Phase 3 KEYNOTE-564: adjuvant pembrolizumab (Keytruda) vs placebo in patients with high-risk clear cell renal cell carcinoma (ccRCC) following nephrectomy. The first Phase 3 trial to demonstrate both DFS and OS benefit from adjuvant immunotherapy in RCC — basis for the November 2021 FDA approval. ASCO 2026 ctDNA biomarker analysis presented by Dr. Toni Choueiri (Abstract 4502).
ASCO 2026
RCC May Simply
Be a Poor
ctDNA-Shedding
Tumor.
ONE CORE TAKEAWAY
MV ONCO
KEYNOTE-564 ctDNA ANALYSIS
In the adjuvant setting,
current ctDNA assays
identified <15% of future
recurrences before clinical relapse.
Therefore, ctDNA negativity
may be poorly reassuring.
However, ctDNA positivity
retains strong prognostic value
and marks biologically
higher-risk disease.
Baseline ctDNA
Strong prognostic
positivity: ~5-8%
specificity, limited sensitivity
Choueiri et al ASCO 2026
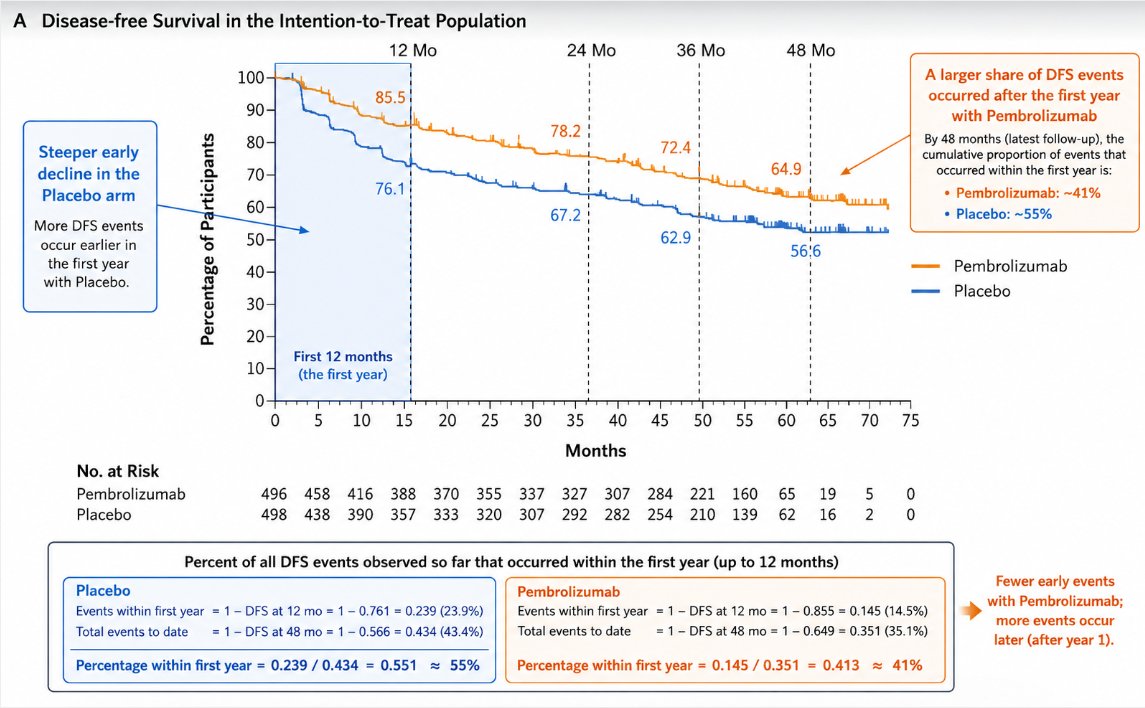
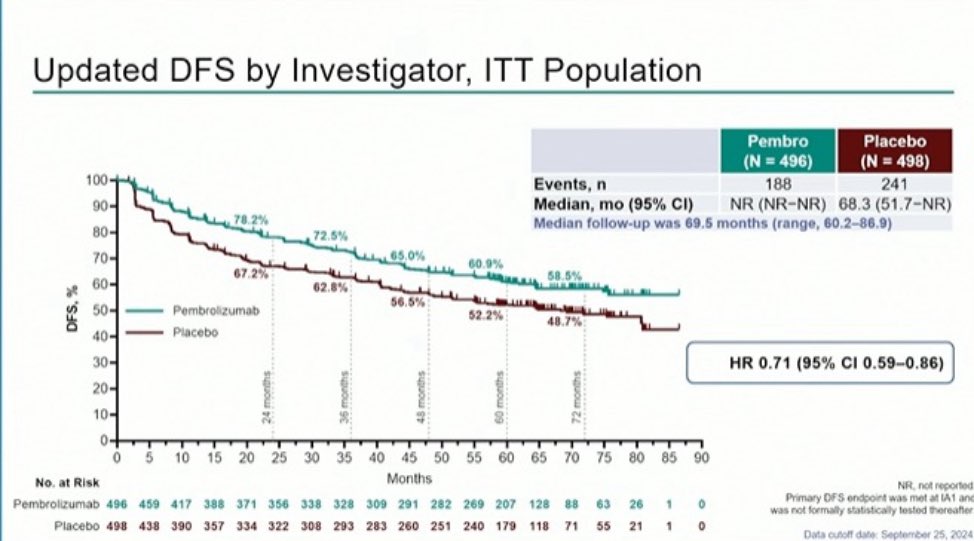
A Disease-free Survival in the Intention-to-Treat Population
12 Mo
24 Mo
36 Mo
48 Mo
100
A larger share of DFS events
85.5
occurred after the first year
90
with Pembrolizumab
78.2
80
72.4
By 48 months (latest follow-up), the
Steeper early
cumulative proportion of events that
decline in the
70
64.9
occurred within the first year is:
Placebo arm
Percentage of Participants
76.1
Pembrolizumab: ~41%
60
67.2
Placebo: ~55%
More DFS events
occur earlier in
50
62.9
56:6
the first year
40
Pembrolizumab
with Placebo.
Placebo
30
20
First 12 months
10
(the first year)
0
0
5
10
15
20
25
30
35
40
45
50
55
60
65
70
75
Months
No. at Risk
Pembrolizumab
496
458
416
388
370
355
337
327
307
284
221
160
65
19
5
0
Placebo
498
438
390
357
333
320
307
292
282
254
210
139
62
16
2
0
Percent of all DFS events observed so far that occurred within the first year (up to 12 months)
Placebo
Fewer early events
Pembrolizumab
with Pembrolizumab;
Events within first year = 1- DFS at 12 mo = 1 - 0.761 = 0.239 (23.9%)
Events within first year = 1- DFS at 12 mo = 1- 0.855 = 0.145 (14.5%)
more events occur
Total events to date = 1- DFS at 48 mo = 1- 0.566 = 0.434 (43.4%)
Total events to date = 1- DFS at 48 mo = 1- 0.649 = 0.351 (35.1%)
later (after year 1).
Percentage within first year = 0.239 / 0.434 = 0.551 ≈ 55%
Percentage within first year = 0.145 / 0.351 = 0.413 ≈ 41%
ASCO
AMERICAN SOCIETY OF CLINICAL ONCOLOGY
KNOWLEDGE CONQUERS CANCER
ASCO Annual Meeting
Abstract #: 4502
Oral Abstract Session
ctDNA analysis in participants with renal cell carcinoma treated with
adjuvant pembrolizumab or placebo in the KEYNOTE-564 trial.
Authors: Toni K. Choueiri, Piotr Tomczak, Naomi B. Haas, David F. McDermott, Balaji Venugopal, Se Hoon Park,
Thomas Ferguson, Stefan N. Symeonides, Wayne Yen Hwa Chang, Jae Lyun Lee, Naveed Sarwar, Piotr Sawrycki,
Chen-Hua Chuang, Yiwei Zhang, Razvan Cristescu, Cai Chen, Carol E. Pena, Rodolfo F. Perini, Joseph E. Burgents,
Thomas Powles
Organizations: Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA, Poznan University of Medical
Sciences, Poznan, Poland, Abramson Cancer Center at the University of Pennsylvania, Philadelphia, PA, Beth Israel
Deaconess Medical Center, Boston, MA, Beatson West of Scotland Cancer Centre and University of Glasgow,
Glasgow, United Kingdom, Sungkyunkwan University, Samsung Medical Center, Seoul, South Korea, Department of
Medical Oncology, Fiona Stanley Hospital, Perth, Western Australia, Australia, Edinburgh ECMC, Edinburgh Cancer
Centre and University of Edinburgh, Edinburgh, United Kingdom, Taipei Veterans General Hospital, Taipei, Taiwan,
Asan Medical Center, University of Ulsan College of Medicine, Seoul, South Korea, Imperial College Healthcare NHS
Trust, London, United Kingdom, Provincial Hospital in Torun, Torun, Poland, Merck & Co., Inc., Rahway, NJ, Barts
Health NHS Trust and the Royal Free NHS Foundation Trust, Barts Cancer Institute, and Queen Mary University of
London, London, United Kingdom
Background:
In the phase 3 KEYNOTE-564 trial (NCT03142334), adjuvant pembrolizumab (pembro) was
superior to placebo (pbo) in participants (pts) with clear cell renal cell carcinoma (ccRCC) at
increased risk of recurrence post nephrectomy. We report an analysis of pretreatment and on-
treatment ctDNA (using 2 versions of a ctDNA assay with different sensitivities) with clinical
outcomes in KEYNOTE-564.
Abstract #4502, ASCO Annual Meeting 2026
ctDNA analysis in participants with renal cell
carcinoma treated with adjuvant pembrolizumab or
placebo in the KEYNOTE-564 trial
Toni K. Choueiri, Piotr Tomczak, Naomi B. Haas, David F. McDermott,
Balaji Venugopal, Se Hoon Park, Thomas Ferguson, Stefan N.
Symeonides, Wayne Yen Hwa Chang, Jae Lyun Lee, Naveed Sarwar, Piotr
Sawrycki, Chen-Hua Chuang, Yiwei Zhang, Razvan Cristescu, Cai Chen,
Carol E. Pena, Rodolfo F. Perini, Joseph E. Burgents, Thomas Powles
@neerajaiims
---
Abstract #4502, ASCO Annual Meeting 2026
ctDNA analysis in participants with renal cell carcinoma treated with adjuvant pembrolizumab or
placebo in the KEYNOTE-564 trial
Presenting Author: Toni Choueiri
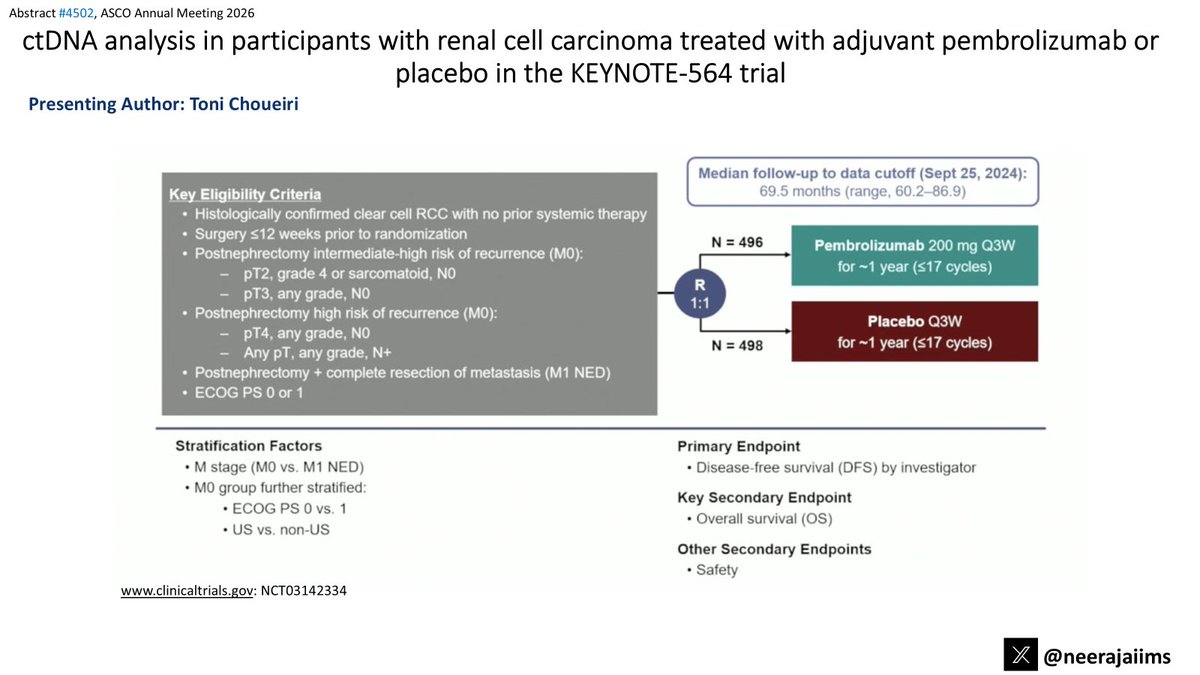
Median follow-up to data cutoff (Sept 25, 2024):
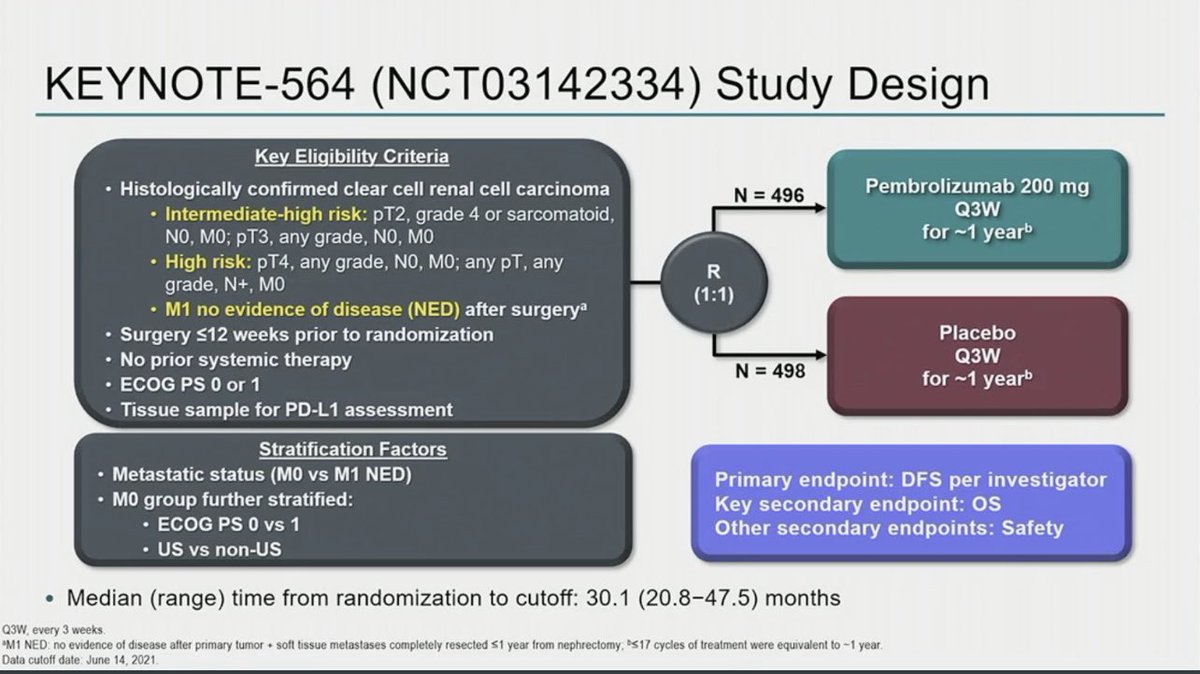
Key Eligibility Criteria
69.5 months (range, 60.2-86.9)
Histologically confirmed clear cell RCC with no prior systemic therapy
Surgery <12 weeks prior to randomization
N = 496
Postnephrectomy intermediate-high risk of recurrence (MO):
Pembrolizumab 200 mg Q3W
- pT2, grade 4 or sarcomatoid, NO
for ~1 year (≤17 cycles)
R
- pT3, any grade, NO
1:1
Postnephrectomy high risk of recurrence (MO):
Placebo Q3W
- pT4, any grade, NO
N = 498
for ~1 year (≤17 cycles)
- Any pT, any grade, N+
Postnephrectomy + complete resection of metastasis (M1 NED)
ECOG PS 0 or 1
Stratification Factors
Primary Endpoint
M stage (MO VS. M1 NED)
Disease-free survival (DFS) by investigator
MO group further stratified:
Key Secondary Endpoint
ECOG PS 0 VS. 1
Overall survival (OS)
US VS. non-US
Other Secondary Endpoints
Safety
www.clinicaltrials.gov: NCT03142334
X
@neerajaiims
---
Abstract #4502, ASCO Annual Meeting 2026
ctDNA analysis in participants with renal cell carcinoma treated with adjuvant pembrolizumab or
placebo in the KEYNOTE-564 trial
Presenting Author: Toni Choueiri
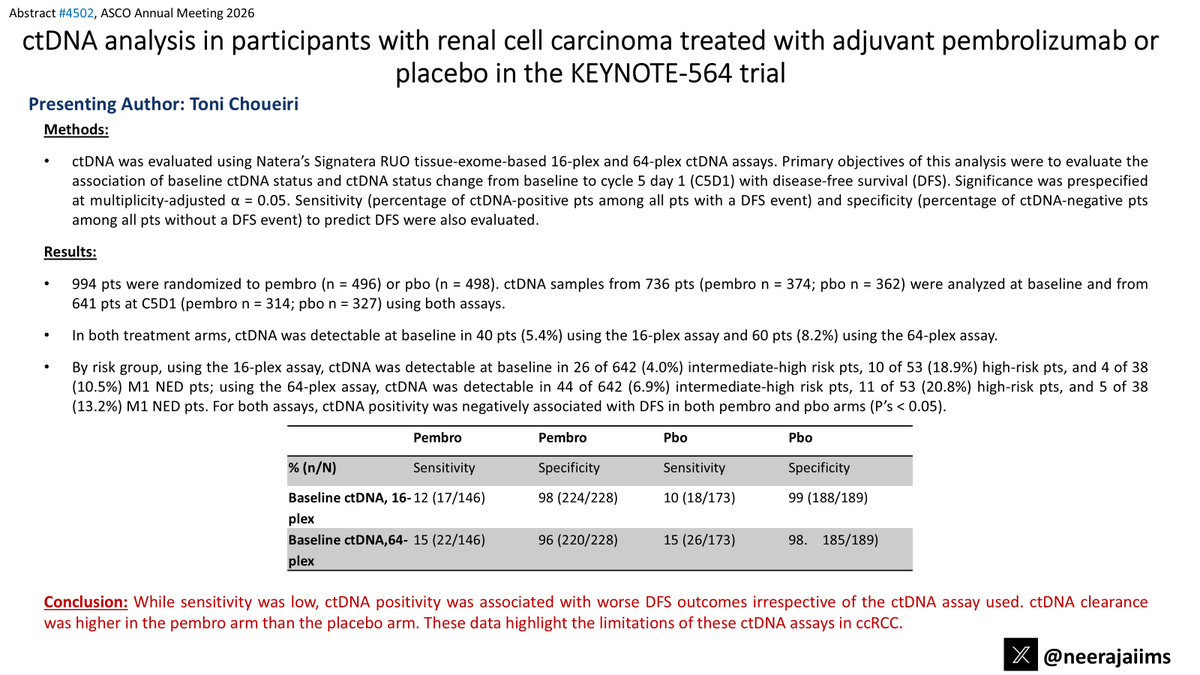
Methods:
ctDNA was evaluated using Natera's Signatera RUO tissue-exome-based 16-plex and 64-plex ctDNA assays. Primary objectives of this analysis were to evaluate the
association of baseline ctDNA status and ctDNA status change from baseline to cycle 5 day 1 (C5D1) with disease-free survival (DFS). Significance was prespecified
at multiplicity-adjusted a = 0.05. Sensitivity (percentage of ctDNA-positive pts among all pts with a DFS event) and specificity (percentage of ctDNA-negative pts
among all pts without a DFS event) to predict DFS were also evaluated.
Results:
994 pts were randomized to pembro (n = 496) or pbo (n = 498). ctDNA samples from 736 pts (pembro n = 374; pbo n = 362) were analyzed at baseline and from
641 pts at C5D1 (pembro n = 314; pbo n = 327) using both assays.
In both treatment arms, ctDNA was detectable at baseline in 40 pts (5.4%) using the 16-plex assay and 60 pts (8.2%) using the 64-plex assay.
By risk group, using the 16-plex assay, ctDNA was detectable at baseline in 26 of 642 (4.0%) intermediate-high risk pts, 10 of 53 (18.9%) high-risk pts, and 4 of 38
(10.5%) M1 NED pts; using the 64-plex assay, ctDNA was detectable in 44 of 642 (6.9%) intermediate-high risk pts, 11 of 53 (20.8%) high-risk pts, and 5 of 38
(13.2%) M1 NED pts. For both assays, ctDNA positivity was negatively associated with DFS in both pembro and pbo arms (P's < 0.05).
Pembro
Pembro
Pbo
Pbo
% (n/N)
Sensitivity
Specificity
Sensitivity
Specificity
Baseline ctDNA, 16-12 (17/146)
98 (224/228)
10 (18/173)
99 (188/189)
plex
Baseline ctDNA,64- 15 (22/146)
96 (220/228)
15 (26/173)
98. 185/189)
plex
Conclusion: While sensitivity was low, ctDNA positivity was associated with worse DFS outcomes irrespective of the ctDNA assay used. ctDNA clearance
was higher in the pembro arm than the placebo arm. These data highlight the limitations of these ctDNA assays in ccRCC.
@neerajaiims
The NEW ENGLAND
JOURNAL of MEDICINE
ESTABLISHED IN 1812
APRIL 18, 2024
VOL. 390 NO. 15
Overall Survival with Adjuvant Pembrolizumab
in Renal-Cell Carcinoma
T.K. Choueiri, P. Tomczak, S.H. Park, B. Venugopal, T. Ferguson, S.N. Symeonides, J. Hajek, Y.-H. Chang, J.-L. Lee,
N. Sarwar, N.B. Haas, H. Gurney, P. Sawrycki, M. Mahave, M. Gross-Goupil, T. Zhang, J.M. Burke, G. Doshi,
B. Melichar, E. Kopyltsov, A. Alva, S. Oudard, D. Topart, H. Hammers, H. Kitamura, D.F. McDermott, A. Silva,
E. Winquist, J. Cornell, A. Elfiky, J.E. Burgents, R.F. Perini, and T. Powles, for the KEYNOTE-564 Investigators*
12
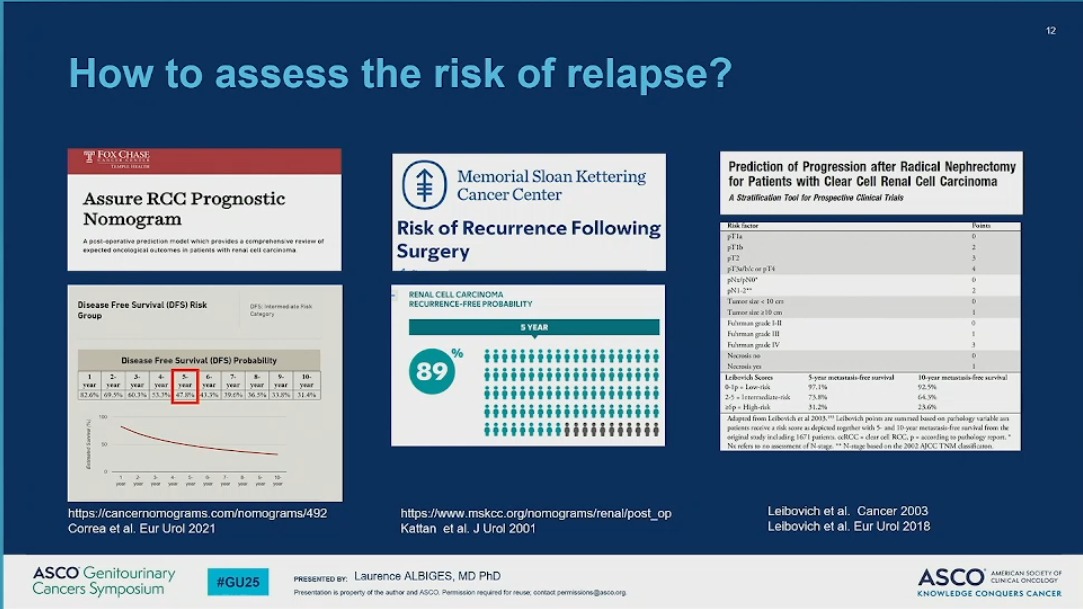
How to assess the risk of relapse?
I FOX CHASE
EMPLE HEALTH
Prediction of Progression after Radical Nephrectomy
Memorial Sloan Kettering
for Patients with Clear Cell Renal Cell Carcinoma
Assure RCC Prognostic
Cancer Center
A Stratification Tool for Prospective Clinical Trials
Nomogram
Risk of Recurrence Following
Risk factor
Posses
PTIs
0
A post operative prediction model which provides comprehensive review of
expected oncelogical outcomes in patients with renal cell carcinoma
Surgery
prib
2
pT2
3
(T)a/ble T4
4
0
RENAL CELL CARCINOMA
pN1-2"
2
Disease Free Survival (DFS) Risk
RECURRENCE-FREE PROBABILITY
Turnor size to on
0
OFS intermed Pask
Group
Category
Tumor size 10 on
I
S YEAR
Fuluman grok 1-11
0
Furman grade III
Furman gode N
%
Nacrods -
0
Disease Free Survival (DFS) Probability
3.
4.
&
7.
1.
9.
10.
89
Necrods yes
2.
6.
Leibevich Scores
5-year metastasis free survival
10. year metastails free service
year
year
year
year
year
year
year
year
year
year
tip. Lew-risk
97.1%
92.5%
82.6%
69.5%
60.3%
53.7%
47.8%
43.3%
19.0%
56.5%
11.8%
31.4%
2-5
73.8%
64.9%
tip High-risk
31.2%
23.6%
100
Adapted from Leibertch " al 2013. Leibersch points IN owned based as purhology variable an
patients receive ** score depicied sogether with and 10 year metastasis free servival from the
I many
original study including 1671 patients. aRCC dear cell RCC. according to purhology report.
to
No refers to to incoment of viage. N-mage based in the 2002 ADCC TNM dissification
2
https://cancernomograms.com/nomograms/492
https://www.mskcc.org/nomograms/renal/post_op
Leibovich et al. Cancer 2003
Correa et al. Eur Urol 2021
Kattan et al. J Urol 2001
Leibovich et al. Eur Urol 2018
ASCO Genitourinary
#GU25
PRESENTED BY: Laurence ALBIGES, MD PhD
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
Cancers Symposium
Presentation is property of the author and ASCO Permission required for reuse contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
19
How to inform the patients?
Recommendation
Strength
rating
If adjuvant therapy is planned:
Strong
Discuss the contradictory results available from adjuvant
ICI trials with the patient to facilitate shared decision-
making
Inform the patient about the potential risk of overtreat-
ment and immune-related side effects if adjuvant therapy
is considered
Bedke J, et al. Updated European Association of Urology Guidelines on the
Use of Adjuvant Immune Checkpoint Inhibitors and Subsequent Therapy for
Renal Cell Carcinoma. Eur Urol. 2025 Feb 3:S0302-2838(25)00026-0.
ASCO Genitourinary
Cancers Symposium
#GU25
PRESENTED BY:
Laurence ALBIGES, MD PhD
ASCO
AMERICAN SOCIETY OF
CUNICAL ONCOLOGY
Presentation is property of the author and ASCO Permission required for reuse contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
41
Can we use a biomarker to select for adjuvant?
The predictive value approach
KIM-1 is associated with DFS benefit of
KIM-1 is associated with DFS benefit of
Atezolizumab in IMMOTION 010
NIVO+IPI in CheckMate 914
DFS analyses in KIM-1, PD-L1 and T-effector1 gene
Figure 4A. Association of KIM-1 levels with DFS
N=584 subjects
signature subgroups
HR: Nivo+Ipi vs Placebo in CA209914
HR (95% CI)
Baseline
Atezolizumab
Placebo
Baseline subgroup
n
a
HR (95% CI)
KMI ist.quartle
1.37 (0.65-2.85)
KIM-1-91
147
143
0.70 (0.50,0.97)
KIM-1
219
1.13 (0.82. 1.54)
KIMI 2nduartie
0.96 (0.51-1.82)
224
PD-L1 positive
KMI 3rd.quartle
0.85 (0.45-1.62)
220
223
0.82 (0.61, 1.10)
PD-L1 negative
151
139
1.04 (0.73, 1.48)
KIMI
0.6 (0.34-1.04)
T-effectormon
191
176
0.87 (0.63.1.21)
T-effectoriow
180
186
0.97 (0.72. 1.33)
HR
0.2
1.0
2
Improved
Poorer
DFSHR
Survival
Survival
POLY
Atezolizumab
better
Placebobetter
-
I
Xu W. et al AACR 2024 Abstract 5151
2024 ASCO
#ASCO24
- Lawrence MD, biomerker INCORD
ASCO
Cancer Res (2024) 84 (6_Supplement): 5151
ASCO Genitourinary
#GU25
PRESENTED BY:
Laurence ALBIGES, MD PhD
ASCO
AMERICAN SOCIETY OF
CUNICAL ONCOLOGY
Cancers Symposium
Presentation is property of the author and ASCO Permission required for reuse contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
42
Can we use a biomarker to select for adjuvant?
The ctDNA approach: are we getting better in RCC?
Patient 65
Large scale retrospective longitudinal monitoring in
1
ctDNA (MTM/mL)
post operative setting is needed to further move to
0.1
prospective trial validation
0.01
ND
0-0-0-0
ctDNA
0
5
10
15
1.00
HR 1.31
1.00
(95% CI: 0.77-2.23)
Time Since First ctDNA Time Point (months)
ctDNA
HR 1.14
(tDNA positive
-
0.75
(95% Cl:0.81-1.62)
|
Procebility of survival e
0.75
tONA negative
PD
Axitinit/pembrolizumab
0.50
0.50
ctDNA*:
HR 0.58
(95% CI: 0.43-0.79)
Probability of overall survival
Basu et al. JCO Precison Oncology 2024
0.25
0.25
ctDNA
HR 0.59
(95% CI: 0.41-0.86)
Real-world data
0
0
commercial ctDNA testing
0
10
20
30
40
50
0
10
20
30
40
50
No. risk
Time (months)
Time (months)
(Signatera, Natera, Inc)
Atezolizumab
184
144
85
44
5
0
184
174
129
57
10
0
ctDNA
Observation
183
140
90
46
6
0
183
170
130
65
7
0
N= 92 (490 plasma samples) pts
Atezolizumab
116
48
25
13
2
0
116
88
55
25
4
0
ctDNA*
Observation
98
17
10
5
1
0
98
54
24
11
1
0
with metastatic RCC
Powles et al. Nature 2021
ASCO Genitourinary
#GU25
PRESENTED BY: Laurence ALBIGES, MD PhD
ASCO
AMERICAN SOCIETY OF
CUNICAL ONCOLOGY
Cancers Symposium
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
Multiple risk calculators exist
UISS (Zisman et al 2002) — DFS of 80.4% at 5 years
SSIGN (Frank et al 2002) - DFS of 89.8% at 5 years
MSKCC (Kattan et al 2001) - DFS of 90% at 5 years
2018 Leibovich (Leibovich et al 2018) - PFS of 75% at 5 years
ASSURE (Andres et al 2021) - DFS of 78.5% at 5 years
2025 ASCO
#ASCO25
PRESENTED BY:
ASCO
AMERICAN SOCIETY or
CUNICAL ONCOLOGY
ANNUAL MEETING
Presentation - property of the who and ASCO Permission required lo - sentact perrissons@asco.org
KNOWLEDGE CONQUERS CANCER
---
17
Cytoreductive nephrectomy (CN)
SURTIME and CARMENA showed worse outcomes with immediate CN1-2
Post-hoc analysis suggest better outcomes with CN in the IO era³⁻⁴
Current SOC is to consider CN only if symptomatic or in selected cases
Delayed CN is recommended over immediate/upfront CN in these selected cases
Ongoing Phase 3 trials may clarify this issue (NORDIC-SUN-Trial, PROBE
and others)
ex A, et al. JAMA Oncol. 2019 PMID 30543350
3. Shen X-P, et al. Eur Rev Med Pharmacol Sci. 2023 PMID 37401306
lejean A, et al. NEJM 2018. PMID 29860937
4. Grim M-O, et al. Eur Urol. 2024. PMID 37852850
ASCO
#ASCO25
PRESENTED BY:
ASCO
AMERICAN SOCIETY O
CUNICAL ONCOLOGY
INUAL MEETING
Presentation . property of the author and ABCO Permission required for - contact perrissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
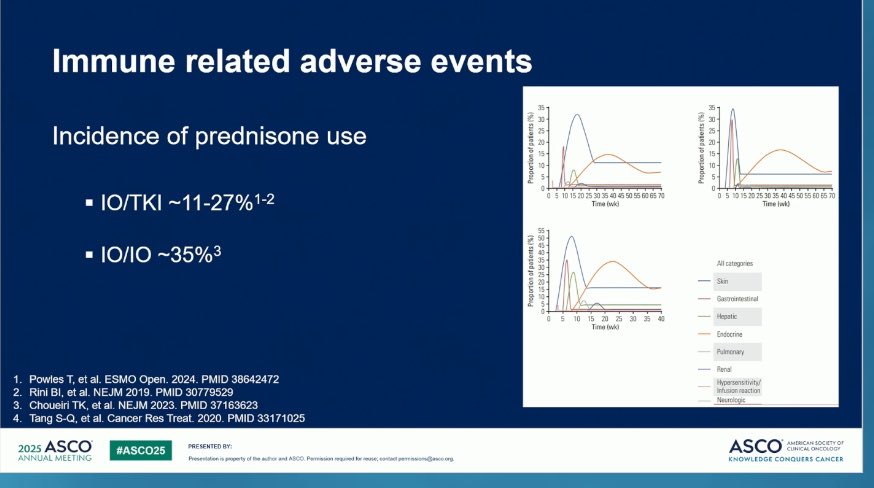
Immune related adverse events
35
35
30
R
Incidence of prednisone use
Propertion patients (%)
25
20
15
Propertion of patients (%)
25
R
15
10
10
5
5
0
0
IO/TKI ~11-27%1-2
0
1 10152025 303540465055606570
0 5 1015202530 3540 4550 5560 65 70
Time (svk)
Time (wk)
10/10 ~35%³
40
Proportion of patients
35 +
30-
All categories
25-4
20 -
Skin
15-
10-
Gastrointestinal
0
5
10
15
20
25
30
R
40
Hepatic
Time (svk)
Endocrine
Pulmonary
Renal
1. Powles T, et al. ESMO Open. 2024. PMID 38642472
Hypersensitivity/
2. Rini BI, et al. NEJM 2019. PMID 30779529
infusion reaction
3. Choueiri TK, et al. NEJM 2023. PMID 37163623
Neurologic
4. Tang S-Q, et al. Cancer Res Treat. 2020. PMID 33171025
2025 ASCO
#ASCO25
ASCO
AMERICAN SOCIETY or
PRESENTED BY:
CUNICAL ONCOLOGY
ANNUAL MEETING
Presentation property of the who and ASCO Permission required for rease, contact petrinsions@asco.org
KNOWLEDGE CONQUERS CANCER
---
Key Takeaways
Recommendation for adjuvant pembrolizumab should be based
on patient's risk level and informed decision making
GrO
Cytoreductive nephrectomy can be considered in select patients
Management of irAE can be a multidisciplinary effort
025 ASCO
PRESENTED BY:
#ASCO25
ASCO
AMERICA
CLINICAL
NNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse; contact permissions@asco.org
KNOWLEDGE CONQUER
KEYNOTE-564 (NCT03142334) is the landmark Phase 3 trial that brought adjuvant pembrolizumab (Keytruda) into the post-nephrectomy setting for high-risk clear cell renal cell carcinoma (ccRCC) — the first Phase 3 to demonstrate both DFS and OS benefit from adjuvant immunotherapy in RCC. 994 patients with intermediate-high risk, high-risk, or M1-NED ccRCC were randomized 1:1 to pembrolizumab 200 mg IV q3w for up to 17 cycles (~1 year) vs placebo following partial or radical nephrectomy. The trial's primary readout (Choueiri et al., NEJM 2021) showed a 32% reduction in the risk of recurrence (DFS HR 0.68); the final OS analysis (NEJM 2024) demonstrated a statistically significant OS benefit (HR 0.62, 95% CI 0.44–0.87), making KEYNOTE-564 the first adjuvant RCC trial to show survival benefit. At ASCO 2026, Dr. Toni Choueiri (Dana-Farber) presented an exploratory ctDNA biomarker analysis (Abstract 4502) evaluating whether circulating tumor DNA can detect recurrence and refine risk in the adjuvant ccRCC setting.
Population
994 adults with intermediate-high risk, high-risk, or M1-NED clear cell RCC who had undergone partial or radical nephrectomy. Stratified by metastatic stage and (in non-metastatic patients) ECOG PS and geography.
Intervention
Pembrolizumab 200 mg IV every 3 weeks for up to 17 cycles (~12 months total) vs placebo. Randomization 1:1.
Primary Endpoint
Disease-free survival (DFS) by investigator assessment.
Key Secondary
Overall survival (OS), DFS by independent central review, safety, and patient-reported outcomes (PROs). Exploratory: ctDNA biomarker analysis (ASCO 2026).
Efficacy & Safety
Reported Results
Disease-Free Survival (Primary Endpoint)
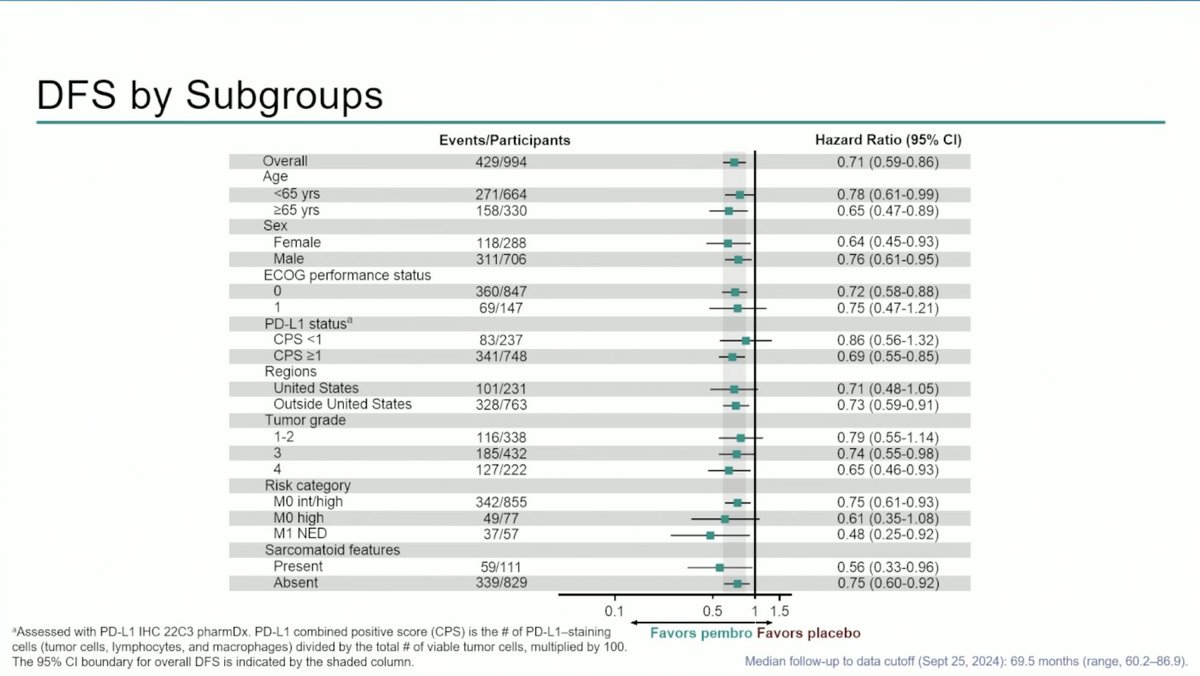
Adjuvant pembrolizumab delivered a 32% reduction in the risk of disease recurrence or death vs placebo: DFS HR 0.68 (95% CI 0.53–0.87; p=0.001) at the primary analysis (Choueiri et al., NEJM 2021). The benefit was consistent across prespecified subgroups, including IMDC intermediate-high, high-risk, and M1-NED disease.
The final OS analysis (NEJM 2024) demonstrated a statistically significant OS benefit with adjuvant pembrolizumab vs placebo: OS HR 0.62 (95% CI 0.44–0.87; p=0.005) — making KEYNOTE-564 the first Phase 3 adjuvant RCC trial to demonstrate a survival benefit. The OS curves continued to separate over time, supporting durable disease control translating into survival gain.
Dr. Choueiri presented an exploratory analysis of circulating tumor DNA in post-nephrectomy ccRCC: baseline ctDNA positivity was associated with worse DFS in both pembrolizumab and placebo arms, validating ctDNA as a prognostic biomarker. However, the assays showed low sensitivity (12–15%) but high specificity (96–99%) for predicting DFS events — suggesting exome-based ctDNA is currently limited as a stand-alone risk stratification tool in this setting. Importantly, pembrolizumab benefit over placebo held across baseline ctDNA subgroups, including the small ctDNA-positive group.
Safety was consistent with the established pembrolizumab profile. Adjuvant pembrolizumab was generally well-tolerated; immune-mediated adverse events were the main toxicity signal, with rates and management consistent with other adjuvant immunotherapy programs.
STATUSFDA Approved · Nov 17, 2021 · Adjuvant Pembrolizumab in High-Risk ccRCC Post-Nephrectomy
On November 17, 2021, the U.S. FDA approved pembrolizumab (Keytruda, Merck) for the adjuvant treatment of adult patients with renal cell carcinoma at intermediate-high or high risk of recurrence following nephrectomy, or following nephrectomy and resection of metastatic lesions (M1-NED). The approval was based on the KEYNOTE-564 primary DFS analysis (HR 0.68). The 2024 final OS readout demonstrated a statistically significant survival benefit (HR 0.62), reinforcing pembrolizumab as the established standard of care in this setting. The ASCO 2026 ctDNA biomarker analysis explores whether ctDNA can refine patient selection going forward.