1L locally advanced or metastatic urothelial carcinoma — Astellas Pharma + Pfizer (via Seagen) + Merck
Discover KOL Sentiment on EV-302 / KEYNOTE-A39 →Design - Phase 3 enfortumab vedotin + pembrolizumab vs platinum-based chemotherapy, first-line locally advanced/metastatic urothelial carcinoma (NCT04223856 / KEYNOTE-A39).
PFS (co-primary) - Median 12.5 vs 6.3 mo, HR ~0.45.
OS (co-primary) - Median ~31.5-33.8 vs ~15.9-16.1 mo, HR ~0.47-0.51 (near-doubling); ASCO 2026 3.5-yr follow-up OS 33.6 vs 15.9 mo (HR 0.53).
Safety - Grade >=3 treatment-related AEs 61.7% vs 71.9% - lower toxicity with the combination.
Regulatory - FDA approved December 2023 - first-line, regardless of cisplatin eligibility.
Sponsor / drug - Astellas + Pfizer (Seagen) + Merck; Padcev + Keytruda.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.














Top tweets by impressions — click to view on X
Congrats @shilpaonc for oral ab#4502 @ASCO #ASCO25👉https://t.co/dtFXREYI6n👉In the Ph3 EV-302 trial in mUC #bladdercancer, pts achieving a CR had higher PFS & OS w/ EV+P vs. chemo (exploratory…
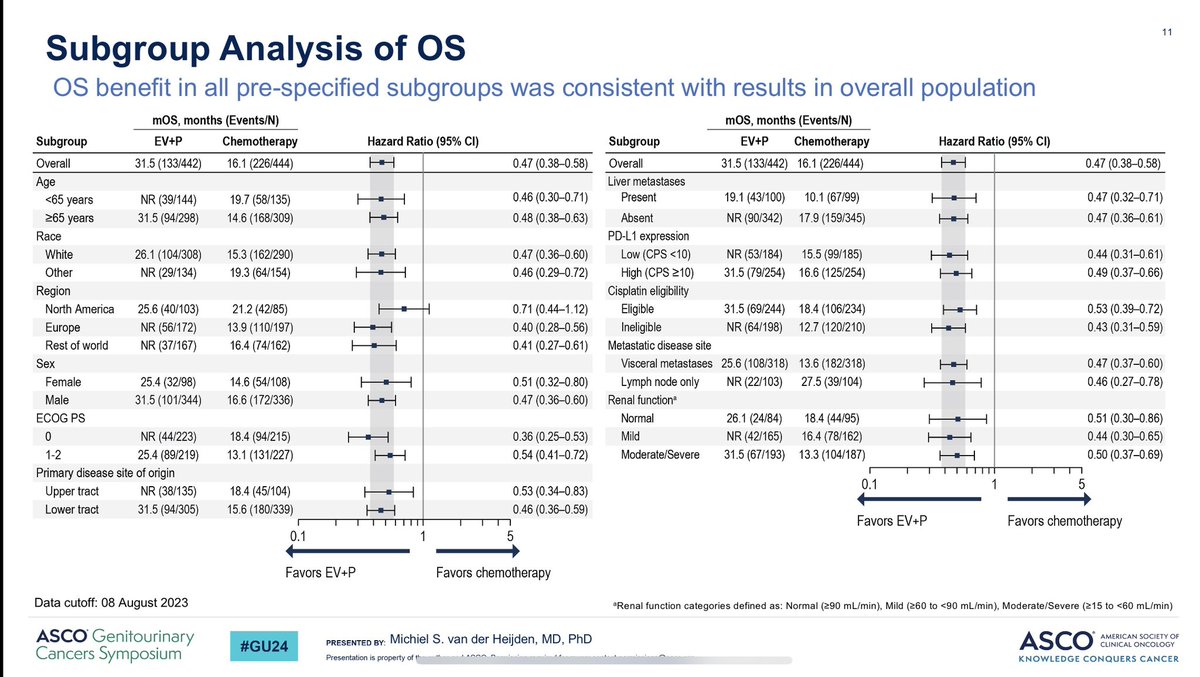
Enfortumab Vedotin + pembro shows broad spectrum of activity for RR PFS and OS in all subgroups. This includes subsets such as lymph node disease, liver mets, PD-L1 status, upper tract disease,…
GU abstracts for #ASCO25!
Schedule & looking forward to:
🔵PARPI in mCSPC #AMPLITUDE
-HRRm analysis #TALAPRO2
-prognosis of PSA>0.2 at 6-12mo in mCSPC
🟠analysis of responders in…
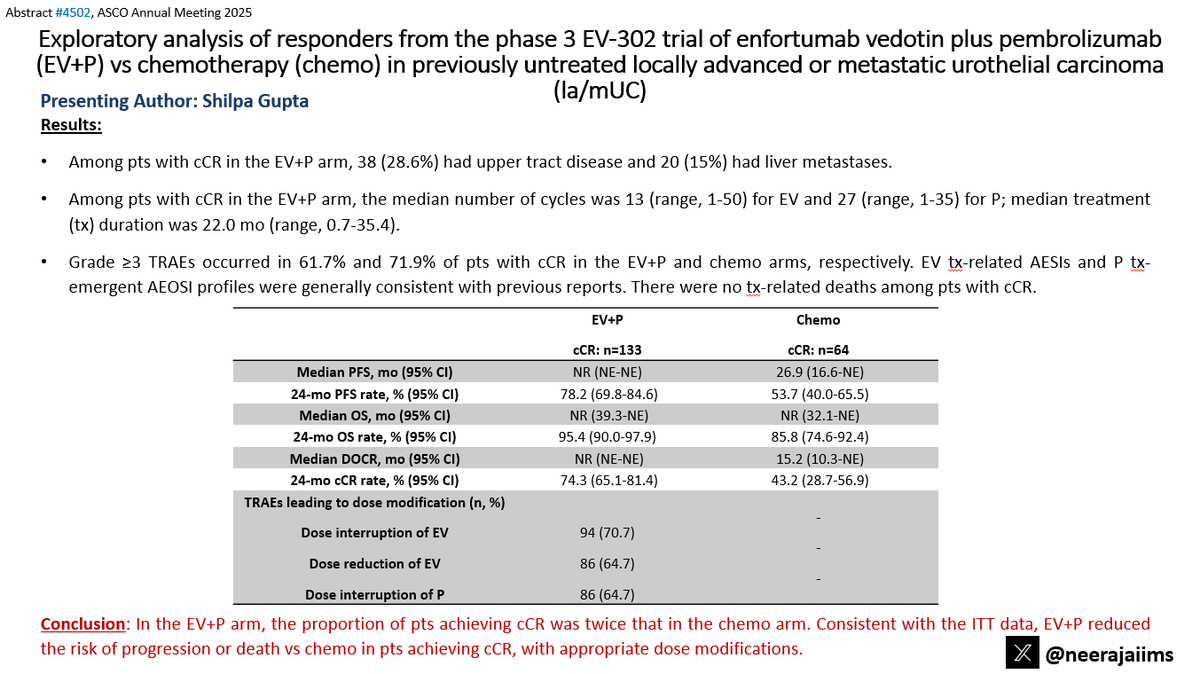
Terrific work by @tompowles1 !! With >2 years of follow-up, 1L EV+P maintains superior OS and PFS vs chemo in la/mUC. cCR rate doubled (30.4% vs 14.5%), with longer response durability and no new…
🌟📢 @ASCO #GU25 |
Abstract #664
🔬 EV-302 confirms superior efficacy of EV+P vs chemo in 1L la/mUC!🌟
@tompowles1 @shilpaonc
📊 Key Findings (N=886, Median FU: 29.1 months)
✅ Median OS: 33.8 vs. 15.9…

#GU24 #bladdercancer highlights in my opinion: 1) AMBASSADOR Phase III @apolo_andrea-improved DFS for adjuvant pembro x 1 year vs. observation in high-risk muscle-invasive #urothelialcarcinoma (HR…
Ab#664 @ASCO #GU25 by @tompowles1👉https://t.co/nR4tDcbKKe 👉Update from ph3 EV-302 in pts w/ met urothelial carcinoma #bladdercancer 👉EV+Pembro vs. chemo: median OS 33.8 vs. 15.9 mo (HR 0.51) 👉⬆️ OS…

#GU25 @ASCO @tompowles1 presents the spectacular data from EV302 with median fu of 2.5 years. EV-pembrolizumab continues to show maintenance of significantly improved OS & PFS compared to…
At @asco #GU25 we will see the 29.1 months median follow-up updated data from EV302!!!! 30.4% of pts in the EV+P arm achieved cCR!! Median duration of cCR was not reached for EV+P vs 15.2 mo (95%…
#ASCO25 abstracts titlkes are out!!!!!
https://t.co/ybAeFhH4He
Much Looking forward to seeing the exciting new data in GU tumors!!!!
See you all in Chicago!!!! @ASCO @ASCOPost @DrChoueiri @tompowles1…
EV+P replaced platinum-based chemotherapy as the preferred 1L regimen for mUC regardless of cisplatin eligibility or PD-L1 status. Near-doubling of OS (33.8 vs 15.9 mo, HR 0.51) is one of the largest efficacy gains in GU oncology in the past decade.
Median PFS was 12.5 months with enfortumab vedotin+pembrolizumab vs. 6.3 months with platinum-based chemotherapy (HR 0.45-0.48, 95% CI 0.38-0.57, P<0.001). ORR 67.5% vs. 44.2%.
Median OS was 31.5-33.8 months (EV+P) vs. 15.9-16.1 months (chemo) — HR 0.47-0.51, 95% CI 0.38-0.61, P<0.00001. Near-doubling of survival; one of the largest efficacy gains in GU oncology.
Grade ≥3 treatment-related AEs occurred in 61.7% with EV+P vs. 71.9% with chemotherapy — LOWER toxicity with the combination. Key AEs: skin toxicity, peripheral neuropathy, hyperglycemia. Active monitoring required.
✅ New 1L standard of care in metastatic urothelial carcinoma. EV+P replaced platinum-based chemotherapy as the preferred 1L regimen for mUC regardless of cisplatin eligibility or PD-L1 status. Near-doubling of OS (33.8 vs 15.9 mo, HR 0.51) is one of the largest efficacy gains in GU oncology in the past decade.
EV-302 (also called KEYNOTE-A39; NCT04223856) is a Phase 3 randomized trial comparing enfortumab vedotin (Padcev) plus pembrolizumab (Keytruda) with platinum-based chemotherapy as first-line treatment for locally advanced or metastatic urothelial (bladder) carcinoma. Progression-free survival and overall survival were co-primary endpoints.
The combination roughly doubled outcomes versus chemotherapy: median PFS was 12.5 versus 6.3 months (HR ~0.45) and median overall survival was about 31.5-33.8 versus 15.9-16.1 months (HR ~0.47-0.51). The ASCO 2026 3.5-year follow-up reported median OS of 33.6 versus 15.9 months (HR 0.53), one of the largest first-line efficacy gains in GU oncology in the past decade.
Yes. In December 2023 the FDA approved enfortumab vedotin-ejfv (Padcev) in combination with pembrolizumab (Keytruda) for the first-line treatment of locally advanced or metastatic urothelial carcinoma, regardless of cisplatin eligibility, based on EV-302.
Grade >=3 treatment-related adverse events were actually lower with the combination than with chemotherapy (61.7% vs 71.9%). Key toxicities of the regimen include skin reactions, peripheral neuropathy, and hyperglycemia, which require active monitoring, but overall the combination was better tolerated on severe-event rates.
Yes. EV-302 established enfortumab vedotin plus pembrolizumab as the preferred first-line regimen for locally advanced or metastatic urothelial carcinoma, displacing platinum-based chemotherapy as the default option regardless of cisplatin eligibility or PD-L1 status.