Adjuvant treatment of clear cell RCC post-nephrectomy at high risk of recurrence — Merck Sharp & Dohme. FDA-approved June 12, 2026; full results published in the New England Journal of Medicine (July 2026).
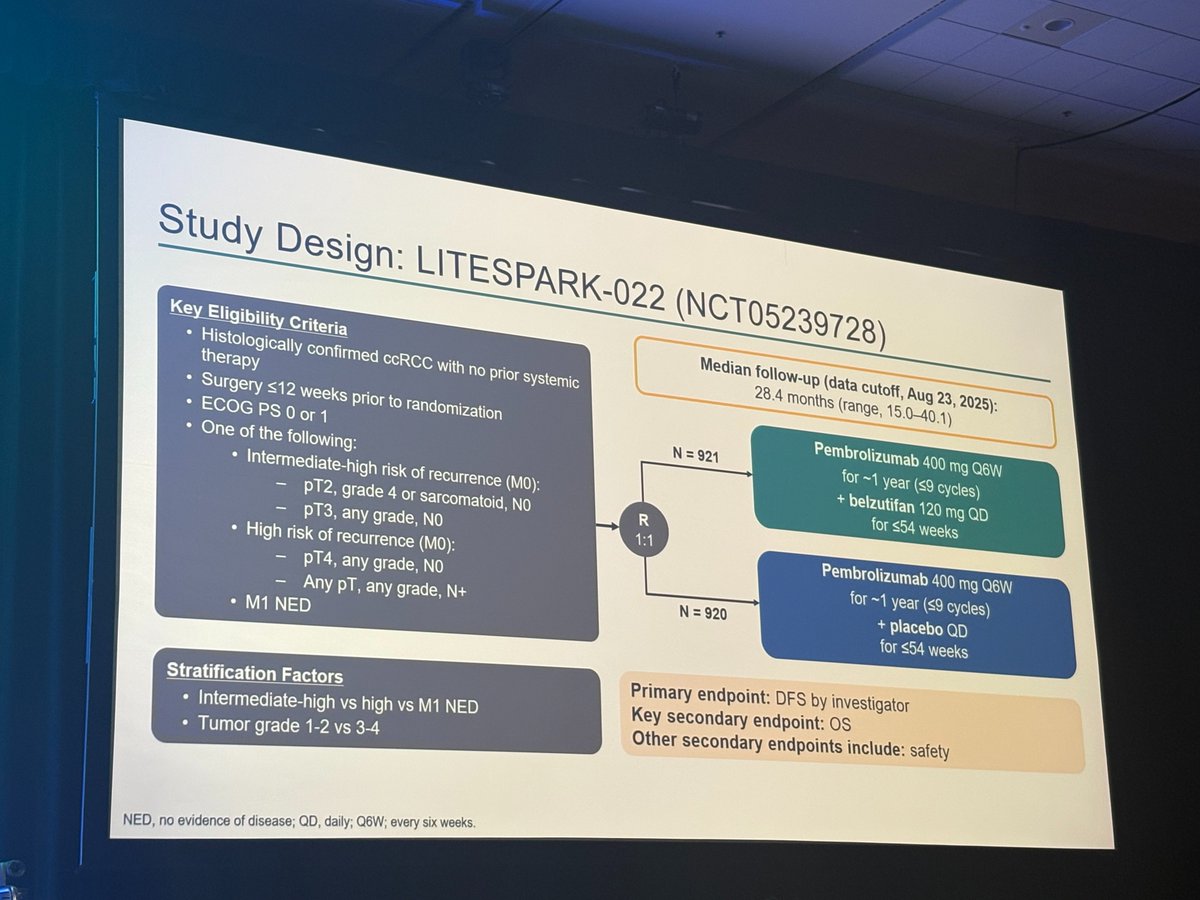
Discover KOL Sentiment on LITESPARK-022 →Read the NEJM Publication (Jul 2026) →Design - Phase 3 adjuvant belzutifan + pembrolizumab vs pembrolizumab + placebo, high-risk ccRCC after nephrectomy, N=1,841 (NCT05239728).
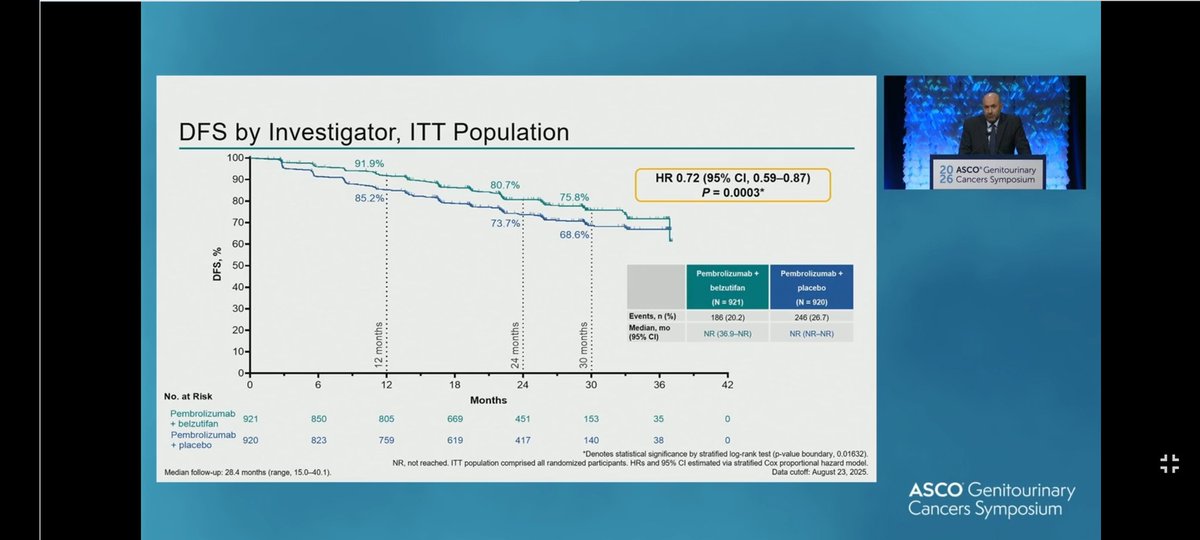
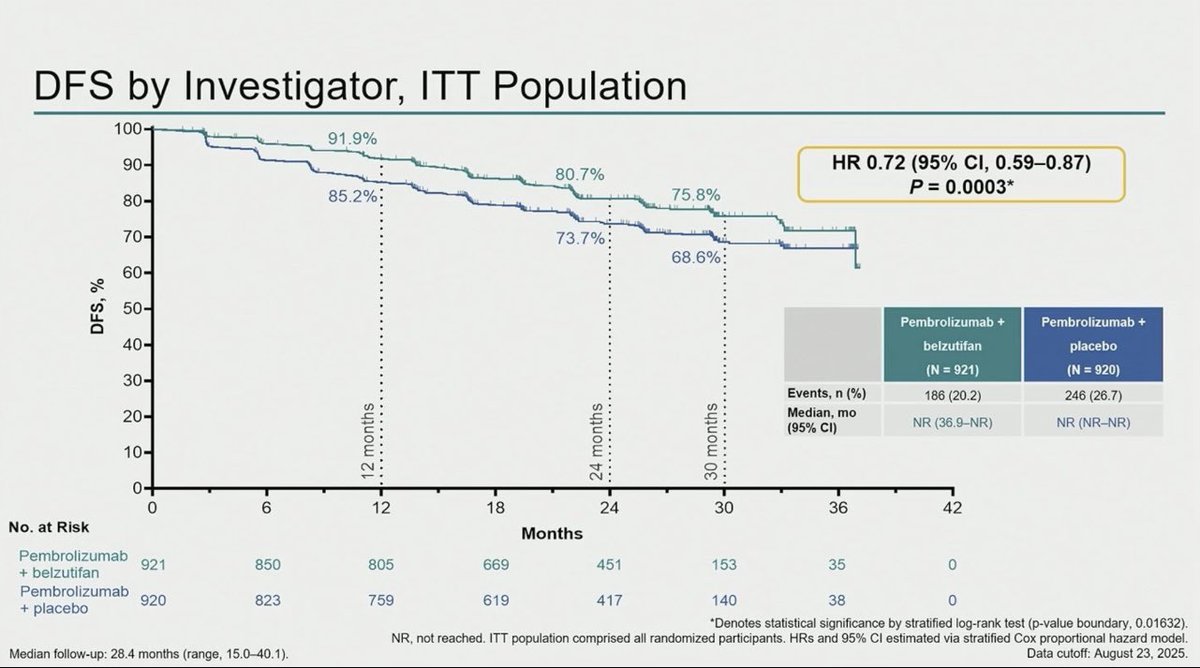
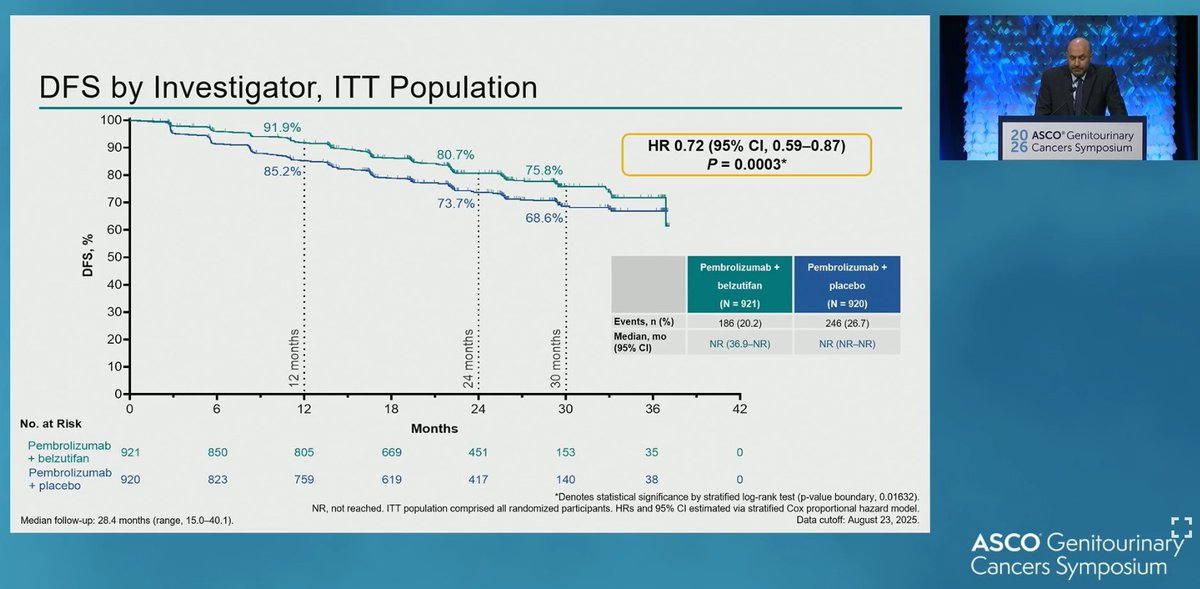
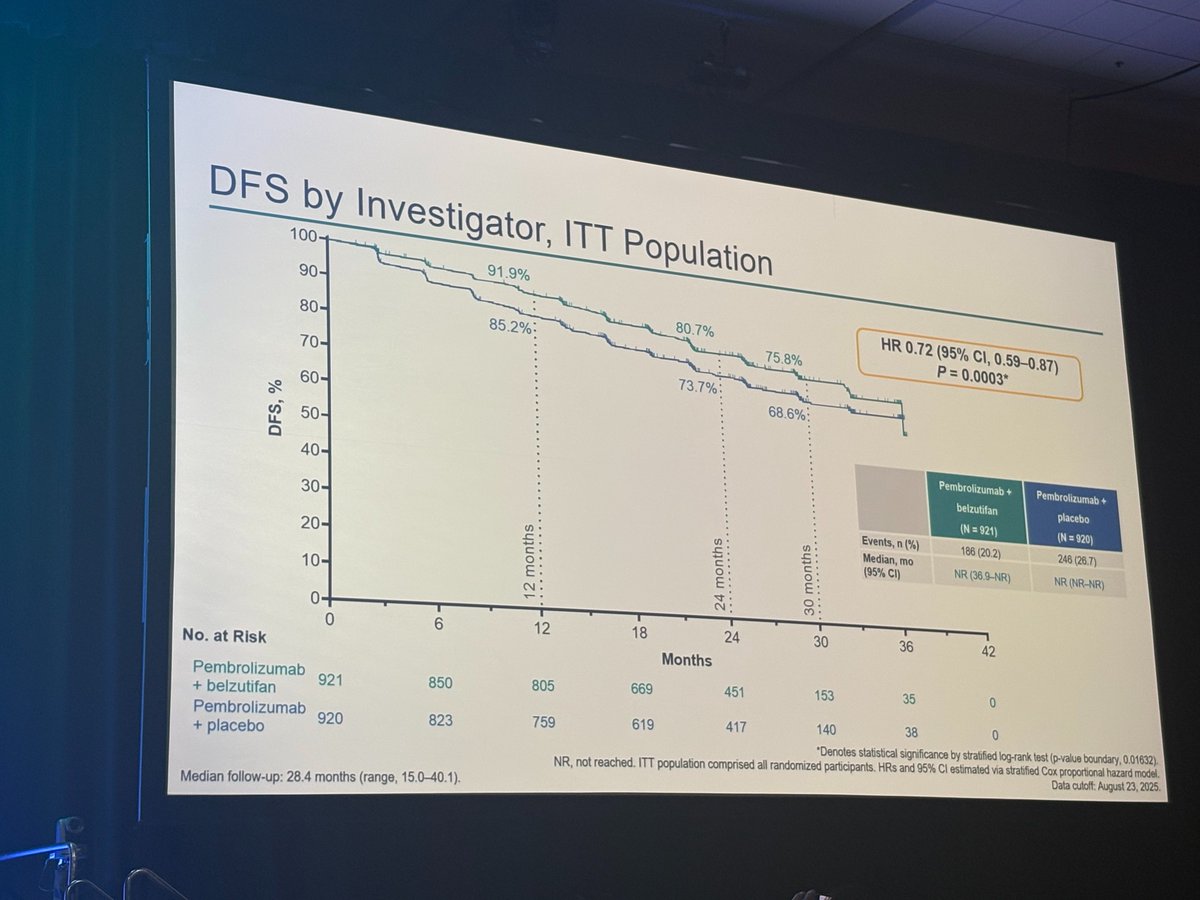
DFS (primary) - HR 0.72 (95% CI 0.59-0.87), P=0.0003 - a 28% relative risk reduction; 24-month DFS 80.7% vs 73.7%; median DFS not reached in either arm.
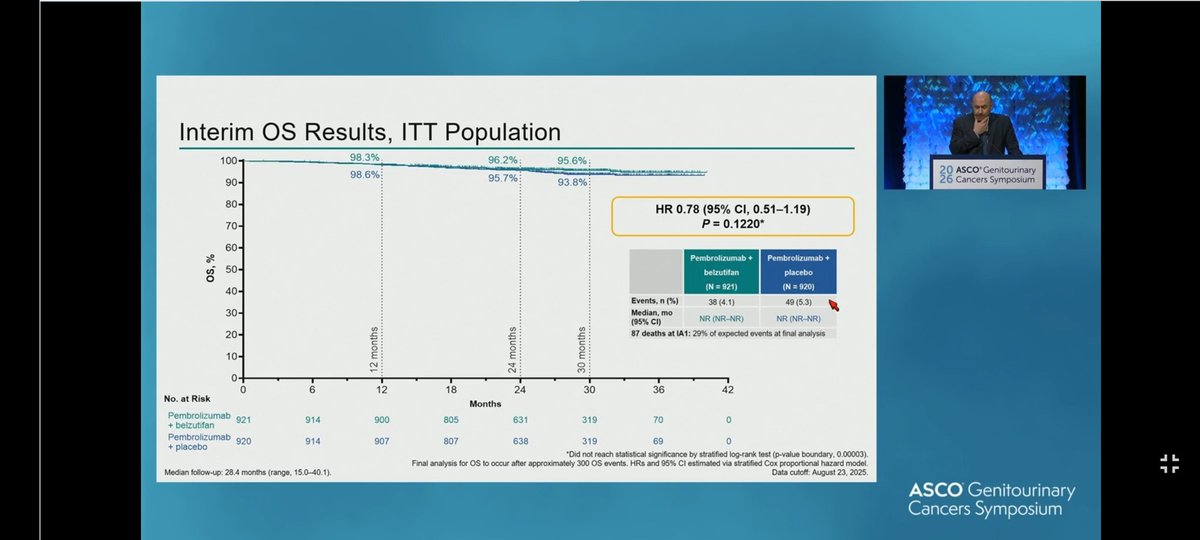
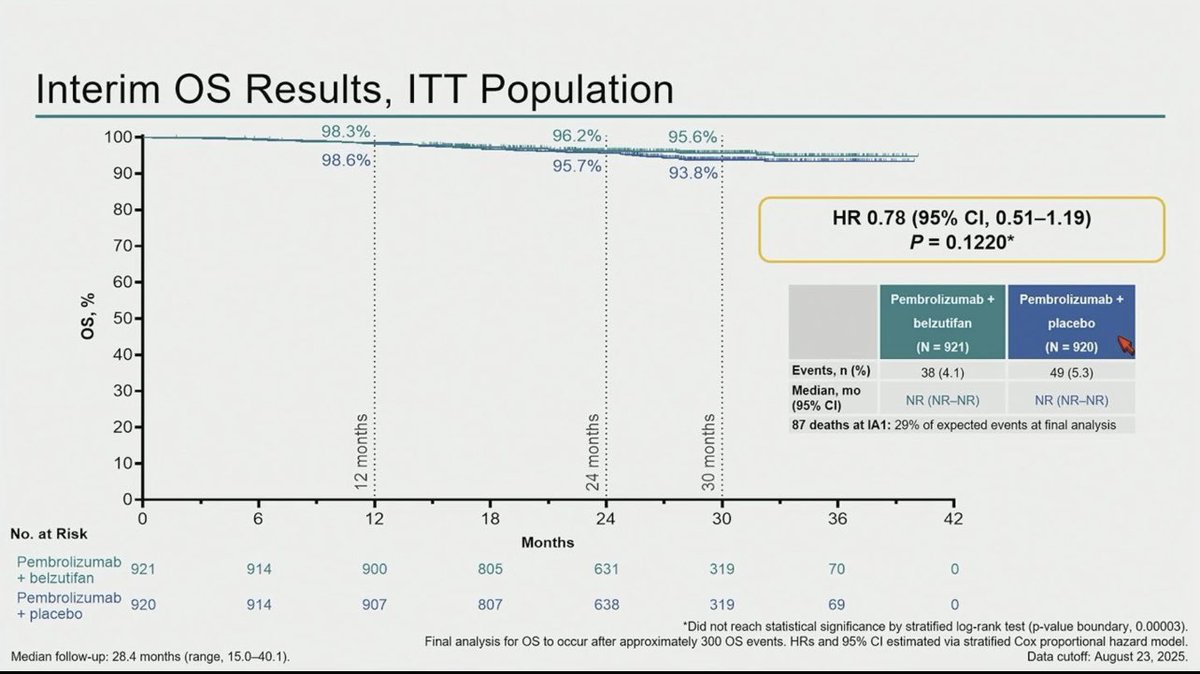
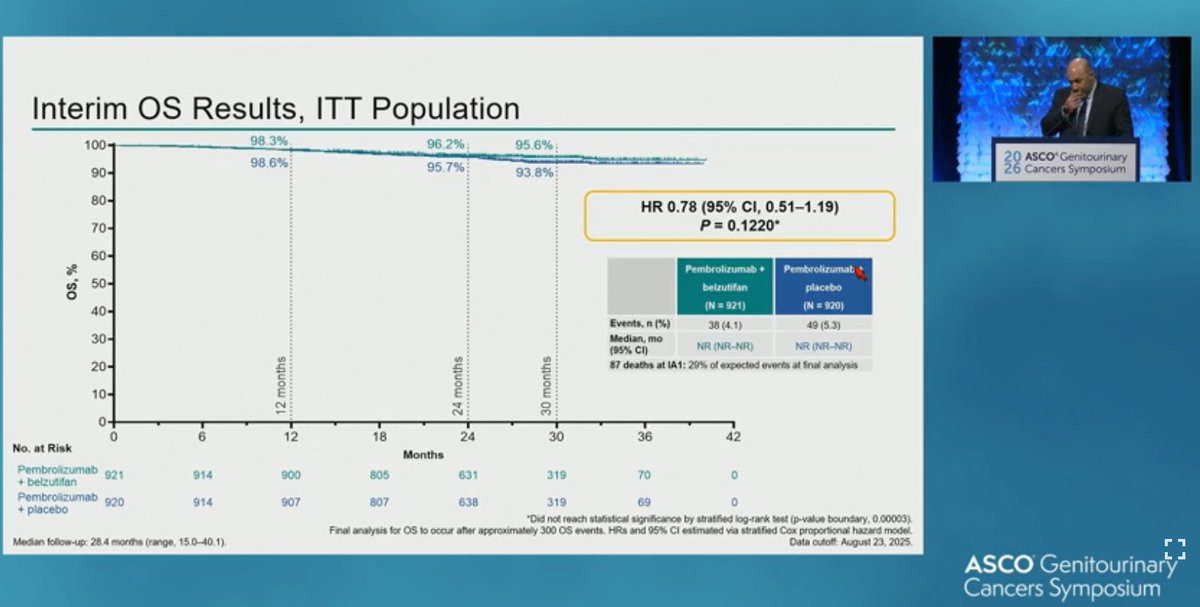
OS - Immature (87 events, ~29% of target); readout expected in subsequent analyses.
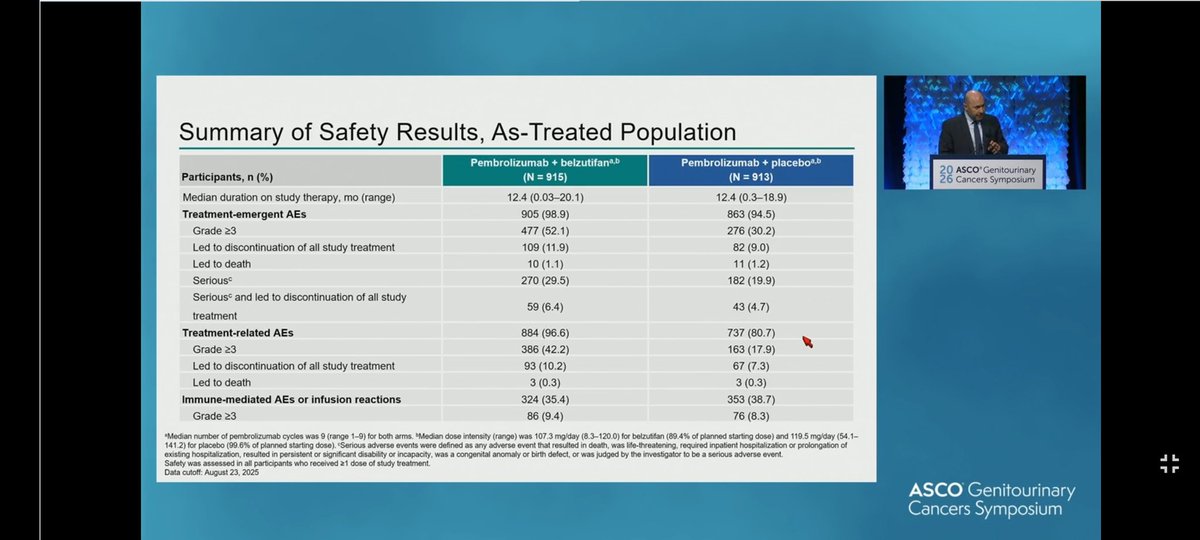
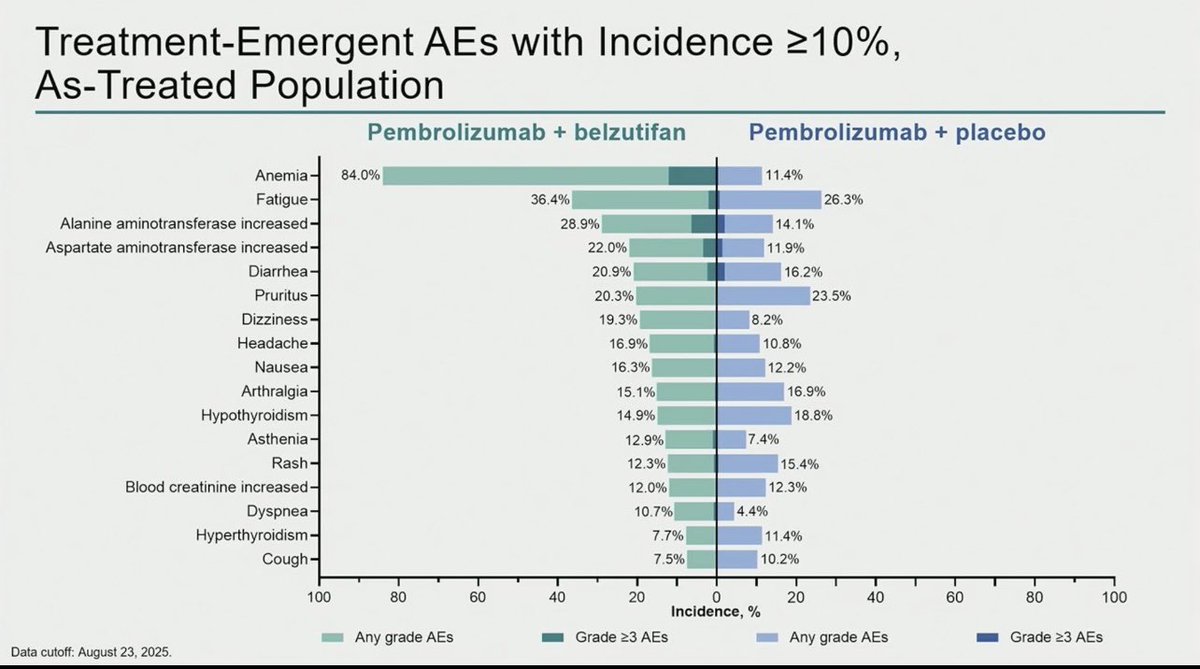
Safety - Higher Grade >=3 adverse events with the combination - dominated by anemia and hypoxia, consistent with the HIF-2alpha mechanism of belzutifan; no new safety signals.
Regulatory - FDA approved June 12, 2026 - belzutifan + pembrolizumab, adjuvant high-risk ccRCC after nephrectomy.
Sponsor / drugs - Merck; belzutifan (Welireg) + pembrolizumab (Keytruda).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.







Top tweets by impressions — click to view on X

🎯 Opening the Best of #KCRS26 plenary, Dr. Tom Powles presents patient reported outcomes from LITESPARK-022, adjuvant pembrolizumab plus belzutifan versus pembrolizumab plus placebo after surgery for ccRCC 🎯 Anemia occurred in 84% of patients on adjuvant pembrolizumab plus belzutifan, yet FKSI-DRS and QLQ-C30 scores stayed stable through week 84 with no clinically meaningful difference versus pembrolizumab plus placebo. An important reminder that AE tables and patient experience are not the same measure @kidneycan

Fascinating to hear from @tompowles1 at #KCRS26 that patient-reported QOL data with belzutifan in Litespark-022 align with toxicity data and is reversible upon discontinuation of treatment

Fitting to see LITESPARK-022 quality-of-life data debut at a patient-advocacy-led meeting. @tompowles1 presenting at #KCRS26. Adjuvant pembro + belzutifan adds reversible grade 3+ toxicity, but the PROs are reassuring: 📊 Symptoms stable, side-effect bother "not at all/a little bit" for >78% 🔍 Physical and role functioning dipped on treatment, then recovered to match placebo 🎯 No clinically meaningful PRO change at week 84 The DFS gain does not come at a lasting quality-of-life cost. Awaiting OS data🩺 #KidneyCancer #RCC #KCRS26 @kidneycan
Adjuvant Pembrolizumab plus Belzutifan in RCC . Litespark022 . Impressive DFS curves. It will become new SOC if it gets OS . Looking forward to OS data in future @DrChoueiri @tompowles1 @OncBrothers…
R3 LITESPARK-022: Adjuvant Pembrolizumab + Belzutifan vs Pembrolizumab for Clear Cell Renal Cell Carcinoma #GU26 showed significantly delayed DFS HR 0.72 (95% CI, 0.59–0.87) active across all…
🆕adjuvant combo for #RCC : LITESPARK-022 #GU26
DFS: HR: 0.72‼️
OS: inmature data..... but comparator arm was THE most effective active treatment available.
@DrChoueiri @tompowles1 @BourlonMaite…
Breaking news from @ASCO #GU26 👉Adding belzutifan to adjuvant pembrolizumab significantly improves disease free survival (HR: 0.72)👉Congrats @drchoueiri & team for changing SOC again in pts with…

Thank you @ASCOPost for this interview about #Litespark022, the first + study of combo in adjuvant Kidney Cancer ! @montypal, @DrRanaMcKay @DrRosenbergMSK we need to update @AUC3_Official ! Data…

#ASCODailyNews: According to phase 3 LITESPARK-022 results, adding belzutifan to pembrolizumab improves DFS in pts with high-risk ccRCC. Read the full #GU26 article: https://t.co/TWsQtiH0xz…

A new standard may be emerging in the adjuvant treatment of high-risk clear cell RCC.
#GU2026 | LITESPARK-022 (Phase 3)
Adjuvant Pembrolizumab + Belzutifan vs Pembrolizumab
🎯…

Big morning for Belzutifan🎉#ASCOGU26
#LITESPARK011 combo w/ Lenva vs Cabo in 2L+ s/p IO in mRCC (55% prior TKI)
➕ PFS, ORR, immature OS, 20 pts w/ CR
⚠️15% hypoxia, 2/3 DR TKI, 1/3 DR…
LITESPARK-022: adjuvant pembrolizumab plus belzutifan vs pembrolizumab for ccRCC #GU26
@DrChoueiri @motzermd @crisuarez08 @DrIacovelli @tompowles1 @DrYukselUrun https://t.co/cFt63B72N7

Adjuvant kidney cancer is evolving.
@DrChoueiri joins the Uromigos to discuss the LITESPARK-022 phase 3 trial of belzutifan + pembrolizumab, mechanistic insights, biomarker development, and what may…
Builds on KEYNOTE-564 (adjuvant pembrolizumab monotherapy) by adding HIF-2α inhibition. 28% relative DFS risk reduction in adjuvant ccRCC. FDA approved June 12, 2026 (belzutifan + pembrolizumab, adjuvant high-risk ccRCC after nephrectomy; LITESPARK-022 DFS HR 0.72). Adds another layer of complexity to the adjuvant RCC treatment landscape alongside monotherapy pembrolizumab and potential future IO-TKI combinations.
DFS HR 0.72 (95% CI 0.59-0.87, P=0.0003) — 28% relative risk reduction favoring belzutifan + pembrolizumab over pembrolizumab + placebo. 24-month DFS rate: 80.7% (combination) vs. 73.7% (monotherapy). Median DFS not reached in either arm.
Overall survival data remain immature (87 events, 29% of target); ongoing follow-up continues. OS readout expected in subsequent analyses.
Higher Grade ≥3 adverse events with the combination — dominated by anemia and hypoxia, consistent with HIF-2α inhibition mechanism of belzutifan. No new safety signals beyond established belzutifan and pembrolizumab profiles.
✅ FDA approved (June 12, 2026) — next-generation adjuvant ccRCC option. Builds on KEYNOTE-564 (adjuvant pembrolizumab monotherapy) by adding HIF-2α inhibition. 28% relative DFS risk reduction in adjuvant ccRCC. On June 12, 2026 the FDA approved belzutifan (Welireg) plus pembrolizumab (Keytruda) for adjuvant treatment of high-risk clear cell RCC following nephrectomy, based on the LITESPARK-022 DFS benefit (HR 0.72). Adds another layer of complexity to the adjuvant RCC treatment landscape alongside monotherapy pembrolizumab and potential future IO-TKI combinations.
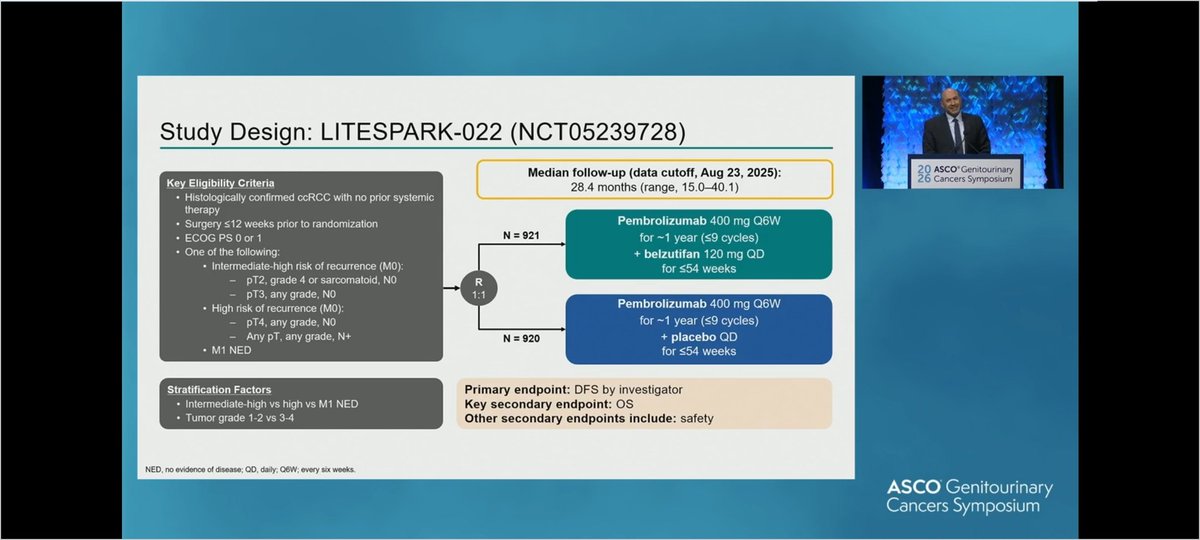
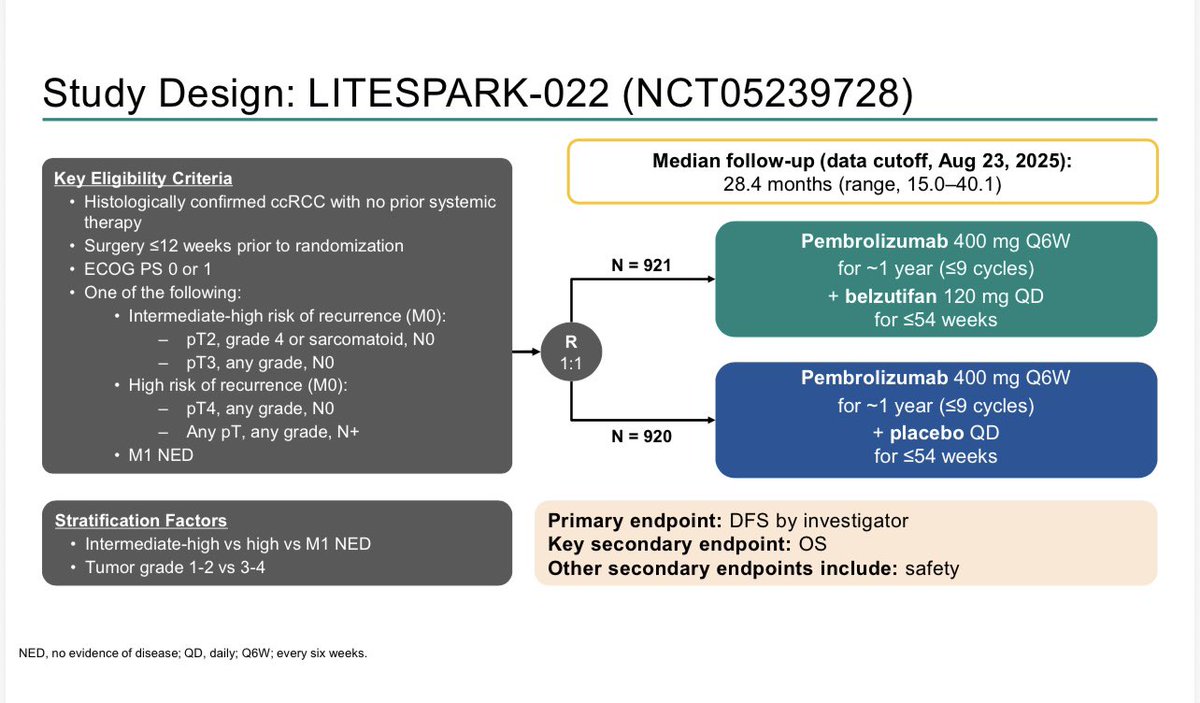
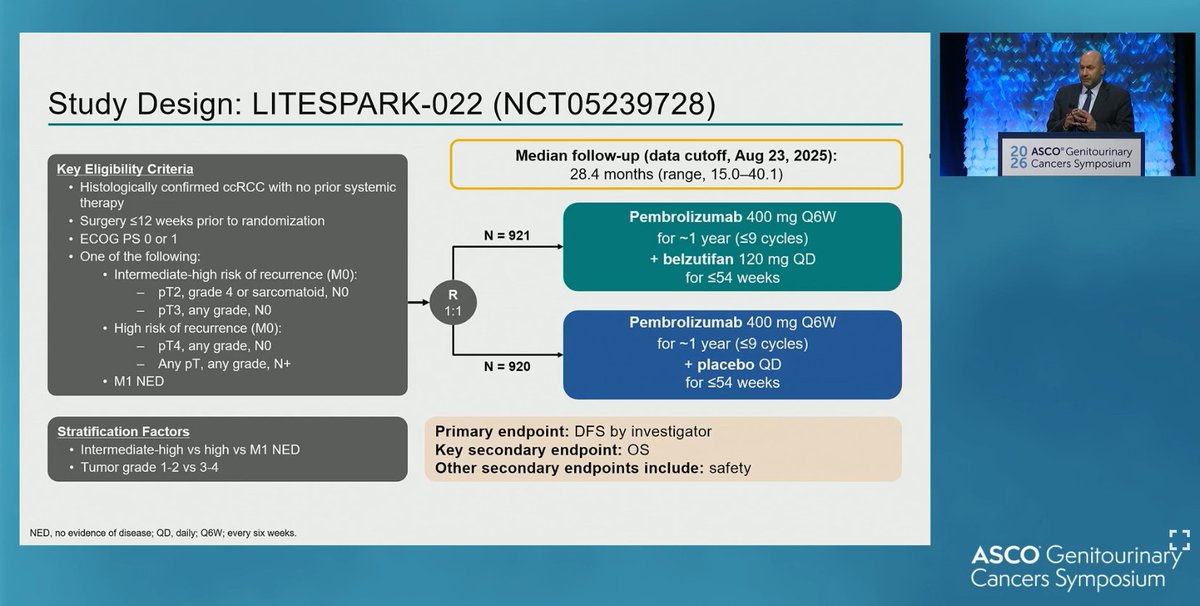
LITESPARK-022 is a Phase 3 multicenter, double-blind, randomized trial (NCT05239728; N=1,841) of adjuvant belzutifan (Welireg), a HIF-2alpha inhibitor, plus pembrolizumab versus pembrolizumab plus placebo in patients with clear cell renal cell carcinoma at intermediate-high or high risk of recurrence after nephrectomy. Disease-free survival was the primary endpoint.
Adding belzutifan to adjuvant pembrolizumab significantly improved disease-free survival: HR 0.72 (95% CI 0.59-0.87; P=0.0003), a 28% relative reduction in the risk of recurrence or death, with a 24-month DFS rate of 80.7% versus 73.7% and median DFS not reached in either arm. Overall survival data remain immature.
Yes. On June 12, 2026 the FDA approved belzutifan (Welireg) in combination with pembrolizumab (Keytruda) for the adjuvant treatment of renal cell carcinoma with a clear cell component at intermediate-high or high risk of recurrence following nephrectomy, or following nephrectomy and resection of metastatic lesions, based on the LITESPARK-022 disease-free survival benefit.
The combination produced more Grade 3 or higher adverse events than pembrolizumab alone, dominated by anemia and hypoxia - the expected on-target consequences of HIF-2alpha inhibition with belzutifan - plus the immune-mediated events associated with pembrolizumab. The belzutifan label carries a boxed warning for embryo-fetal toxicity and warnings for anemia and hypoxia; no new safety signals were identified.
KEYNOTE-564 established adjuvant pembrolizumab monotherapy as a standard for high-risk clear cell RCC after nephrectomy. LITESPARK-022 builds on that by adding HIF-2alpha inhibition with belzutifan, further improving disease-free survival and providing a next-generation adjuvant option, while adding anemia and hypoxia to the toxicity profile that clinicians must manage.