% CI 25.3–36.1) — but without statistical significance, consistent with the deeper ER suppression the oral SERD provides without translating into a PFS win.
Safety was consistent with the known profiles of giredestrant and palbociclib individually, with no unexpected findings. Any-grade adverse events occurred in 99.8% (giredestrant arm) vs 98.0% (letrozole arm); grade 3/4 AEs in 85.5% vs 80.8%; AEs leading to treatment discontinuation were low and similar (9.5% vs 8.3%). Neutropenia was the dominant AE in both arms (CDK4/6 class effect). The one distinctive signal was bradycardia, more frequent with giredestrant (11.7% vs 1.8%) — but the vast majority were grade 1 and asymptomatic, with no grade 3/4 events in either arm.
KOLs have proposed four mechanistic explanations for the negative readout, drawn from @ChandrakanthMv's published breakdown:
① Frontline disease is highly endocrine-sensitive. Aromatase inhibition + CDK4/6 already achieves strong ER pathway suppression in untreated mBC. Replacing the AI with an oral SERD offers limited incremental benefit in this setting.
② ESR1 mutations are uncommon upfront. ESR1 mutations — where oral SERDs typically show their advantage — emerge after AI exposure. Frontline populations therefore derive limited SERD-specific benefit.
③ CDK4/6 already blocks downstream signaling. Palbociclib suppresses ER-driven cell-cycle progression. Additional ER degradation may not significantly enhance disease control beyond what CDK4/6 inhibition already provides.
④ Strong comparator arm. Letrozole + palbociclib is a highly effective standard. Superiority against this backbone is difficult to demonstrate.
ASCO discussant Matthew P. Goetz, MD (Mayo Clinic) framed the central interpretation: in the frontline setting, palbociclib suppresses ER-driven cell-cycle progression so effectively that swapping the aromatase inhibitor for an oral SERD adds little incremental benefit — the CDK4/6 inhibitor "blunts" any advantage the SERD might otherwise show. He also raised an alternative hypothesis: that mechanisms driving CDK4/6 resistance are not addressed simply by exchanging a SERD for an AI. His proposed path forward is strategic deployment of oral SERDs — potentially as 1L monotherapy with timing matched to a patient's risk profile — rather than a blanket AI-for-SERD substitution on the CDK4/6 backbone.
⚠️ AI + CDK4/6 remains the standard first-line therapy in ER+/HER2- metastatic breast cancer. PERSEVERA suggests oral SERDs do not displace aromatase inhibitors in the 1L setting. The likely value proposition for oral SERDs remains after endocrine resistance or in ESR1-mutant disease — settings being tested in evERA (advanced post-endocrine resistance) and pionERA (post-CDK4/6 resistant). The adjuvant question — does an oral SERD reduce recurrence vs AI in early disease — is being tested in lidERA. Contrast against EMBER-3 (imlunestrant) and SERENA-6 (camizestrant), where SERDs have shown benefit in selected resistant/ESR1-mutant populations.
PERSEVERA (also styled persevERA) is a Phase 3 randomized trial (NCT04546009) of giredestrant, an investigational oral selective estrogen-receptor degrader, plus palbociclib versus letrozole plus palbociclib in first-line ER-positive, HER2-negative locally advanced or metastatic breast cancer. Approximately 992 patients were randomized 1:1, and investigator-assessed progression-free survival was the primary endpoint.
No. PERSEVERA was a negative trial. The primary investigator-assessed progression-free survival endpoint was not met: median PFS was 33.1 months with giredestrant plus palbociclib versus 28.2 months with letrozole plus palbociclib, with a hazard ratio of about 0.89 that did not reach statistical significance. The results were presented at ASCO 2026 (Abstract LBA1006).
No. Giredestrant is an investigational oral selective estrogen-receptor degrader and is not FDA approved. Because PERSEVERA did not meet its primary endpoint, it did not establish a first-line role for giredestrant plus a CDK4/6 inhibitor in ER-positive, HER2-negative advanced breast cancer.
KOLs and the ASCO discussant have discussed a CDK4/6 'blunting' hypothesis: in the frontline setting, palbociclib suppresses estrogen-receptor-driven cell-cycle progression so effectively that swapping the aromatase inhibitor for an oral SERD adds little incremental benefit. Overall survival showed no difference and response rates were similar between arms, consistent with this interpretation.
Aromatase inhibitor plus a CDK4/6 inhibitor remains the standard first-line therapy in ER-positive, HER2-negative metastatic breast cancer. PERSEVERA suggests oral SERDs do not displace aromatase inhibitors in the untreated first-line setting; their established value remains after endocrine resistance or in ESR1-mutant disease.