Phase 3 POTOMAC: durvalumab (Imfinzi) added to BCG induction and maintenance vs BCG alone in BCG-naïve, high-risk non-muscle-invasive bladder cancer (NMIBC). FDA-approved May 28, 2026 — the first new therapy for BCG-naïve high-risk NMIBC in over 30 years.
FDA Approved 2026-05-28 · DFS HR 0.68BCG-naïve High-Risk NMIBCPhase 3 · NCT03528694Durvalumab + BCG vs BCG Alone · AstraZenecaFDA Approved May 28, 2026
Design - Phase 3 randomized durvalumab (Imfinzi) + BCG induction and maintenance vs BCG alone in BCG-naive high-risk NMIBC (NCT03528694; AstraZeneca).
DFS (primary) - 32% reduction in risk of disease recurrence, progression, or death vs BCG alone: HR 0.68 (95% CI 0.50-0.93; p=0.0154) at median follow-up 60.7 months.
5-year OS (ASCO 2026 update) - No overall-survival detriment at the planned 5-year analysis (data cutoff 03 Oct 2025; median follow-up 72 months): HR 0.81 (95% CI 0.54-1.19).
Safety - Grade 3/4 treatment-related adverse events 21% (durvalumab + BCG) vs 4% (BCG alone); no treatment-related deaths; profile consistent with known durvalumab safety.
Regulatory - FDA approved per page May 28, 2026 (durvalumab + BCG, BCG-naive high-risk NMIBC) - GATE to confirm.
Sponsor / drug - AstraZeneca; durvalumab (Imfinzi) + BCG.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.
Top Voices
KOL Leaders Discussing POTOMAC
Ashish M. Kamat, MD, MBBS
@UroDocAsh
13,076 impressions
Andrea Necchi
@AndreaNecchi
12,511 impressions
Toni Choueiri, MD
@DrChoueiri
7,432 impressions
FDA Oncology
@FDAOncology
6,272 impressions
Oncology Brothers
@OncBrothers
4,505 impressions
Vignesh Packiam, MD
@VigneshPackiam
3,507 impressions
Medical Digest & Congress Report
@MedicalDigestCR
3,101 impressions
OncUpdates
@OncUpdates
2,941 impressions
Conference Data
Key Slides & Data
New · ASCO 2026 Annual Meeting
POTOMAC 5-year update presented June 1, 2026 (Maria De Santis, MD). At the planned 5-year overall survival analysis (data cutoff 03 October 2025; median follow-up 72 months), adding durvalumab to BCG (induction + maintenance) showed no detriment to OS — HR 0.81 (95% CI 0.54–1.19); 5-year OS 87.6% vs 86.3% (deaths 45 [13%] vs 56 [16%]; median OS not reached in either arm). Durvalumab did not have a major impact on patient-reported quality of life, with generally similar PROs between arms.
[Slide 1]
POTOMAC: Study Design
Durvalumab 1500 mg IV (Q4W X 13 cycles)
Primary endpoint
D+BCG (I+M)
BCG Maintenance
Study population
N=339
BCG Induction
DFS: D+BCG (I+M) vs BCG (I+M)
3 weekly doses at
Age ≥18 years
Weekly x 6 weeks
3m
6m
12m
18m
24m
NMIBC
Secondary endpoints
BCG-naive
5-year OS rate
High-risk tumor defined
Durvalumab 1500 mg IV (Q4W X 13 cycles)
(data cutoff 03 October 2025)
R
D+BCG
as any of the following:
Patient-reported outcomes
(1:1:1)
(I only)
T1
BCG Induction
N=1018
(data cutoff 03 April 2025)
N=339
High-grade/G3
Weekly x 6 weeks"
CIS
Multiple and
recurrent and large
(≥3 cm)
BCG (I+M)
BCG Maintenance
N=340
BCG Induction
3 weekly doses at
Weekly X 6 weeks"
3m
6m
12m
18m
24m
Stratification factors:
First patient enrolled: June 2018
Higher-risk papillary disease (T1G3/T1 high-grade or multiple and recurrent and large tumors)
Last patient enrolled: October 2020
CIS
Last D dose: January 2022
Last BCG dose: January 2023
De Santis M, et al Lancet 2025;406.2221-2234 All disease assessments were performed by the investigator For patients with persistent CIS disease at 3 months, a single BCG res induction was administered
weekly for 6 weeks according to local standard practice BCG, bacillus Calmette- Guérin; CIS, carcinoma in situ: D. durvalumab DFS, disease free survival; G, grade; 1, induction; IV, intravenous; m, month;
2026 ASCO
#ASCO26
M. maintenance, OS, overall survival; NMIBC, muscle invasive bladder cancer, Q4W, every 4 weeks; R, randomization
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 2]
POTOMAC: 5-Year Overall Survival - ITT
No detriment at the 5-year OS analysis was observed with the addition of durvalumab to BCG (I+M) therapy
D+BCG (I+M)
BCG (I+M)
N=339
N=340
Deaths, n (%)
45 (13)
56 (16)
Median OS
NR
NR
1.0
88%
(95% CI), months
(NR-NR)
(NR-NR)
0.8
86%
Probability of OS
0.6
0.4
HR 0.81 (95% CI, 0.54-1.19)
0.2
Median follow-upᵃ: 72 months
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
51
54
57
60
63
66
69
72
75
78
81
84
87
90
Time from randomization (months)
No. of patients at risk
D+BCG (I+M) 339 336 329 326 324 320 319 315 314 311 306 303 298 296 293 290 290 286 283 277 270 236 217 182 141 115 73 30 11 1 0
BCG (I+M) 340 338 336 333 330 328 326 322 317 313 313 313 309 305 301 295 292 288 284 281 275 239 220 185 140 108 70 32 12 0 0
in censored patients across treatment arms Data cutoff 03 October 2025. OS is the time from randomization until death due to any cause regardless of whether the patient withdraws from randomized therapy or
receives another anti-cancer therapy BCG, bacillus Calmette-Guérin CI, confidence interval; D, durvalumab; HR hazard ratio, I, induction ITT, intent to treat population; M, maintenance NR, not reached; OS,
2026 ASCO
#ASCO26
overall survival
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 3]
POTOMAC: EORTC QLQ-C30 Change From Baseline
Adjusted mean changes from baseline showed modest deterioration in GHS/QoL and physical functioning and increased fatigue
in both treatment arms, with generally similar changes between treatment arms
GHS/QoL1
Physical Functioning
Fatigue
Difference between arms: -2.7 (95% CI, -4.85 to -0.54)
Difference between arms: -2.6 (95% CI, -4.43 to -0.81)
Difference between arms: 4.0 (95% CI, 1.50 to 6.46)
20
20
20
Adjusted mean change
10
from baseline
Better
Worse
-20
Adjusted mean change
10
from baseline
Better
0
Adjusted mean change
10
Worse
0
-10'
from baseline
0
-10
Worse
-10
Better
-20
-20
2
10
18
26
34
42
50
58
66
74
82
90
98
106114122130138146
2
10
18
26
34
42
50
58
66
74
82
90
98
106
2
10
18
26
34
42
50
58
66
74
82
90
98
106114122130138146
Visit (weeks)
Visit (weeks)
Visit (weeks)
No of patients in analysis
No of patients in analysis
No of patients in analysis
D+BCG (I+M)214 202 189 180 177 174 171 156 149 142 148 135 138 130 126 122 117 104 105
D+BCG (I+M)214 202 189 180 177 174 171 156 149 142 148 138 138 130 126 122 117 104 105
D+BCG (1+M)214 202 189 180 177 174 171 156 149 142 148 138 138 130 126 122 117 104 105
BCG (I+M)232 219 213 192 193 178 183 158 165 165 158 149 152 138 139 133 120 124 123
BCG (I+M)232 219 213 192 193 178 183 158 165 165 158 149 152 138 139 133 120 124 123
BCG (I+M)232 219 213 192 193 178 183 158 165 165 158 149 152 138 139 133 120 124 123
Clinically meaningful change from baseline
1. De Santis M, of al Lancet 2025:406 2221-2234 Data cutoff 03 April 2025 Decreases indicate worsening for GHS/QoL and physical functioning; increases indicate worsening for fatigue Error bars show 95%
CI Change from baseline was analyzed using mixed model for repeated measures and heterogenous Toeplitz, with stratification factors, treatment, visit, baseline score treatment by-visit and baseline score-
by-visit interactions as explanatory variables Only patients with an evaluable baseline score and at least evaluable postbaseline score are included in the analysis model A clinically meaningful change was
defined as a 10 point change in score compared with baseline. BCG, bacillus Calmette-Guérin CFB, change from baseline, CI, confidence interval, D. durvalumab; EORTC QLQ-C30 European Organisation for
2026 ASCO
#ASCO26
Research and Treatment of Cancer 30 item core quality of life questionnaire GHS/QoL global health scale/quality of Me, I, induction, M, maintenance
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse; contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 4]
POTOMAC PRO-CTCAE Symptoms
PRO-CTCAE Symptom Worsening on Treatment Through Week 106
Abdominal pain
76% (39/51)
D+BCG (I+M)
(Interference)
68% (40/59)
BCG (I+M)
Across abdominal pain, diarrhea, and
Abdominal pain
67% (162/241)
painful urination, rates of PRO-CTCAE
(Frequency)
63% (156/246)
worsening were similar between treatment
Abdominal pain
59% (30/51)
arms through Week 106, consistent with the
(Severity)
63% (37/59)
shared BCG treatment backbone
Diarrhea
60% (144/241)
(Frequency)
For urinary frequency, rates of PRO-CTCAE
65% (159/246)
worsening were numerically higher with
Painful urination
83% (200/241)
D+BCG (80%) VS BCG (73%), with a
(Severity)
82% (201/246)
difference ≤10%
Urinary frequency
79% (127/160)
(Interference)
69% (125/181)
Urinary frequency
80% (193/241)
(Frequency)
73% (179/246)
0
20
40
60
80
100
Patients with any worsening (%)a
Data cutoff 03 April 2025 Patients with increased PRO CTCAE score during treatment/patients with baseline and at least 1 on treatment PRO CTCAE assessment BCG, bacillus Calmette-Guérin,
2026
ASCO
#ASCO26
D, durvalumab; I, induction, M. maintenance, PRO CTCAE, patient reported outcomes version of the Common Terminology Criteria for Adverse Events
ASCO
AMERICAN SOCIETY OF
CUNICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
[Slide 1]
POTOMAC: EORTC QLQ-C30 Change From Baseline
Adjusted mean changes from baseline showed modest deterioration in GHS/QoL and physical functioning and increased fatigue
in both treatment arms, with generally similar changes between treatment arms
2026ASCO
ANNUAL MEETING
GHS/QoL'
Physical Functioning
Fatigue
Difference between arms -27 (95% CL,-4,85 10-0.54)
Difference between arms -2.5 (95% CL -4.4310-0.81)
Difference between arms: 4.0 (95% CL 1.50 to 6.46)
2026 ASCO
#ASCO26
ASCO
ANNUAL MEETING
CONDUERS CANCER
---
[Slide 2]
POTOMAC: EORTC QLQ-NMIBC24 Change From Baseline
Adjusted mean change-from-baseline scores were not clinically meaningful and were similar between treatment arms
Urinary Symptoms
Intravesical Treatment Issues
Difference between ams for overall mean 1.2
Difference between ams for overal mean CFB-1.2(0% CL-3.79 1o1.29)
I
-
Future Perspective/Worries
Sexual Functioning
Difference between arms for overall mean CFB-22 (90% CL, -5.11 10 0.66)
Difference between am for overal mean CFB
-
Val.
I
Clarically meaningful change baseline
Data - Email tan Change for have - analyzed - - expeated - Toxpito - -
baseline
of
interactions
-
explanatory
I
I
with
taxine
the
analysis
defined
.
10-port
I
compand
with
I
below
Guara
CFS,
I
confidence
2026 ASCO
#ASCO26
Company Organisation I -
ASCO
ANNUAL MEETING
KNOWLEDGE CONQUERS
---
[Slide 3]
POTOMAC PRO-CTCAE Symptoms
PRO-CTCAE Symptom Worsening on Treatment Through Week 106
Abdominal pain
76% (39/51)
D+BCG (I+M)
(Interference)
68% (40/59)
BCG (I+M)
Across abdominal pain, diarrhea, and
Abdominal pain
67% (162/241)
painful urination, rates of PRO-CTCAE
(Frequency)
63% (156/246)
worsening were similar between treatment
Abdominal pain
59% (3051)
arms through Week 106, consistent with the
(Severity)
63% (37/59)
shared BCG treatment backbone
Diarrhea
60% (144/241)
For urinary frequency, rates of PRO-CTCAE
(Frequency)
65% (159/246)
worsening were numerically higher with
Painful urination
83% (200/241)
D+BCG (80%) VS BCG (73%), with a
(Severity)
82% (201/246)
difference <10%
Urinary frequency
79% (127/160)
(Interference)
69% (125/181)
Urinary frequency
80% (193/241)
(Frequency)
73% (179/246)
0
20
40
60
80
100
Patients with any worsening (%)*
Date - April with nonumed - during Insurrent/pations - BOG tacks -
2026 ASCO
#ASCO26
D. aduction, M. mankmance PRO-CTCAL patient autoomes - the Common lemecks or Advote Events
ASCO
ANNUAL MEETING
KNOWLEDGE CONQUERS CANCER
---
[Slide 4]
POTOMAC: Conclusions
At the planned 5-year OS analysis, the addition of durvalumab to
2026ASCO
BCG (I+M) continued to show no detriment to OS (HR 0.81; 95% CI,
ANNUAL MEETING
0.54-1.19)
from
the
The addition of durvalumab to BCG (I+M) did not have a major
Plan
impact on patient-reported quality of life, with generally similar PROs
between treatment arms
These data further support 1 year of durvalumab in combination with BCG induction and
maintenance as a new treatment for patients with BCG-naïve, high-risk NMIBC
1
De
M.
a
code
-
I
-
.
name
2026 ASCO
#ASCO26
patient
ASCO
ANNUAL MEETING
[Slide 1]
POTOMAC: Study Design
Durvalumab 1500 mg IV (Q4W X 13 cycles)
Primary endpoint
D+BCG (I+M)
BCG Maintenance
Study population
N=339
BCG Induction
DFS: D+BCG (I+M) vs BCG (I+M)
3 weekly doses at
Age ≥18 years
Weekly X 6 weeks
3m
6m
12m
18m
24m
NMIBC
Secondary endpoints
BCG-naive
5-year OS rate
High-risk tumor defined
Durvalumab 1500 mg IV (Q4W X 13 cycles)
(data cutoff 03 October 2025)
R
D+BCG
as any of the following:
Patient-reported outcomes
(1:1:1)
(I only)
T1
BCG Induction
N=1018
(data cutoff 03 April 2025)
N=339
High-grade/G3
Weekly X 6 weeks
CIS
Multiple and
recurrent and large
(>3 cm)
BCG (I+M)
BCG Maintenance
N=340
BCG Induction
3 weekly doses at
Weekly X 6 weeks
3m
6m
12m
18m
24m
Stratification factors:
First patient enrolled: June 2018
Higher-risk papillary disease (T1G3/T1 high-grade or multiple and recurrent and large tumors)
Last patient enrolled: October 2020
CIS
Last D dose: January 2022
Last BCG dose: January 2023
De Santis M, of al. Lancet 2025,406,2221-2234 All disease assessments were performed by the investigator For patients with persistent CIS disease at 3 months, a single BCG re-induction was administered
weekly for 6 weeks according to local standard practice BCG, bacillus Calmette-Guerin; CIS, carcinoma in situ; D, durvalumab; DFS, disease-free survival; G, grade; I, induction; IV, intravenous; m, month;
2026 ASCO
#ASCO26
M, maintenance; OS, overall survival; NMIBC, non-muscle-invasive bladder cancer, Q4W, every 4 weeks; R, randomization
ASCO
AMERICAN SOCIETY OF
CUMICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco. org.
KNOWLEDGE CONQUERS CANCER
---
[Slide 2]
POTOMAC: EORTC QLQ-C30 Change From Baseline
Adjusted mean changes from baseline showed modest deterioration in GHS/QoL and physical functioning and increased fatigue
in both treatment arms, with generally similar changes between treatment arms
GHS/QoL1
Physical Functioning
Fatigue
Difference between arms: -2.7 (95% CI, -4.85 to -0.54)
Difference between arms: -2.6 (95% CI, -4.43 to -0.81)
Difference between arms: 4.0 (95% CI, 1.50 to 6.46)
20
20
20
Adjusted mean change
10
Better
from baseline
-10
Adjusted mean change
10
Better
0
from baseline
Adjusted mean change
10
0
Worse
from baseline
Worse
0
Worse
-10
-10
Botter
-20
-20
-20
2 10 18 26 34 42 50 58 66 74 82 90 98 106114122130138146
2 10 18 26 34 42 50 58 66 74 82 90 98 106114122130138146
2 10 18 26 34 42 50 58 66 74 82 90 98 106114122130138146
Visit (weeks)
Visit (weeks)
Visit (weeks)
No. of patients in analysis
No of patients in analysis
No. of patients in analysis
D+BCQ (1+88)214 189 180 177 174 171 156 149 142 148 138 138 130 126 122 117 104 105
D+BCG (1+81)214 202 189 180 177 174 171 156 149 142 148 138 138 130 126 122 117 104 105
D+BCG (I+M)214 202 189 180 177 174 171 156 149 142 148 138 138 130 126 122 117 104 105
BCG (+M)232 213 192 193 178 183 158 165 165 158 149 152 138 139 133 120 124 123
BCG (1+18)232 219 213 192 193 178 183 158 165 165 158 149 152 138 139 133 120 124 123
BCQ (1+M) 219 213 192 193 178 183 158 165 165 158 149 152 138 139 133 120 124 123
Clinically meaningful change from baseline
1. De Santis M, of al. Lancet 2025,406,2221-2234 Data cutoff 03 April 2025 Decreases indicate worsening for GHS/QoL and physical functioning: increases indicate worsening for fatigue. Error bara show 95%
CI. Change from baseline was analyzed using a mixed model for repeated measures and heterogenous Toeplitz, with stratification factors, treatment, visit, baseline score, treatment-by-visit and baseline score-
by-visit interactions as explanatory variables. Only patients with an evaluable baseline score and at least 1 evaluable postbaseline score are included in the analysis model A clinically meaningful change was
defined as a 10-point change in score compared with baseline. BCG, bacillus Calmette-Guérin, CFB, change from baseline; CL, confidence interval; D, durvalumab; EORTC QLQ-C30, European Organisation for
2026 ASCO
Research and Treatment of Cancer 30-item core quality of life questionnaire; GHS/QoL. global health scale/quality of life; I, induction; M, maintenance
#ASCO26
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 3]
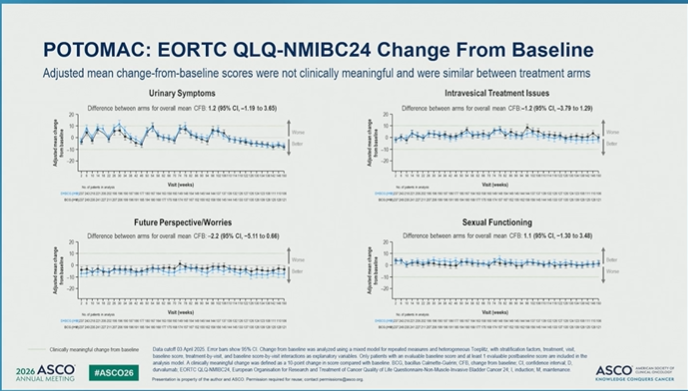
POTOMAC: EORTC QLQ-NMIBC24 Change From Baseline
Adjusted mean change-from-baseline scores were not clinically meaningful and were similar between treatment arms
Urinary Symptoms
Intravesical Treatment Issues
Difference between arms for overall mean CFB:1.2 (95% CI,-1.19 to 3.65)
Difference between arms for overall mean CFB:-1.2 (95% CI, -3.79 to 1.29)
20
20
10
10
Adjusted mean change
Worse
from baseline
0
Beter
Adjusted mean change
Worse
from baseline
0
Better
-10
-10
-20
-20
10
14
18
22
21
#
|
M
30
42
41
30
54
-
42
"
70
N
78
82
N
to
#
102
126112
14
122
5
130
134
138142
45
100
:
10
14
18
22
26
30
H
42
54
14
42
06
79
74
78
#2
-
90
94
-
192
106110
114
14
(26
(30
42
100
Visit (weeks)
in pateris analysis
No - analysis
Visit (weeks)
program
196
190
177
180
62
IS4
153
ISS
190
145
148
134
143
$45144
144
or
-
132
25
127
126
124
100
243
221
195
-
-
149
148
-
1
in
(21
200
241
Future Perspective/Worries
Sexual Functioning
Difference between arms for overall mean CFB:-2.2 (95% CI, -5.11 to 0.66)
Difference between arms for overall mean CFB: 1.1 (95% CI, -1.30 to 3.48)
20
20
10
10
Adjusted mean change
Worse
from baseline
10
Adjusted mean change
from baseline
Beter
0
0
Better
Worse
-10
-20
-20
14
"
25
30
34
#
42
48
so
$4
-
u
"
to
N
76
#
"
N
M
16
102
105
10
=
122
129
130
134
138142
145
150
2
10
14
18
22
25
30
24
a
42
44
to
$4
sa
=
"
N
78
"
#
90
M
"
102
105
114
118
122
125
130
134
138142
145
Visit (weeks)
to - analysis
No - analysis
Visit (weeks)
pregar
F96
180
107
154
10
154
160
149
148
154
43
E
137
(27
129
122
127
FOR
195
190
177
160
167
164
158
560
135
BCG
Clinically meaningful change from baseline
Data cutoff 03 April 2025 Error bars show 95% CI Change from baseline was analyzed using mixed model for repeated measures and heterogeneous Toeplitz, with stratification factors, treatment, visit,
baseline score, treatment by visit, and baseline score by visit interactions as explanatory variables. Only patients with an evaluable baseline score and at least 1 evaluable postbaseline score are included in the
analysis model A clinically meaningful change was defined as a 10 point change in score compared with baseline BCG, bacillus Calmette-Guérin; CFB, change from baseline; CI, confidence interval; 0,
2026 ASCO
#ASCO26
durvalumab; EORTC QLQ-NMIBC24, European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-Non-Muscle-Invasive Bladder Cancer 24; I, induction; M, maintenance
ASCO
AMERICAN SOCIETY or
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org.
KNOWLEDGE CONQUERS CANCER
---
[Slide 4]
Key Takeaway Points
In the POTOMAC study, the addition of durvalumab to
BCG (I+M) continued to show no OS detriment at the
planned 5-year OS analysis
Durvalumab in combination with BCG (I+M) did not have a
major impact on patient-reported quality of life
2026 ASCO
BCG, Bacillus Calmette-Guerin I, induction; M, maintenance OS, overall survival.
#ASCO26
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse; contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
[Slide 1]
POTOMAC: Study Design
Durvalumab 1500 mg IV (Q4W . 13 cycles)
Study population
D+BCG (I+M)
BCG Maintenance
N=339
BCG Induction
Age 2 18 years
3 weekly doses at
Weekly * 6 weeks
NMIBC
3m
6m
12m
18m
24m
BCG-naive
High-risk tumor
Durvalumab 1500 mg IV (Q4W - 13
defined as any of
R
D+BCG
cycles)
the following:
(1:1/1)
(I only)
N=1018
BCG Induction
T1
N=339
Weekly * 6 weeks
High-grade/G3
CIS
Multiple and
recurrent and
BCG (I+M)
BCG Maintenance
large (23 cm)
N=340
BCG Induction
3 weekly doses at
Weekly * 6 weeks
3m
6m
12m
18m
24m
Stratification factors:
.
Postio
Higher-risk papillary disease (T1G3/T1 high-grade or multiple and recurrent and
---
[Slide 2]
POTOMAC: EORTC QLQ-C30 Change From Baseline
Adjusted mean changes from baseline showed modest deterioration in GHS/QoL and physical functioning and increased fatigue
in both treatment arms, with small differences between treatment arms
GHS/QoL'
Physical Functioning
Fatigue
D+BCG (1+M) -76 (95% CI, -9.19 to -6.07)
D+BCG (I+M): -5.5 (95% CL -6.76 to -4.15)
D+BCG (I+M): 10.1 (95% CI, 8.32 32 to 11.90)
BCG (I+M): -4.9 (95% CI, -6.46 to -3.41)
BCG (1+M): -28 (95% CL -4.11 -4.11to-1.56)
BCG (I+M): 6.1 (95% CI, 4.37 to 7.88)
Difference between arms: -2.7 (95% CI, -4.85 to -0.54)
Difference between arms: =2.6 (95% CI, -4.43 to -0.81)
Difference between arms: 4.0 (95% CL 1.50 to 6.46)
20
20
20
Address change I
St
I I
Befor
Adjusted I I
2
Deber
-10
-10
licre
I I I
10
Work
D
0
Worse
I
benefine 1
0
-10
Better
-20
&
8
2
10
18
X
34
42
56
56
74
12
90
M
2
NO
14
X
34
42
50
58
66
74
12
to
2
10
.
28
34
42
50
50
56
T4
82
XI
Visit [weeks]
Visit (weeks)
Valt [weeks]
No of justerns . anarysis
No or patients if anarysis
No. if (satents if anarysis
Cirically meaninglu change from baseline
---
[Slide 3]
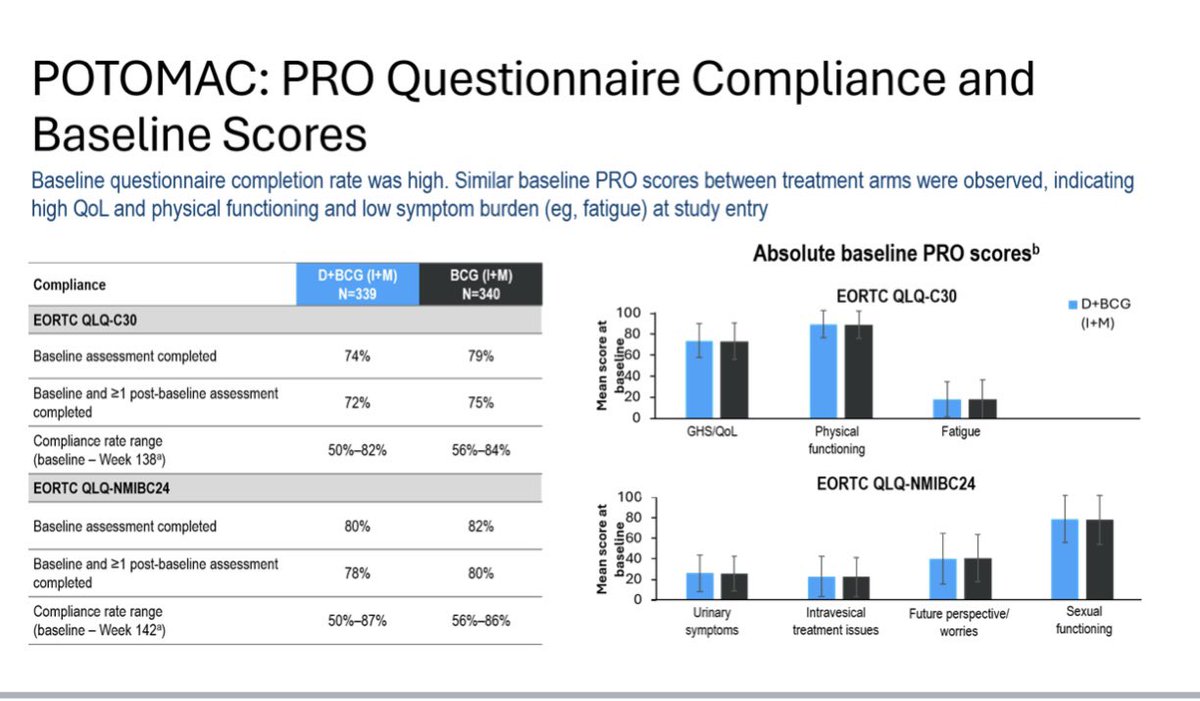
POTOMAC: PRO Questionnaire Compliance and
Baseline Scores
Baseline questionnaire completion rate was high. Similar baseline PRO scores between treatment arms were observed, indicating
high QoL and physical functioning and low symptom burden (eg, fatigue) at study entry
Absolute baseline PRO scoresᵇ
D+BCG (I+M)
BCG (I+M)
Compliance
N=339
N=340
EORTC QLQ-C30
D+BCG
100
EORTC QLQ-C30
(I+M)
80
Baseline assessment completed
74%
79%
Mean score at
baseline
60
40
Baseline and >1 post-baseline assessment
72%
75%
20
completed
0
GHS/QoL
Physical
Fatigue
Compliance rate range
50%-82%
56%-84%
functioning
(baseline - Week 138ᵃ)
EORTC QLQ-NMIBC24
EORTC QLQ-NMIBC24
100
80
Baseline assessment completed
80%
82%
Baseline and >1 post-baseline assessment
78%
80%
Mean score at
baseline
60
40
completed
20
0
Compliance rate range
50%-87%
Urinary
Intravesical
Future perspective/
Sexual
56%-86%
(baseline - Week 142ᵃ)
symptoms
treatment issues
worries
functioning
---
[Slide 4]
Frequency of toxicity with adjuvant immune checkpoint
inhibition in RCC according to patient defined framework
LC
Adjuvant immune therapy
Life changing
Frequency of patient-defined categories
SLT
in IMmotion010 atezolizumab arm (n=262)
Endocrine
Significant long term
LC
Adrenal insufficiency/Hypophysitis
12%
Insulin dependent diabetes
Rheumatological
Chronic toxicity requiring
-
≥3 Arthritis/Myositis/Vasculitis
SLT
Steroids
Cardiopulmonary
NS
22%
- Admission to hospital
-
≥3 Pneumonitis/Myo/Pericarditis
54%
- Treatment discontinuation
Neurological
- "Hypothyroidism
Meningoencephalitis
SST
-
Demyelinating syndromes/NMJ disorders
12%
LC
5%
SLT
NS
10%
SST
Non-significant
Placebo/Follow up
SST
Significant short term
Frequency of patient-
10%
defined categories in
Asymptomatic blood abnormalities
NS
Acute toxicity requiring steroids /
Grade 1 AEs
IMmotion010 placebo arm
75%
hospital admission / treatment
Infusion related reactions
(n=274)
discontinuation
6
Elizabeth Nally
[Slide 1]
POTOMAC: 5-Year Overall Survival - ITT
No detriment at the 5-year OS analysis was observed with the addition of durvalumab to BCG (I+M) therapy
D+BCG (I+M)
BCG (I+M)
N=339
N=340
Deaths, n (%)
45 (13)
56 (16)
Median OS
NR
NR
1.0
88%
(95% CI), months
(NR-NR)
(NR-NR)
0.8
86%
Probability of os
0.6
0.4
HR 0.81 (95% CI, 0.54-1.19)
0.2
Median follow-up: 72 months
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
51
54
57
60
63
66
69
72
75
78
81
84
87
90
Time from randomization (months)
No. of patients at risk
D+BCG (I+M) 339 336 329 326 324 320 319 315 314 311 306 303 298 296 293 290 290 286 283 277 270 236 217 182 141 115 73 30 11 1 0
BCG (I+M) 340 338 336 333 330 328 326 322 317 313 313 313 309 305 301 295 292 288 284 281 275 239 220 185 140 108 70 32 12 0 0
in censored patients across treatment arms. Data cutoff 03 October 2025. OS is the time from randomization until death due to any cause regardless of whether the patient withdraws from randomized therapy or
receives another anti cancer therapy. BCG, bacillus Calmette Guérin; CI, confidence interval; D. durvalumab; HR, hazard ratio; I, induction; ITT, intent to treat population; M, maintenance: NR, not reached; OS,
ASCO
overall survival
#ASCO26
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
UAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org.
KNOWLEDGE CONQUERS CANCER
---
[Slide 2]
POTOMAC PRO-CTCAE Symptoms
PRO-CTCAE Symptom Worsening on Treatment Through Week 106
Abdominal pain
76% (39/51)
D+BCG (I+M)
(Interference)
68% (40/59)
BCG (I+M)
Across abdominal pain, diarrhea, and
Abdominal pain
67% (162/241)
painful urination, rates of PRO-CTCAE
(Frequency)
63% (156/246)
worsening were similar between treatment
Abdomenal pain
59% (30/51)
arms through Week 106, consistent with the
(Seventy)
63% (37/59)
shared BCG treatment backbone
Diarrhea
60% (144/241)
(Frequency)
For urinary frequency, rates of PRO-CTCAE
65% (159/246)
worsening were numerically higher with
Painful unnation
83% (200/241)
D+BCG (80%) VS BCG (73%), with a
(Seventy)
82% (201/246)
difference <10%
Uninary frequency
79% (127/160)
(Interference)
69% (125/181)
Urinary frequency
80% (193/241)
(Frequency)
73% (179/246)
0
20
40
60
80
100
Patients with any worsening (%)*
Date cutcult 00 April 2025 Patents - remained PRO CTCAE soom during breatment/patents with baseficiar and if less 1 on bestment PRO-CTCAL - BCG, backs Calmette Code
ASCO
#ASCO26
D. L induction M, maintenance, PRO-CTCAL patient reported culcomer - of the Common Terminary Orderia for Adverse Events
ASCO
AMERICAN accept of
-
AL MEETING
Presentation . property of the author and ASCO. Permission - lest - - any
KNOWLEDGE CONQUERS CANCER
---
[Slide 3]
POTOMAC: EORTC QLQ-NMIBC24 Change From Baseline
Adjusted mean change-from-baseline scores were not clinically meaningful and were similar between treatment arms
Urinary Symptoms
Intravesical Treatment Issues
Difference between - for overall mean CFB: 1.2 (95% CL-1.19 to 3.65)
Difference between ams for overal mean CFB:-1.2(85% CL-3.79 to 1.29)
20
20
10
12
1 I I
mm
Internal
change I
None
0
0
I
Ester
-10
I
50
-20
-29
.
-
Valt (weeks)
Visit (weeks)
!
!
-
Future Perspective/Worries
Sexual Functioning
Difference behween - for overall mean CFB:-22 (95% CL, -5.11 to 0.00)
Difference between anns for overall mean CFB: 1.1 (95% CL-1.30 to 3.45)
20
20
10
10
I I
None
I I
H
butter
0
0
Dellar
Flose
10
-13
-20
-20
&
I
Vall (weeks)
Vall (weeks)
Clearally mesningful change from Landing
Data culcul 03 April 25 Enter tars the 05% a Charge from Laneline was analyzed ving nued model for repeated I and helerogeneous Fooplitz with institution before, Instruction visit,
buseless acces, treatment by - and baseline sours by - interactions as explaratory variables Only patients with an evaluable baselee - and at less - - are included b the
analysis model A clinically meaninght change - defined - . 10-point change # address companed with baseline BCO. beciefus Committe-Outrin CFB, change - beseles, a confidence interval D,
ASCO
durvaluments EGRTC QLQ-NMIBC24 European Organisation by Research and Testment of Cancer Quality of Life Quantionnaire Non Invoice Baker Cancer 24 L induction M markssance
ASCO
INFECTS
-
#ASCO26
AL MEETING
Presentation . possents of the who and ASCO - required for - -
ENOWLEDGE COMQUERS
---
[Slide 4]
POTOMAC: EORTC QLQ-C30 Change From Baseline
Adjusted mean changes from baseline showed modest deterioration in GHS/QoL and physical functioning and increased fatigue
in both treatment arms, with generally similar changes between treatment arms
GHS/QoL1
Physical Functioning
Fatigue
Difference between arms: -2.7 (95% CI, -4.85 to -0.54)
Difference between arms: -2.6 (95% CI, -4.43 to -0.81)
Difference between arms: 4.0 (95% CI, 1.50 to 6.46)
20
20
20
Adjusted mean change
10
from baseline
Better
Adjusted mean change
10
from baseline
Better
Worse
Worse
Adjusted mean change
10
0
from baseline
Worse
0
0
10
-10
-10
Better
-20
-20
-20
2 10 18 26 34 42 50 58 66 74 82 90 98 106114122130138146
2 10 18 26 34 42 50 58 66 74 82 90 98 106114122130138146
2 10 18 26 34 42 50 58 66 74 82 90 98 106114122130138146
Visit (weeks)
Visit (weeks)
Visit (weeks)
No. of patients in analysis
No of patients in analysis
No. of patients in analysis
D+BCG (1+11)214 189 180 177 174 171 156 149 142 148 138 138 130 126 122 117 104 105
D+BCG (1+M): 202 189 180 177 174 171 156 149 142 148 138 138 130 126 122 117 104 105
D+BCG (1+M) 202 189 180 177 174 171 156 149 142 148 138 138 130 126 122 117 104 105
BCG (1+M)232 219 213 192 193 178 183 158 165 165 158 149 152 138 139 133 120 124 123
BCG (I+M) 219 213 192 193 178 183 158 165 165 158 149 152 138 139 133 120 124 123
BCQ (1+M)232 219 213 192 193 178 183 158 165 165 158 149 152 138 139 133 120 124 123
Clinically meaningful change from baseline
1. De Santis M, of al. Lancet 2025,406,2221-2234 Data cutoff 03 April 2025. Decreases indicate worsening for GHS/QoL and physical functioning: increases indicate worsening for fatigue. Error bars show 95%
CI. Change from baseline was analyzed using a mixed model for repeated measures and heterogenous Toeplitz, with stratification factors, treatment, visit, baseline score, treatment-by-visit and baseline score-
by-visit interactions as explanatory variables. Only patients with an evaluable baseline score and at least 1 evaluable postbaseline score are included in the analysis model. A clinically meaningful change was
defined as a 10-point change in score compared with baseline. BCG, bacillus Calmette-Guerin CFB, change from baseline; CI, confidence interval; D, durvalumab; EORTC QLQ-C30, European Organisation for
ASCO
Research and Treatment of Cancer 30-item core quality of life questionnaire; GHS/QoL. global health scale/quality of life; 1, induction, M, maintenance.
ASCO
AMERICAN SOCIETY OF
#ASCO26
CUNICAL ONCOLOGY
AL MEETING
Presentation is property of the author and ASCO Permission required for reuse; contact permissions@asco.or
KNOWLEDGE CONQUERS CANCER
[Slide 1]
POTOMAC: 5-Year Overall Survival - ITT
No detriment at the 5-year OS analysis was observed with the addition of durvalumab to BCG (I+M) therapy
D+BCG (I+M)
BCG (I+M)
N=339
N=340
Deaths, (%)
45 (13)
56 (16)
Median OS
NR
NR
1.0
88%
(95% CI), months
(NR-NR)
(NR-NR)
0.8
86%
Probability of OS
0.6
0.4
HR 0.81 (95% CI, 0.54-1.19)
0.2
Median follow-up: 72 months
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
51
54
57
60
63
66
69
72
75
78
81
84
87
90
Time from randomization (months)
No. of patients at risk
D+BCG (I+M) 339 336 329 326 324 320 319 315 314 311 306 303 298 296 293 290 290 286 283 277 270 236 217 182 141 115 73 30 11 1 0
BCG (I+M) 340 338 336 333 330 328 326 322 317 313 313 313 309 305 301 295 292 288 284 281 275 239 220 185 140 108 70 32 12 0 0
% consored patients across treatment arms. Data outoff 03 October 2025 os 0 the time from randomization until death due to any cause regardless of whether the patient withdraws from randomized therapy or
26 ASCO
#ASCO26
overall survival
receives another and cancer therapy BCG, bacillus Calmette Gudrin CI, confidence interval; 0. durvalumab; HR, hazard ratio, induction; ITT. intent to treat population; M, maintenance NR, not reached 08,
NUAL MEETING
Presentation N property of the author and ASCO Permission required for - contact permissione@asco.org org.
ASCO
AMERICAN SOCE
CUPICAL OHCOU
KHOWLEDGE CONQUERS - CAN
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
SCO
ASCO
ASCO
ASCO
ASCC
ASCO
D
ASCO
O
ASCO
ASC
ASCO
---
[Slide 2]
POTOMAC: PRO Questionnaire Compliance and Baseline Scores
Baseline questionnaire completion rate was high. Baseline PRO scores were similar between treatment arms and indicated high QoL
and physical functioning and low symptom burden (e.g., fatigue) at study entry
Absolute baseline PRO scoresᵇ
Compliance
D+BCG (I+M)
BCG (I+M)
EORTC QLQ-C30
D+BCG (I+M)
№339
N=340
100
BCG (I+M)
Mean score at baseline
80
High
EORTC QLQ-C30
functioning
60
High
GHS/Got
Baseline assessment completed
74%
79%
40
Low
20
Baseline and 21 post-baseline
symptom
72%
75%
burden
assessment completed
0
GHS/QoL
Physical
Fatigue
Compliance rate range
functioning
50%-82%
56%-84%
(baseline - Week 138*)
EORTC QLQ-NMIBC24
EORTC QLQ-NMIBC24
100
Baseline assessment completed
80%
82%
Baseline and 21 post-baseline
78%
Mean score at baseline
80
High
60
functioning
40
80%
Low
Low
assessment completed
20
Low
symptom
symptom
symptom
burden
burden
burden
Compliance rate range
0
50%-87%
56%-86%
Urinary
Intravesical treatment
(baseline - Week 142°)
Future perspective/ wornes
Sexual functioning
symptoms
issues
Data a 03 April 2025 Compliance range refects the lowest and highest - level compliance from bassine through Week 138 or Week 142 For GHS/QoL and functioning scales, higher scores indicate
better Gol. and function For symptom ocales, higher scores indicate greater symptom burden, BCG bacillus Calmette Cubrin 0. durvalumab EORTC CI.Q-C30 European Organisation for Research and
Treatment of Cancer form core quality of Me questionnaire, EORTC Q NMBC24 European Organisation for Research and Treatment of Cancer Quality of Questionnaire Non Muscle invoive Bladder
2026 ASCO
#ASCO26
Cancer 24, GHS/QL poblic health acare/quality of the HRQX health-related quality of life, L induction M maintenance, PRO patient reported outcome, Onl, quality of the
ASCO
AMERICAN
DURICAL -
ANNUAL MEETING
property of the author and ASCO Permission required for - contact permissions@ascs.org
KHOWLEDGE CONQUERS CANCER
ASCO
ASCO
ASCO
ASCO
ASCO
A!
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
ASCO
A
ASCO
SCO
ASCO
SCO
ASCO
AS
ASCO
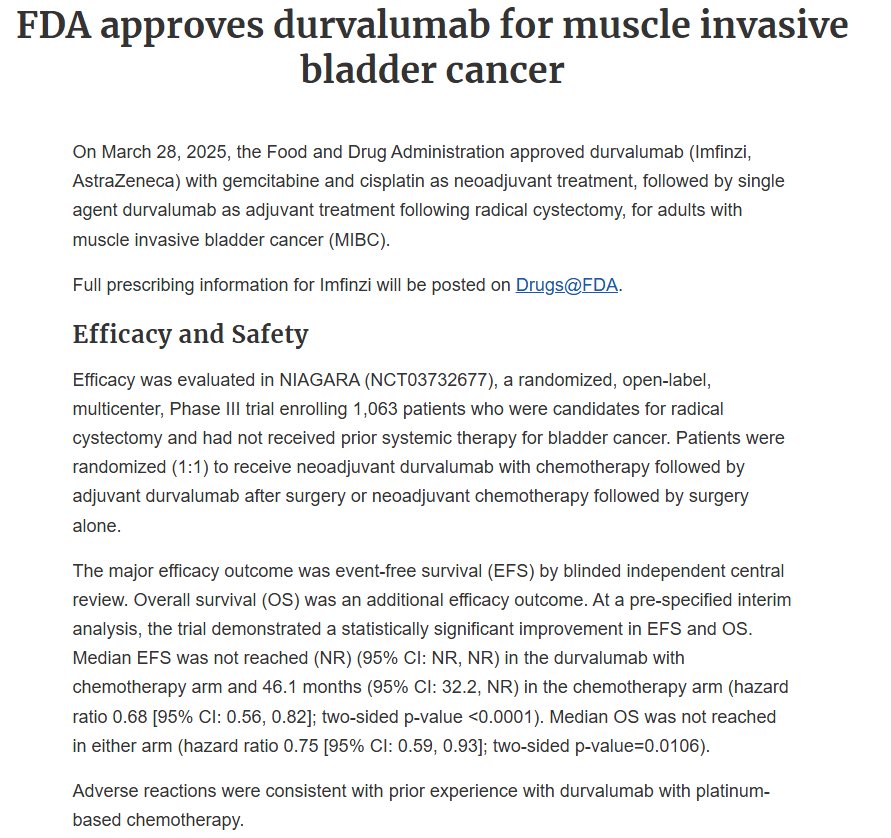
FDA approves durvalumab for muscle invasive
bladder cancer
On March 28, 2025, the Food and Drug Administration approved durvalumab (Imfinzi,
AstraZeneca) with gemcitabine and cisplatin as neoadjuvant treatment, followed by single
agent durvalumab as adjuvant treatment following radical cystectomy, for adults with
muscle invasive bladder cancer (MIBC).
Full prescribing information for Imfinzi will be posted on Drugs@FDA.
Efficacy and Safety
Efficacy was evaluated in NIAGARA (NCT03732677), a randomized, open-label,
multicenter, Phase III trial enrolling 1,063 patients who were candidates for radical
cystectomy and had not received prior systemic therapy for bladder cancer. Patients were
randomized (1:1) to receive neoadjuvant durvalumab with chemotherapy followed by
adjuvant durvalumab after surgery or neoadjuvant chemotherapy followed by surgery
alone.
The major efficacy outcome was event-free survival (EFS) by blinded independent central
review. Overall survival (OS) was an additional efficacy outcome. At a pre-specified interim
analysis, the trial demonstrated a statistically significant improvement in EFS and OS.
Median EFS was not reached (NR) (95% CI: NR, NR) in the durvalumab with
chemotherapy arm and 46.1 months (95% CI: 32.2, NR) in the chemotherapy arm (hazard
ratio 0.68 [95% CI: 0.56, 0.82]; two-sided p-value <0.0001). Median OS was not reached
in either arm (hazard ratio 0.75 [95% CI: 0.59, 0.93]; two-sided p-value=0.0106).
Adverse reactions were consistent with prior experience with durvalumab with platinum-
based chemotherapy.
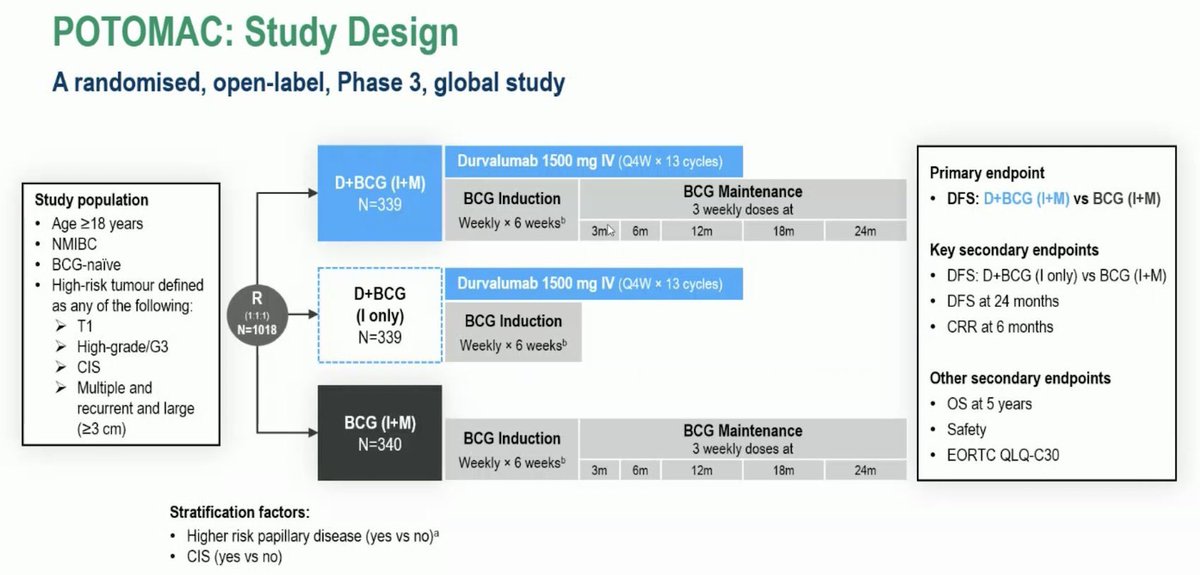
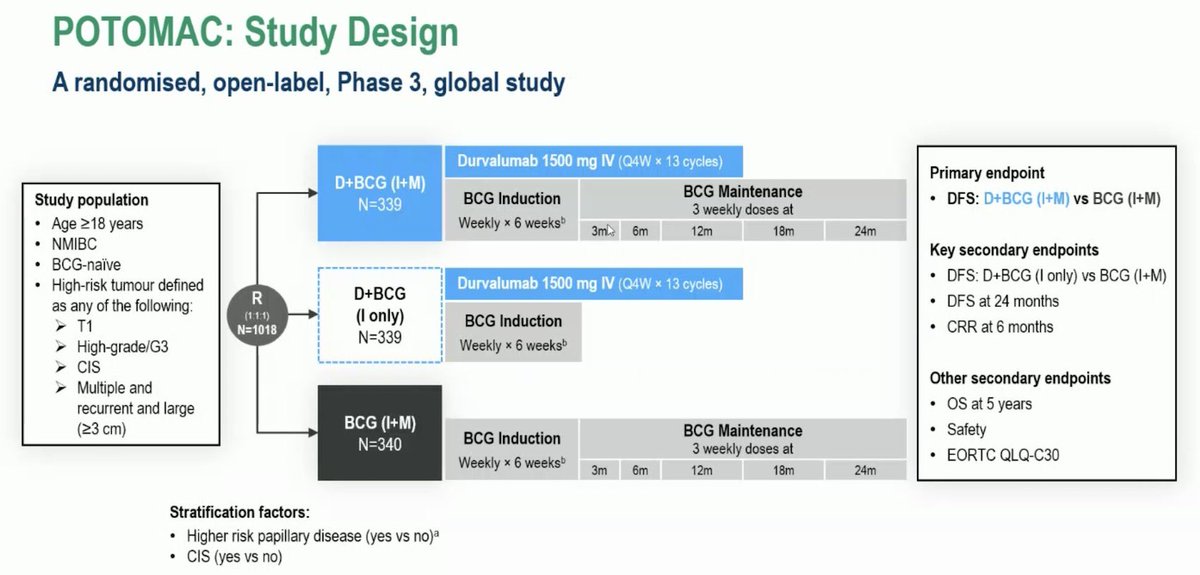
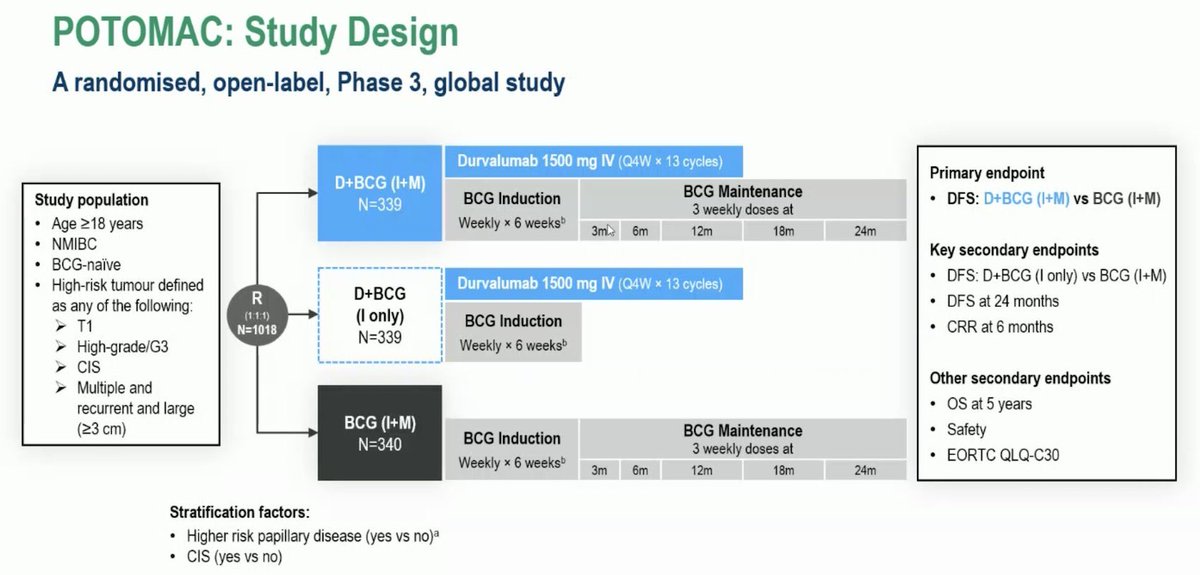
POTOMAC: Study Design
A randomised, open-label, Phase 3, global study
Durvalumab 1500 mg IV (Q4W X 13 cycles)
Primary endpoint
D+BCG (I+M)
BCG Induction
BCG Maintenance
Study population
N=339
DFS: D+BCG (I+M) vs BCG (I+M)
3 weekly doses at
Age ≥18 years
Weekly x 6 weeks
3ml
6m
12m
18m
24m
NMIBC
Key secondary endpoints
BCG-naive
High-risk tumour defined
Durvalumab 1500 mg IV (Q4W X 13 cycles)
DFS: D+BCG (I only) VS BCG (I+M)
as any of the following:
R
D+BCG
DFS at 24 months
(1:1:1)
T1
(I only)
BCG Induction
N=1018
CRR at 6 months
N=339
High-grade/G3
Weekly X 6 weeksb
CIS
Other secondary endpoints
Multiple and
recurrent and large
OS at 5 years
(≥3 cm)
BCG (I+M)
N=340
BCG Induction
BCG Maintenance
Safety
3 weekly doses at
EORTC QLQ-C30
Weekly x 6 weeks
3m
6m
12m
18m
24m
Stratification factors:
Higher risk papillary disease (yes VS no)a
CIS (yes VS no)
---
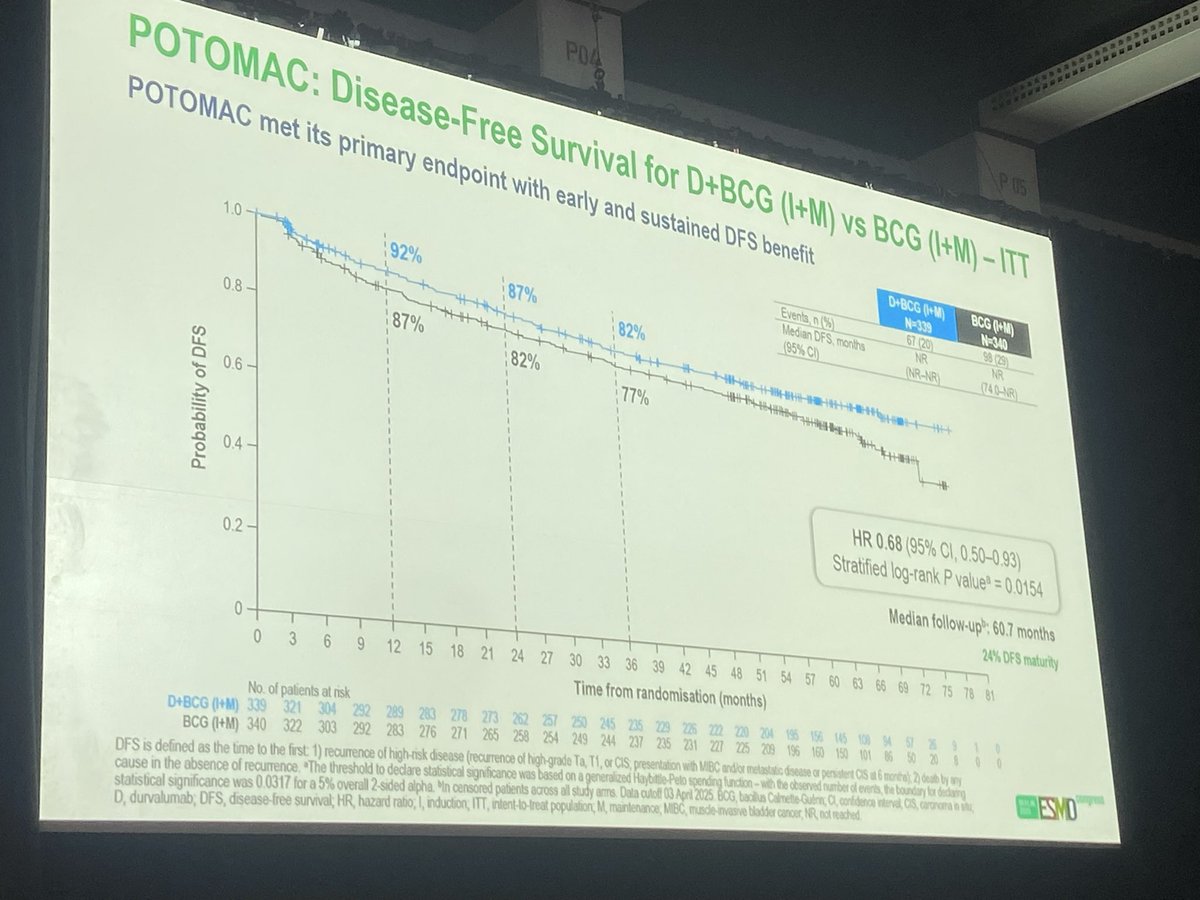
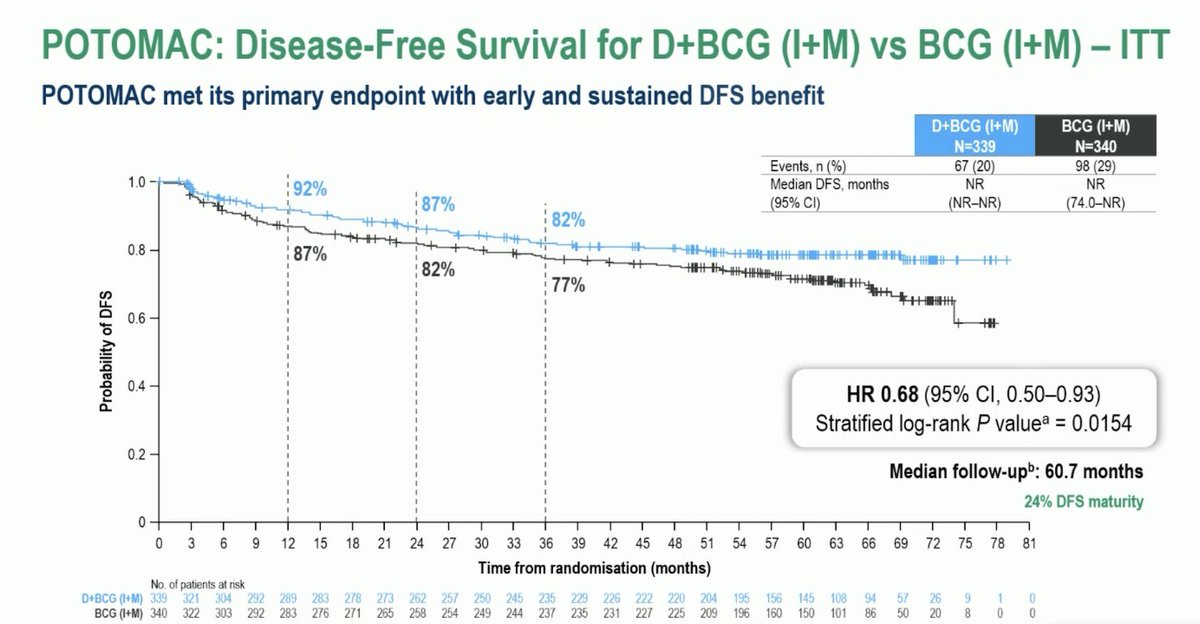
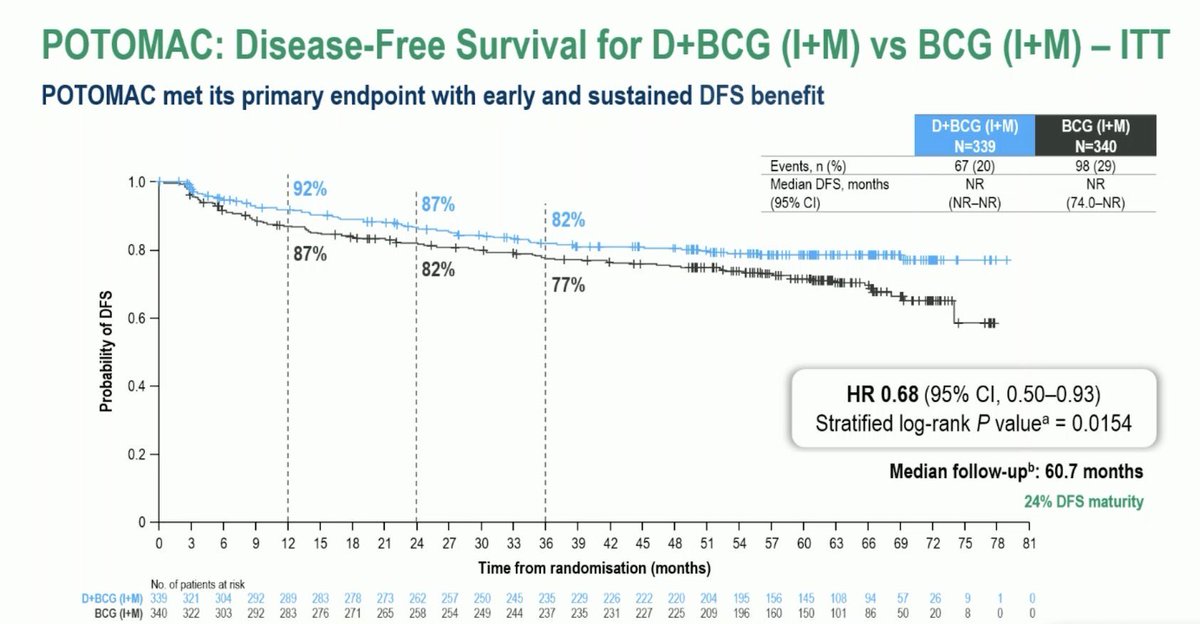
POTOMAC: Disease-Free Survival for D+BCG (I+M) vs BCG (I+M) - ITT
POTOMAC met its primary endpoint with early and sustained DFS benefit
D+BCG (I+M)
BCG (I+M)
N=339
N=340
Events, n (%)
67 (20)
98 (29)
1.0
92%
Median DFS, months
NR
NR
87%
(95% CI)
(NR-NR)
(74.0-NR)
82%
0.8
87%
82%
77%
Probability of DFS
0.6
+
0.4
HR 0.68 (95% CI, 0.50-0.93)
Stratified log-rank P value = 0.0154
0.2
Median follow-upb: 60.7 months
24% DFS maturity
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
51
54
57
60
63
66
69
72
75
78
81
Time from randomisation (months)
No of patients at risk
D+BCG (I+M)
339
321
304
292
289
283
278
273
262
257
250
245
235
229
226
222
220
204
195
156
145
108
94
57
26
9
1
0
BCG (I+M)
340
322
303
292
283
276
271
265
258
254
249
244
237
235
231
227
225
209
196
160
150
101
86
50
20
8
0
0
---
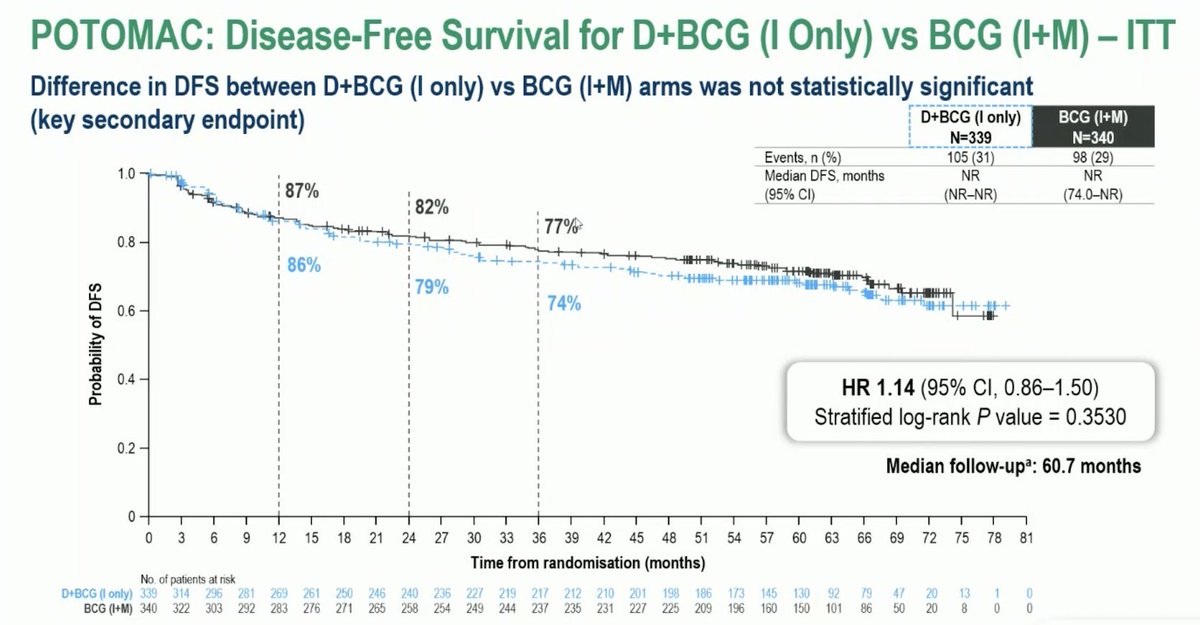
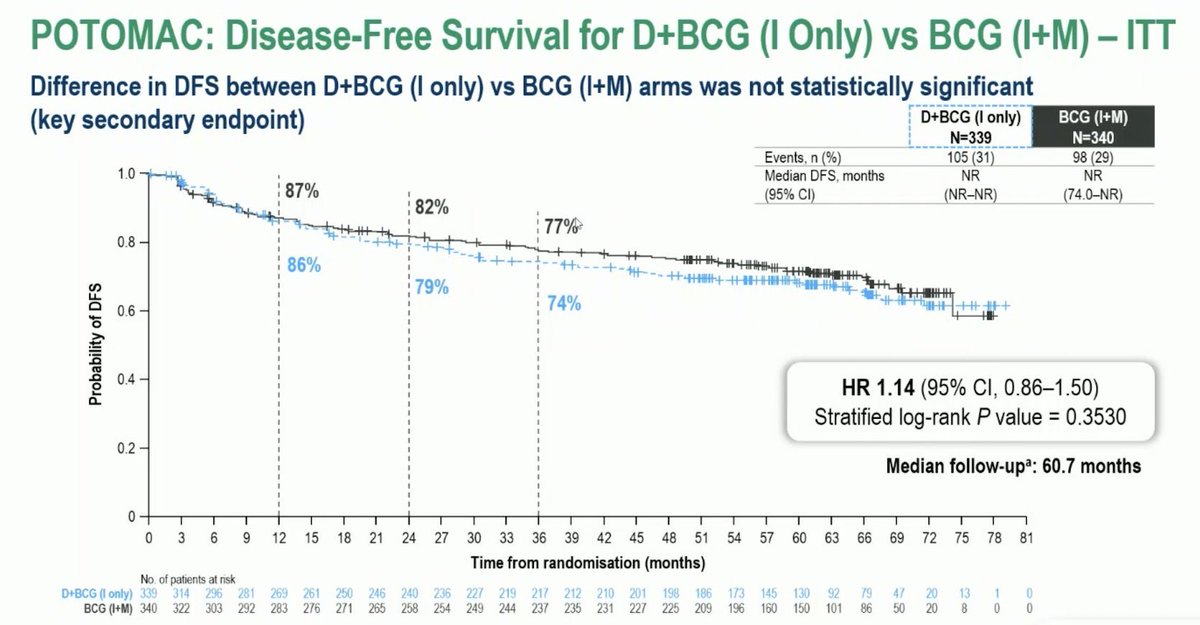
POTOMAC: Disease-Free Survival for D+BCG (I Only) vs BCG (I+M) - ITT
Difference in DFS between D+BCG (I only) vs BCG (I+M) arms was not statistically significant
(key secondary endpoint)
D+BCG (I only)
BCG (I+M)
N=339
N=340
Events, n (%)
105 (31)
98 (29)
1.0
Median DFS, months
NR
NR
87%
(95% CI)
(NR-NR)
(74.0-NR)
82%
77%
0.8
86%
79%
74%
Probability of DFS
0.6
0.4
HR 1.14 (95% CI, 0.86-1.50)
Stratified log-rank P value = 0.3530
0.2
Median follow-upᵃ: 60.7 months
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
51
54
57
60
63
66
69
72
75
78
81
Time from randomisation (months)
No of patients at risk
D+BCG (I only)
339
314
296
281
269
261
250
246
240
236
227
219
217
212
210
201
198
186
173
145
130
92
79
47
20
13
1
0
BCG (I+M)
340
322
303
292
283
276
271
265
258
254
249
244
237
235
231
227
225
209
196
160
150
101
86
50
20
8
0
0
---
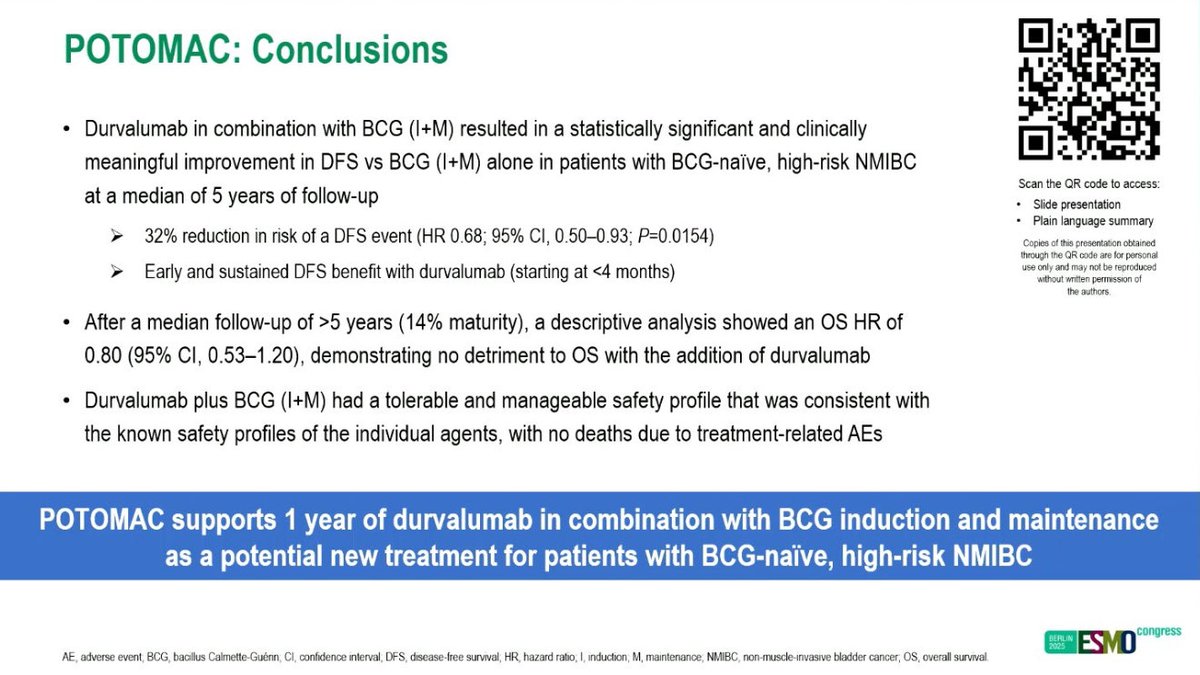
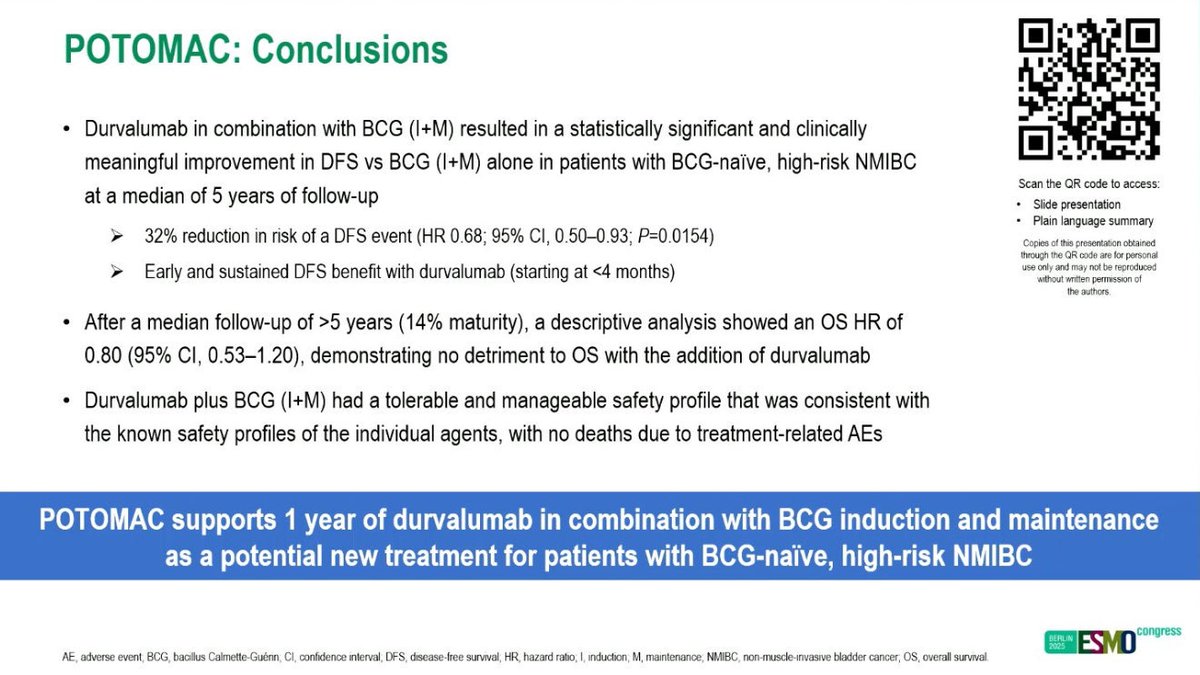
POTOMAC: Conclusions
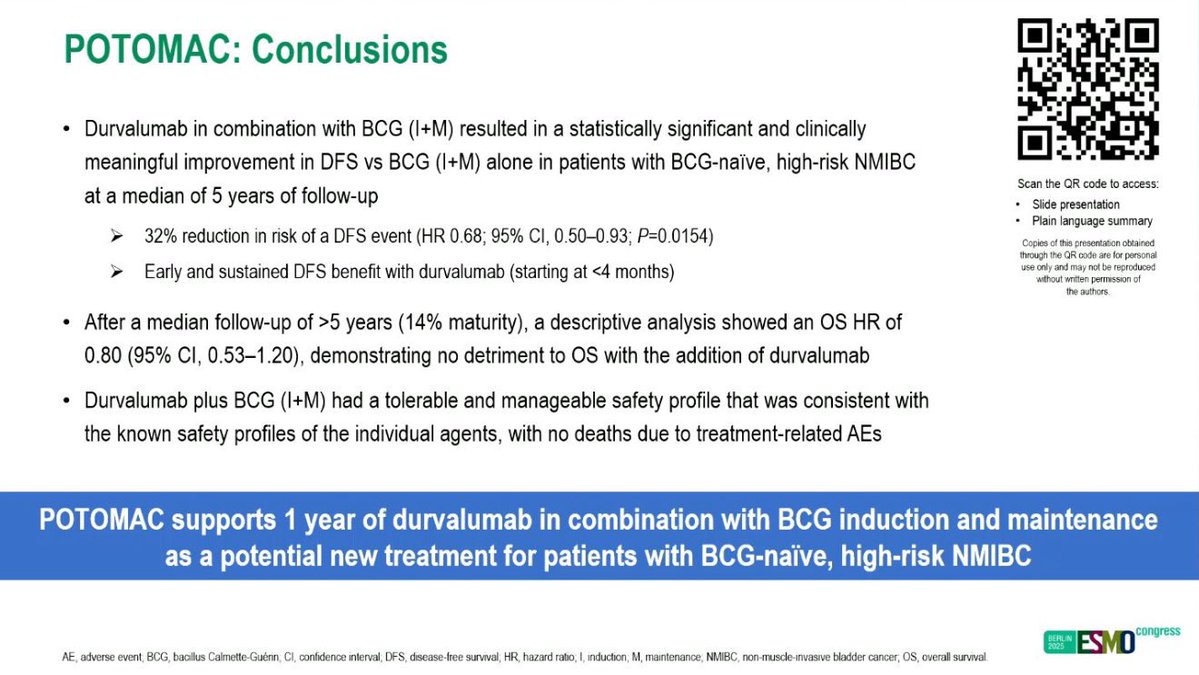
Durvalumab in combination with BCG (I+M) resulted in a statistically significant and clinically
meaningful improvement in DFS VS BCG (I+M) alone in patients with BCG-naïve, high-risk NMIBC
Scan the QR code to access:
at a median of 5 years of follow-up
Slide presentation
Plain language summary
32% reduction in risk of a DFS event (HR 0.68; 95% CI, 0.50-0.93; P=0.0154)
Copies of this presentation obtained
through the QR code are for personal
Early and sustained DFS benefit with durvalumab (starting at <4 months)
use only and may not be reproduced
without written permission of
the authors
After a median follow-up of >5 years (14% maturity), a descriptive analysis showed an OS HR of
0.80 (95% CI, 0.53-1.20), demonstrating no detriment to OS with the addition of durvalumab
Durvalumab plus BCG (I+M) had a tolerable and manageable safety profile that was consistent with
the known safety profiles of the individual agents, with no deaths due to treatment-related AEs
POTOMAC supports 1 year of durvalumab in combination with BCG induction and maintenance
as a potential new treatment for patients with BCG-naïve, high-risk NMIBC
congress
BERLIN
2025
ESMO
AE, adverse event BCG, bacillus Calmette-Guénn CI, confidence interval DFS, disease-free survival, HR hazard ratio; I, induction M, maintenance, NMIBC non-muscle-invasive bladder cancer, OS, overall survival
Q
=
AstraZeneca
Imfinzi approved in the US
in first and only
immunotherapy
combination for patients
with BCG-naïve, high-risk
non-muscle-invasive
bladder cancer.
PUBLISHED
28 May 2026
FDA Approves Durvalumab in
Combination with Bacillus
Calmette-Guerin for High-Risk Non-
Muscle Invasive Bladder Cancer
As a service to our members, the American Association
for Cancer Research will distribute information from the
U.S. Food and Drug Administration about newly
approved novel therapies for cancer patients. By doing
so, we aim to help the FDA inform cancer researchers
and oncologists of recent approvals in a timely manner.
Included in the email from the FDA will be a link to the
product label, which will provide the relevant clinical
information on the indication, contraindications, dosing,
and safety. In sharing this information, the AACR does
not endorse any product or therapy and does not take
any position on the safety or efficacy of the product or
therapy described.
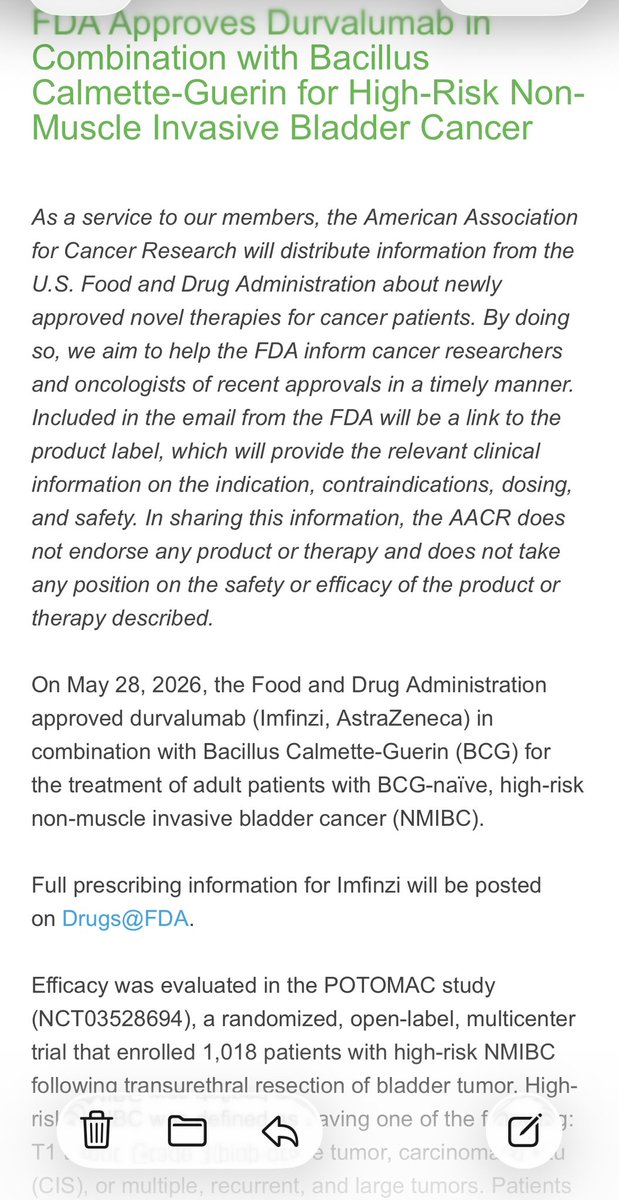
On May 28, 2026, the Food and Drug Administration
approved durvalumab (Imfinzi, AstraZeneca) in
combination with Bacillus Calmette-Guerin (BCG) for
the treatment of adult patients with BCG-naïve, high-risk
non-muscle invasive bladder cancer (NMIBC).
Full prescribing information for Imfinzi will be posted
on Drugs@FDA.
Efficacy was evaluated in the POTOMAC study
(NCT03528694), a randomized, open-label, multicenter
trial that enrolled 1,018 patients with high-risk NMIBC
following transurethral resection of bladder tumor. High-
risl
aving one of the f
7:
T1
e tumor, carcinoma
d
(CIS), or multiple, recurrent, and large tumors. Patients
14:12
5G
010
thelancet.com
X
THE LANCET
of
Search for.
Q
COMMENT - Online first, October 17, 2025
Front-line durvalumab and BCG in
the treatment of non-muscle-
invasive bladder cancer
Andrea Necchi a,b
X
. Alberto Briganti a,c .
Francesco Montorsi a,c
Affiliations & Notes
<
Article Info
<
Linked Articles (1)
>
Over the past 5 years, systemic therapy for urothelial
carcinoma has changed considerably throughout the
clinical stages. 1 In addition to regulatory approvals of
immune-checkpoint inhibitor (ICI)-based therapies for
muscle-invasive or metastatic disease, advances have
also been made for non-muscle-invasive bladder
cancer (NMIBC). Nadofaragene firadenovec-vncg,
nogapendekin alfa inbakicept-pmln, and gemcitabine
%
Get Access
Outline
Share
More
BERLIN
2025
ESMO
congress
BERLIN GERMANY
17-21 OCTOBER 2025
---
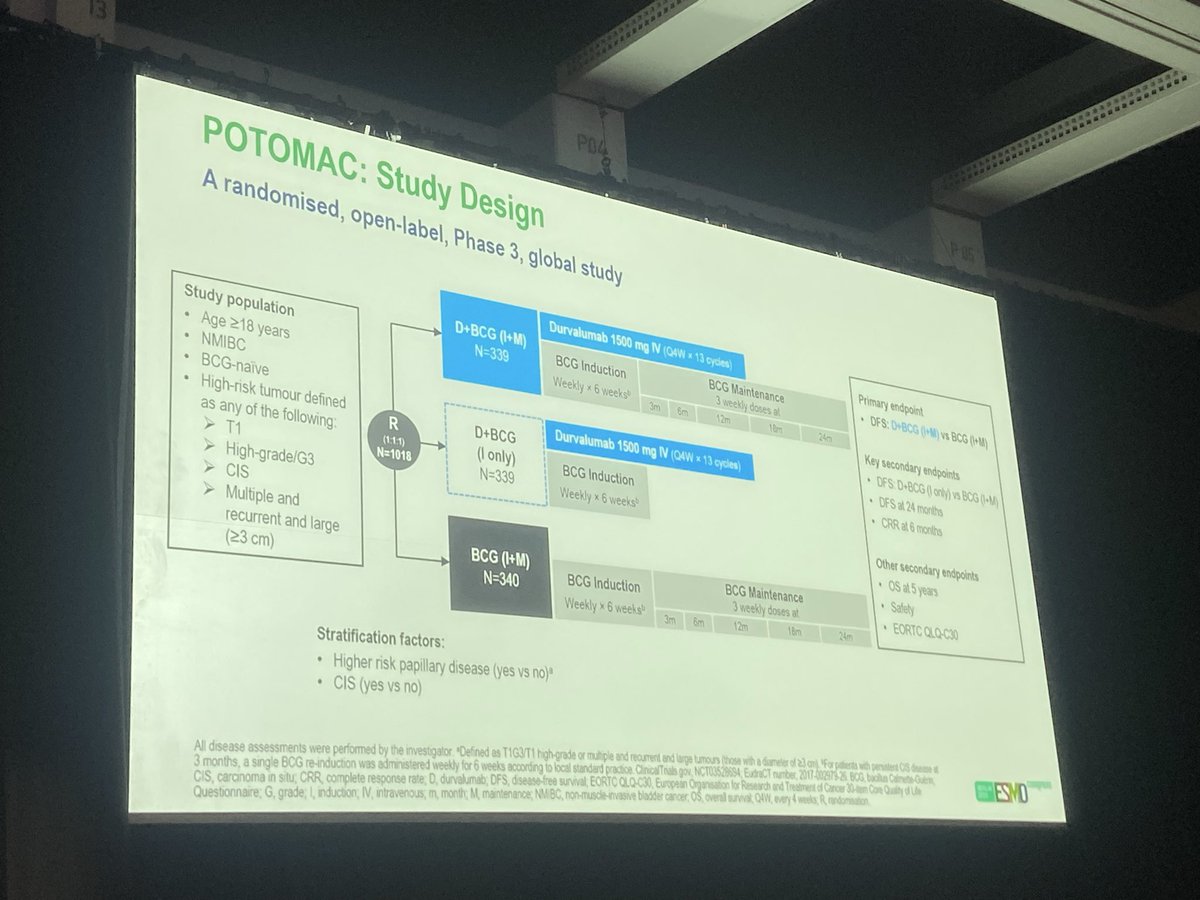
POTOMAC: Study Design
A randomised, open-label, Phase 3, global study
Durvalumab 1500 mg IV (Q4W X 13 cycles)
D+BCG (I+M)
Primary endpoint
Study population
N=339
BCG Induction
BCG Maintenance
3 weekly doses at
DFS: D+BCG (I+M) vs BCG (1+M)
Age ≥18 years
Weekly X 6 weeks®
NMIBC
3m
6m
12m
1 Pm
24m
BCG-naive
Key secondary endpoints
High-risk tumour defined
R
D+BCG
Durvalumab 1500 mg IV (Q4W X 13 cycles)
DFS: D+BCG 0 only) vs BCG (I+M)
as any of the following:
(1:11)
(I only)
DFS at 24 months
T1
N=1018
BCG Induction
High-grade/G3
N=339
CRR at 6 months
Weekly X 6 weeks
CIS
Multiple and
Other secondary endpoints
recurrent and large
OS at 5 years
(>3 cm)
BCG (I+M)
BCG Induction
BCG Maintenance
N=340
Safety
3 weekly doses at
Weekly X 6 weeks
EORTC QLQ-C30
3m
5m
12m
18m
24m
Stratification factors:
Higher risk papillary disease (yes VS no)*
CIS (yes VS no)
All disease assessments were performed by the investigator. Defined 05 T1G3/T1 high-grade or multiple and recument and large tumours (those with I diameter of 23 and For patients with persistent OS Income I
3 months, a single BCG re-induction was administered weekly for 6 weeks according to local standard practice. ClinicalTrials gov, NCT03528694; EudraCT number, 2017-002979-26 BCG bacilus Calinete-Guém,
Questionnaire: G, grade; , induction IV, intravenous, m, month; M maintenance; NMBC, non-muscle-invasive bladder cancer OS, overall survival, Q4W, every 4 weeks, R rendomisation
CIS, carcinoma in situ, CRR complete response rate, D, durvalumab, DFS, disease-free survival, EORTC QLQ-C30, European Organisation for Research and Treatment of Cancer 30-tem Core Quality of Lie
ESMO
---
POTOMAC: Disease-Free Survival for D+BCG (I+M) VS BCG (I+M) - ITT
POTOMAC met its primary endpoint with early and sustained DFS benefit
D+BCG (I+M)
BCG (I+M)
N=339
N=340
1.0
Events, n (%)
92%
67(20)
98(29)
Median DFS, months
NR
87%
NR
(95% CI)
82%
(NR-NR)
(74.0-NR)
0.8
87%
82%
77%
Probability of DFS
0.6
0.4
HR 0.68 (95% CI, 0.50-0.93)
Stratified log-rank P value® = 0.0154
0.2
Median follow-upb: 60.7 months
24% DFS maturity
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
51
54
57
60
63
66
69
72
75
78
81
Time from randomisation (months)
No. of patients at risk
D+BCG (I+M) 339 321 304 292 289 283 278 273 262 257 250 245 235 229 226 222 220 204 195 156 145 108 94 57 20 9 1 0
BCG (I+M) 340 322 303 292 283 276 271 265 258 254 249 244 237 235 231 227 225 209 196 160 150 101 86 50 20 8 0 0
DFS is defined as the time to the first: 1) recurrence of high-risk disease (recurrence of high-grade Ta, T1, or CIS, presentation with MIBC and/or metastatic disease or persistent CIS #6 months): 2) death by any
cause in the absence of recurrence *The threshold to declare statistical significance was based on a generalized Haybittle-Peto spending function- with the observed number of events, the boundary for declaring
statistical significance was 0.0317 for a 5% overall 2-sided alpha. Mn censored patients across all study arms. Data cutoff 03 April 2025 BCG, bacillus Calmette-Guénn; CL confidence interval, CIS, caronoma a sa,
ESMO
D, durvalumab; DFS, disease-free survival; HR, hazard ratio, I, induction; ITT, intent-to-treat population; M, maintenance, MIBC, muscle-invasive bladder cancer, NR not reached.
---
POTOMAC: Conclusions
Durvalumab in combination with BCG (I+M) resulted in a statistically significant and clinically
meaningful improvement in DFS VS BCG (I+M) alone in patients with BCG-naive, high-risk NMIBC
at a median of 5 years of follow-up
Scan the OR code to access
Side presentation
32% reduction in risk of a DFS event (HR 0.68; 95% CI, 0.50-0.93; P=0.0154)
Plan language surmary
Crass If is - and
trugh to DI - is " -
Early and sustained DFS benefit with durvalumab (starting at <4 months)
- (6) as ray
- etc. - #
for ukin
After a median follow-up of >5 years (14% maturity), a descriptive analysis showed an OS HR of
0.80 (95% CI, 0.53-1.20), demonstrating no detriment to OS with the addition of durvalumab
Durvalumab plus BCG (I+M) had a tolerable and manageable safety profile that was consistent with
the known safety profiles of the individual agents, with no deaths due to treatment-related AEs
POTOMAC supports 1 year of durvalumab in combination with BCG induction and maintenance
as a potential new treatment for patients with BCG-naïve, high-risk NMIBC
an
AE, adverse event, BCG, bacillus Calmette-Guérin CI, confidence interval; DFS, disease free survival, HR, hazard ratio, 1, induction M. mantenance, NMBC, non made name Madder canar, 05, overall und
ESMO
POTOMAC: Study Design
A randomised, open-label, Phase 3, global study
Durvalumab 1500 mg IV (Q4W X 13 cycles)
Primary endpoint
D+BCG (I+M)
BCG Induction
BCG Maintenance
Study population
N=339
DFS: D+BCG (I+M) vs BCG (I+M)
3 weekly doses at
Age ≥18 years
Weekly x 6 weeks
3ml
6m
12m
18m
24m
NMIBC
Key secondary endpoints
BCG-naive
High-risk tumour defined
Durvalumab 1500 mg IV (Q4W X 13 cycles)
DFS: D+BCG (I only) VS BCG (I+M)
as any of the following:
R
D+BCG
DFS at 24 months
(1:1:1)
T1
(I only)
BCG Induction
N=1018
CRR at 6 months
N=339
High-grade/G3
Weekly X 6 weeksb
CIS
Other secondary endpoints
Multiple and
recurrent and large
OS at 5 years
(≥3 cm)
BCG (I+M)
N=340
BCG Induction
BCG Maintenance
Safety
3 weekly doses at
EORTC QLQ-C30
Weekly x 6 weeks
3m
6m
12m
18m
24m
Stratification factors:
Higher risk papillary disease (yes VS no)a
CIS (yes VS no)
---
POTOMAC: Disease-Free Survival for D+BCG (I+M) VS BCG (I+M) - ITT
POTOMAC met its primary endpoint with early and sustained DFS benefit
D+BCG (I+M)
BCG (I+M)
N=339
N=340
Events, n (%)
67 (20)
98 (29)
1.0
92%
Median DFS, months
NR
NR
87%
(95% CI)
(NR-NR)
(74.0-NR)
82%
0.8
87%
82%
77%
Probability of DFS
0.6
+
0.4
HR 0.68 (95% CI, 0.50-0.93)
Stratified log-rank P valueᵃ = 0.0154
0.2
Median follow-upb: 60.7 months
24% DFS maturity
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
51
54
57
60
63
66
69
72
75
78
81
Time from randomisation (months)
No of patients at risk
D+BCG (I+M)
339
321
304
292
289
283
278
273
262
257
250
245
235
229
226
222
220
204
195
156
145
108
94
57
26
9
1
0
BCG (I+M)
340
322
303
292
283
276
271
265
258
254
249
244
237
235
231
227
225
209
196
160
150
101
86
50
20
8
0
0
---
POTOMAC: Disease-Free Survival for D+BCG (I Only) vs BCG (I+M) - ITT
Difference in DFS between D+BCG (I only) vs BCG (I+M) arms was not statistically significant
(key secondary endpoint)
D+BCG (I only)
BCG (I+M)
N=339
N=340
Events, n (%)
105 (31)
98 (29)
1.0
Median DFS, months
NR
NR
87%
(95% CI)
(NR-NR)
(74.0-NR)
82%
77%
0.8
86%
79%
74%
Probability of DFS
0.6
0.4
HR 1.14 (95% CI, 0.86-1.50)
Stratified log-rank P value = 0.3530
0.2
Median follow-upᵃ: 60.7 months
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
51
54
57
60
63
66
69
72
75
78
81
Time from randomisation (months)
No of patients at risk
D+BCG (I only)
339
314
296
281
269
261
250
246
240
236
227
219
217
212
210
201
198
186
173
145
130
92
79
47
20
13
1
0
BCG (I+M)
340
322
303
292
283
276
271
265
258
254
249
244
237
235
231
227
225
209
196
160
150
101
86
50
20
8
0
0
---
POTOMAC: Conclusions
Durvalumab in combination with BCG (I+M) resulted in a statistically significant and clinically
meaningful improvement in DFS VS BCG (I+M) alone in patients with BCG-naïve, high-risk NMIBC
Scan the QR code to access:
at a median of 5 years of follow-up
Slide presentation
Plain language summary
32% reduction in risk of a DFS event (HR 0.68; 95% CI, 0.50-0.93; P=0.0154)
Copies of this presentation obtained
through the QR code are for personal
Early and sustained DFS benefit with durvalumab (starting at <4 months)
use only and may not be reproduced
without written permission of
the authors
After a median follow-up of >5 years (14% maturity), a descriptive analysis showed an OS HR of
0.80 (95% CI, 0.53-1.20), demonstrating no detriment to OS with the addition of durvalumab
Durvalumab plus BCG (I+M) had a tolerable and manageable safety profile that was consistent with
the known safety profiles of the individual agents, with no deaths due to treatment-related AEs
POTOMAC supports 1 year of durvalumab in combination with BCG induction and maintenance
as a potential new treatment for patients with BCG-naïve, high-risk NMIBC
congress
BERLIN
2025
ESMO
AE, adverse event BCG, bacillus Calmette-Guénn CI, confidence interval, DFS, disease-free survival HR hazard ratio, I, induction M. maintenance, NMIBC non-muscle-invasive bladder cancer, OS, overall survival
POTOMAC: Study Design
A randomised, open-label, Phase 3, global study
Durvalumab 1500 mg IV (Q4W x 13 cycles)
Primary endpoint
D+BCG (I+M)
BCG Induction
BCG Maintenance
Study population
N=339
DFS: D+BCG (I+M) vs BCG (I+M)
3 weekly doses at
Age ≥18 years
Weekly x 6 weeks
3ml.
6m
12m
18m
24m
NMIBC
Key secondary endpoints
BCG-naive
High-risk tumour defined
Durvalumab 1500 mg IV (Q4W X 13 cycles)
DFS: D+BCG (I only) VS BCG (I+M)
as any of the following:
R
D+BCG
DFS at 24 months
(1:1:1)
T1
(I only)
BCG Induction
N=1018
CRR at 6 months
N=339
High-grade/G3
Weekly X 6 weeksb
CIS
Other secondary endpoints
Multiple and
recurrent and large
OS at 5 years
(≥3 cm)
BCG (I+M)
N=340
BCG Induction
BCG Maintenance
Safety
3 weekly doses at
EORTC QLQ-C30
Weekly x 6 weeks
3m
6m
12m
18m
24m
Stratification factors:
Higher risk papillary disease (yes VS no)a
CIS (yes VS no)
---
POTOMAC: Disease-Free Survival for D+BCG (I+M) VS BCG (I+M) - ITT
POTOMAC met its primary endpoint with early and sustained DFS benefit
D+BCG (I+M)
BCG (I+M)
N=339
N=340
Events, n (%)
67 (20)
98 (29)
1.0
92%
Median DFS, months
NR
NR
87%
(95% CI)
(NR-NR)
(74.0-NR)
82%
0.8
87%
82%
77%
Probability of DFS
0.6
+
0.4
HR 0.68 (95% CI, 0.50-0.93)
Stratified log-rank P valueᵃ = 0.0154
0.2
Median follow-upb: 60.7 months
24% DFS maturity
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
51
54
57
60
63
66
69
72
75
78
81
Time from randomisation (months)
No of patients at risk
D+BCG (I+M)
339
321
304
292
289
283
278
273
262
257
250
245
235
229
226
222
220
204
195
156
145
108
94
57
26
9
1
0
BCG (I+M)
340
322
303
292
283
276
271
265
258
254
249
244
237
235
231
227
225
209
196
160
150
101
86
50
20
8
0
0
---
POTOMAC: Disease-Free Survival for D+BCG (I Only) vs BCG (I+M) - ITT
Difference in DFS between D+BCG (I only) vs BCG (I+M) arms was not statistically significant
(key secondary endpoint)
D+BCG (I only)
BCG (I+M)
N=339
N=340
Events, n (%)
105 (31)
98 (29)
1.0
Median DFS, months
NR
NR
87%
(95% CI)
(NR-NR)
(74.0-NR)
82%
77%
0.8
86%
79%
74%
Probability of DFS
0.6
0.4
HR 1.14 (95% CI, 0.86-1.50)
Stratified log-rank P value = 0.3530
0.2
Median follow-upᵃ: 60.7 months
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
51
54
57
60
63
66
69
72
75
78
81
Time from randomisation (months)
No of patients at risk
D+BCG (I only)
339
314
296
281
269
261
250
246
240
236
227
219
217
212
210
201
198
186
173
145
130
92
79
47
20
13
1
0
BCG (I+M)
340
322
303
292
283
276
271
265
258
254
249
244
237
235
231
227
225
209
196
160
150
101
86
50
20
8
0
0
---
POTOMAC: Conclusions
Durvalumab in combination with BCG (I+M) resulted in a statistically significant and clinically
meaningful improvement in DFS VS BCG (I+M) alone in patients with BCG-naïve, high-risk NMIBC
Scan the QR code to access:
at a median of 5 years of follow-up
Slide presentation
Plain language summary
32% reduction in risk of a DFS event (HR 0.68; 95% CI, 0.50-0.93; P=0.0154)
Copies of this presentation obtained
through the QR code are for personal
Early and sustained DFS benefit with durvalumab (starting at <4 months)
use only and may not be reproduced
without written permission of
the authors
After a median follow-up of >5 years (14% maturity), a descriptive analysis showed an OS HR of
0.80 (95% CI, 0.53-1.20), demonstrating no detriment to OS with the addition of durvalumab
Durvalumab plus BCG (I+M) had a tolerable and manageable safety profile that was consistent with
the known safety profiles of the individual agents, with no deaths due to treatment-related AEs
POTOMAC supports 1 year of durvalumab in combination with BCG induction and maintenance
as a potential new treatment for patients with BCG-naïve, high-risk NMIBC
congress
BERLIN
2025
ESMO
AE, adverse event BCG, bacillus Calmette-Guénn CI, confidence interval, DFS, disease-free survival HR hazard ratio, I, induction M. maintenance NMIBC non-muscle-invasive bladder cancer, OS, overall survival
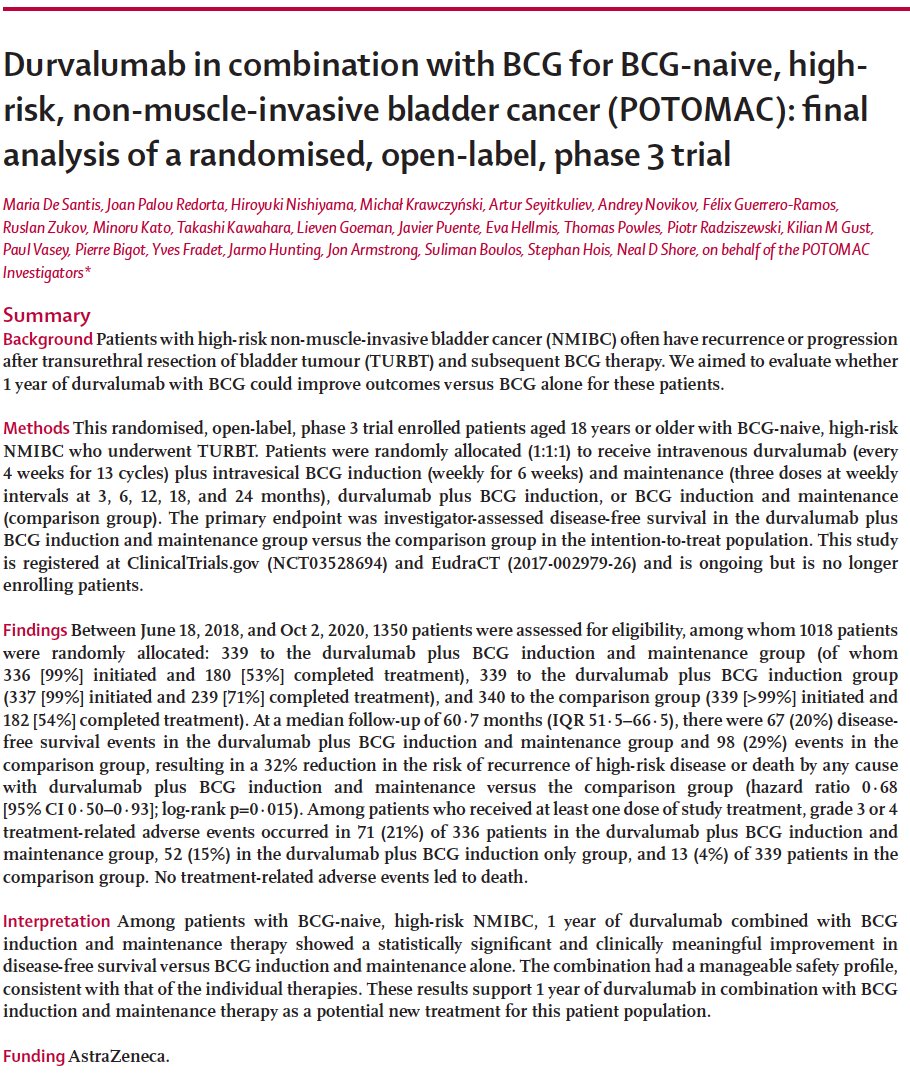
Durvalumab in combination with BCG for BCG-naive, high-
risk, non-muscle-invasive bladder cancer (POTOMAC): final
analysis of a randomised, open-label, phase 3 trial
Maria De Santis, Joan Palou Redorta, Hiroyuki Nishiyama, Michal Krawczyński, Artur Seyitkuliev, Andrey Novikov, Félix Guerrero-Ramos,
Ruslan Zukov, Minoru Kato, Takashi Kawahara, Lieven Goeman, Javier Puente, Eva Hellmis, Thomas Powles, Piotr Radziszewski, Kilian M Gust,
Paul Vasey, Pierre Bigot, Yves Fradet, Jarmo Hunting, Jon Armstrong, Suliman Boulos, Stephan Hois, Neal D Shore, on behalf of the POTOMAC
Investigators*
Summary
Background Patients with high-risk non-muscle-invasive bladder cancer (NMIBC) often have recurrence or progression
after transurethral resection of bladder tumour (TURBT) and subsequent BCG therapy. We aimed to evaluate whether
1 year of durvalumab with BCG could improve outcomes versus BCG alone for these patients.
Methods This randomised, open-label, phase 3 trial enrolled patients aged 18 years or older with BCG-naive, high-risk
NMIBC who underwent TURBT. Patients were randomly allocated (1:1:1) to receive intravenous durvalumab (every
4 weeks for 13 cycles) plus intravesical BCG induction (weekly for 6 weeks) and maintenance (three doses at weekly
intervals at 3, 6, 12, 18, and 24 months), durvalumab plus BCG induction, or BCG induction and maintenance
(comparison group). The primary endpoint was investigator-assessed disease-free survival in the durvalumab plus
BCG induction and maintenance group versus the comparison group in the intention-to-treat population. This study
is registered at ClinicalTrials.gov (NCT03528694) and EudraCT (2017-002979-26) and is ongoing but is no longer
enrolling patients.
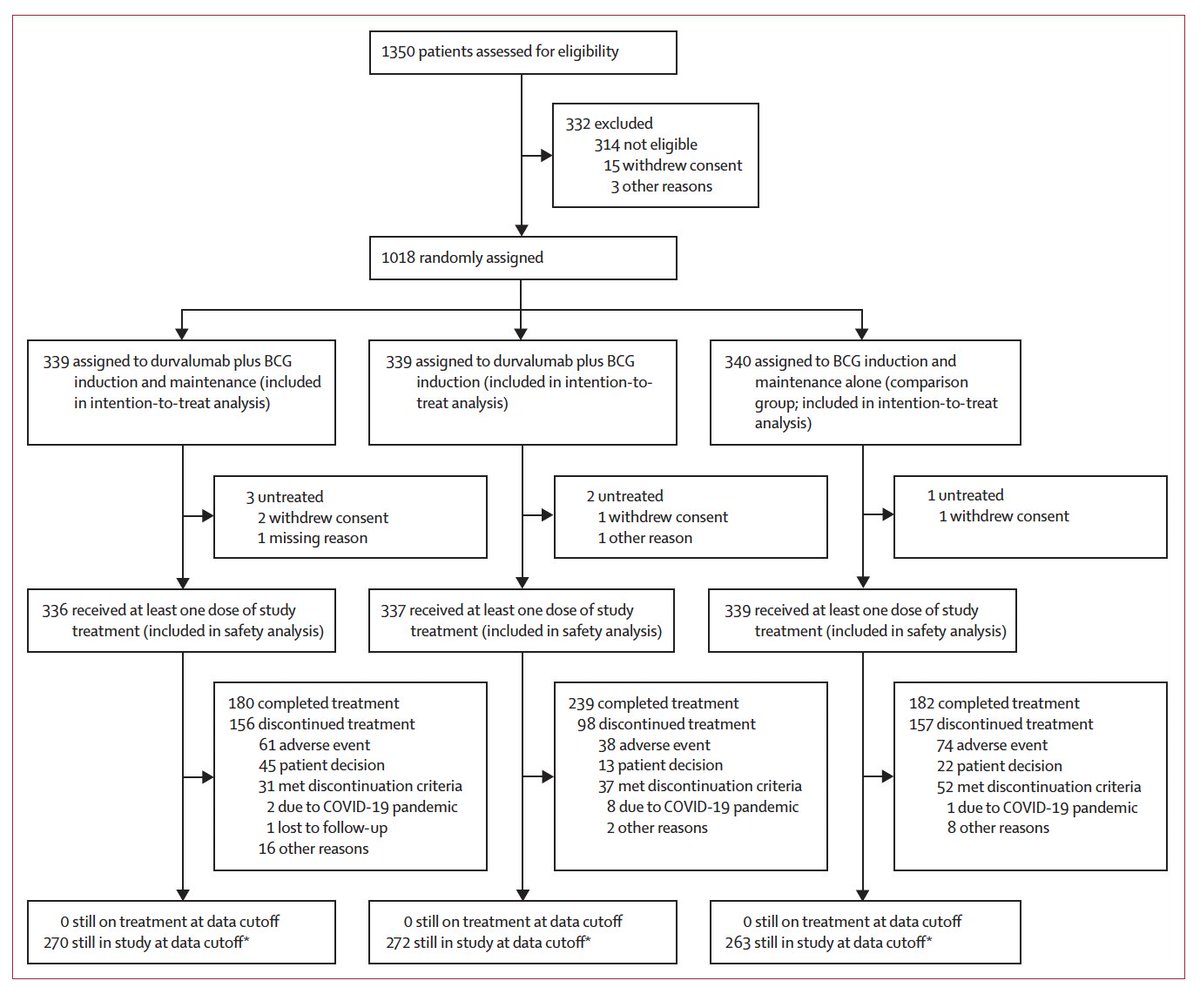
Findings Between June 18, 2018, and Oct 2, 2020, 1350 patients were assessed for eligibility, among whom 1018 patients
were randomly allocated: 339 to the durvalumab plus BCG induction and maintenance group (of whom
336 [99%] initiated and 180 [53%] completed treatment), 339 to the durvalumab plus BCG induction group
(337 [99%] initiated and 239 [71%] completed treatment), and 340 to the comparison group (339 [>99%] initiated and
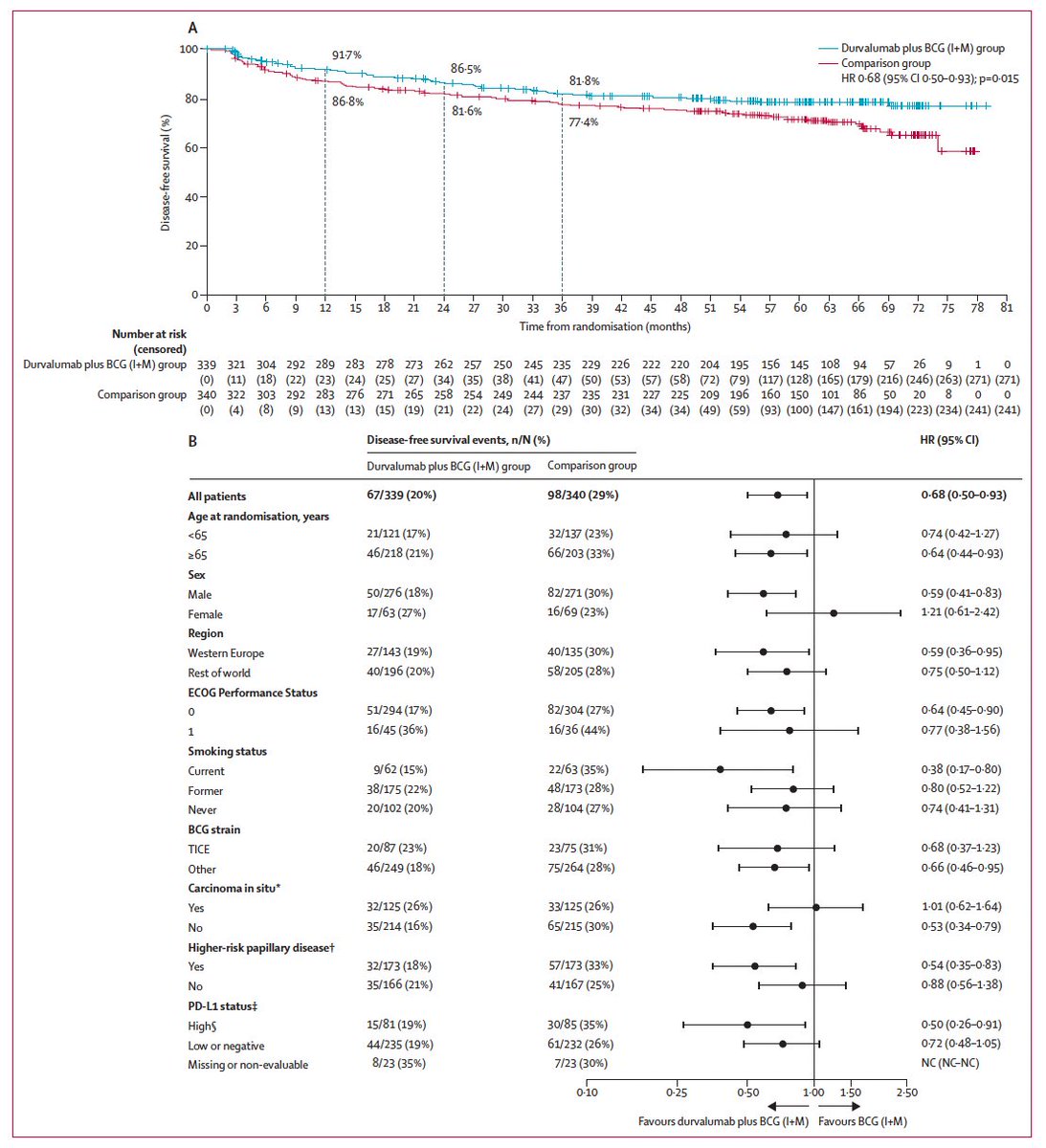
182 [54%] completed treatment). At a median follow-up of 60.7 months (IQR 51.5-66.5), there were 67 (20%) disease-
free survival events in the durvalumab plus BCG induction and maintenance group and 98 (29%) events in the
comparison group, resulting in a 32% reduction in the risk of recurrence of high-risk disease or death by any cause
with durvalumab plus BCG induction and maintenance versus the comparison group (hazard ratio 0.68
[95% CI .50-0.93]; log-rank p=0.015). Among patients who received at least one dose of study treatment, grade 3 or 4
treatment-related adverse events occurred in 71 (21%) of 336 patients in the durvalumab plus BCG induction and
maintenance group, 52 (15%) in the durvalumab plus BCG induction only group, and 13 (4%) of 339 patients in the
comparison group. No treatment-related adverse events led to death.
Interpretation Among patients with BCG-naive, high-risk NMIBC, 1 year of durvalumab combined with BCG
induction and maintenance therapy showed a statistically significant and clinically meaningful improvement in
disease-free survival versus BCG induction and maintenance alone. The combination had a manageable safety profile,
consistent with that of the individual therapies. These results support 1 year of durvalumab in combination with BCG
induction and maintenance therapy as a potential new treatment for this patient population.
Funding AstraZeneca.
---
1350 patients assessed for eligibility
332 excluded
314 not eligible
15 withdrew consent
3 other reasons
1018 randomly assigned
339 assigned to durvalumab plus BCG
339 assigned to durvalumab plus BCG
340 assigned to BCG induction and
induction and maintenance (included
induction (included in intention-to-
maintenance alone (comparison
in intention-to-treat analysis)
treat analysis)
group; included in intention-to-treat
analysis)
3 untreated
2 untreated
1 untreated
2 withdrew consent
1 withdrew consent
1 withdrew consent
1 missing reason
1 other reason
336 received at least one dose of study
337 received at least one dose of study
339 received at least one dose of study
treatment (included in safety analysis)
treatment (included in safety analysis)
treatment (included in safety analysis)
180 completed treatment
239 completed treatment
182 completed treatment
156 discontinued treatment
98 discontinued treatment
157 discontinued treatment
61 adverse event
38 adverse event
74 adverse event
45 patient decision
13 patient decision
22 patient decision
31 met discontinuation criteria
37 met discontinuation criteria
52 met discontinuation criteria
2 due to COVID-19 pandemic
8 due to COVID-19 pandemic
1 due to COVID-19 pandemic
1 lost to follow-up
2 other reasons
8 other reasons
16 other reasons
0 still on treatment at data cutoff
0 still on treatment at data cutoff
0 still on treatment at data cutoff
270 still in study at data cutoff*
272 still in study at data cutoff*
263 still in study at data cutoff*
---
Durvalumab plus
Durvalumab plus
Comparison
BCG induction and
BCG induction group
group
maintenance group
(n=339)
(n=340)
(n=339)
Age, years
Median (IQR)
68 (61-74)
68 (61-73)
67 (61-73)
<65
121 (36%)
123 (36%)
137 (40%)
>65
218 (64%)
216 (64%)
203 (60%)
Sex
Male
276 (81%)
272 (80%)
271 (80%)
Female
63 (19%)
67 (20%)
69 (20%)
Race
White
267 (79%)
267 (79%)
268 (79%)
Asian
61 (18%)
63 (19%)
60 (18%)
Other
4 (1%)
6 (2%)
8 (2%)
Missing
7 (2%)
3 (1%)
4 (1%)
Ethnicity
Hispanic or Latino
17 (5%)
14 (4%)
10 (3%)
Not Hispanic or Latino
322 (95%)
325 (96%)
330 (97%)
Region
Western Europe
143 (42%)
126 (37%)
135 (40%)
Rest of world
196 (58%)
213 (63%)
205 (60%)
ECOG performance status score
0
294 (87%)
305 (90%)
304 (89%)
1
45 (13%)
34 (10%)
36 (11%)
Smoking status
Current
62 (18%)
60 (18%)
63 (19%)
Former
175 (52%)
182 (54%)
173 (51%)
Never
102 (30%)
97 (29%)
104 (31%)
Carcinoma in situ*
Yes
125 (37%)
125 (37%)
125 (37%)
No
214 (63%)
214 (63%)
215 (63%)
Papillary disease only
Yes
217 (64%)
222 (65%)
220 (65%)
No
122 (36%)
117 (35%)
120 (35%)
T1 diseaset
195 (58%)
191 (56%)
211 (62%)
Ta diseaset
112 (33%)
114 (34%)
99 (29%)
Tumour PD-L1 expression
High$
81 (24%)
90 (27%)
85 (25%)
Low or negative
235 (69%)
228 (67%)
232 (68%)
Missing or non-evaluable
23 (7%)
21 (6%)
23 (7%)
Data are median (IQR) or n (%). ECOG=Eastern Cooperative Oncology Group. *Per interactive voice response system;
data represent patients who had carcinoma in situ (with or without papillary disease) at baseline. +Data represent
patients who had papillary disease (with or without carcinoma in situ). #PD-L1 status was determined by the
percentage of tumour cells with any membrane staining above background or by the percentage of tumour-associated
immune cells with staining at any intensity above background; ICP represents the percentage of tumour area occupied
by any tumour-associated immune cells; IC+ represents the percentage area of ICP showing PD-L1 positive immune cell
staining. SPD-L1 status was considered high if any of the following criteria were met: >25% of tumour cells showed
membrane staining; or ICPwas 1% and IC+ was >25%; or ICP was 1% and IC+ was 100%.
Table 1: Baseline demographic and disease characteristics of patients in the intention-to-treat
population
---
A
100
91.7%
Durvalumab plus BCG (I+M) group
86-5%
Comparison group
81-8%
HR 0-68 (95% CI 0-50-0-93); p=0-015
80
86.8%
81-6%
77-4%
Disease-free survival (%)
60
40
20
0
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
51
54
57
60
63
66
69
72
75
78
81
Number at risk
Time from randomisation (months)
(censored)
Durvalumab plus BCG (I+M) group
339
321
304
292
289
283
278
273
262
257
250
245
235
229
226
222
220
204
195
156
145
108
94
57
26
9
1
0
(0)
(11)
(18)
(22)
(23)
(24)
(25)
(27)
(34)
(35)
(38)
(41)
(47)
(50)
(53)
(57)
(58)
(72)
(79)
(117)
(128)
(165)
(179)
(216)
(246)
(263)
(271)
(271)
Comparison group
340
322
303
292
283
276
271
265
258
254
249
244
237
235
231
227
225
209
196
160
150
101
86
50
20
8
0
0
(0)
(4)
(8)
(9)
(13)
(13)
(15)
(19)
(21)
(22)
(24)
(27)
(29)
(30)
(32)
(34)
(34)
(49)
(59)
(93)
(100)
(147)
(161)
(194)
(223)
(234)
(241)
(241)
B
Disease-free survival events, n/N (%)
HR (95% CI)
Durvalumab plus BCG (I+M) group
Comparison group
All patients
67/339 (20%)
98/340 (29%)
0.68 (0-50-0-93)
Age at randomisation, years
<65
21/121 (17%)
32/137 (23%)
0.74 (0-42-1-27)
>65
46/218 (21%)
66/203 (33%)
0.64 (0-44-0-93)
Sex
Male
50/276 (18%)
82/271 (30%)
0.59 (0-41-0-83)
Female
17/63 (27%)
16/69 (23%)
1-21 (0-61-2-42)
Region
Western Europe
27/143 (19%)
40/135 (30%)
0.59 (0-36-0-95)
Rest of world
40/196 (20%)
58/205 (28%)
0.75 (0-50-1-12)
ECOG Performance Status
0
51/294 (17%)
82/304 (27%)
0-64 (0-45-0-90)
1
16/45 (36%)
16/36 (44%)
0.77 (0-38-1-56)
Smoking status
Current
9/62 (15%)
22/63 (35%)
0.38 (0-17-0-80)
Former
38/175 (22%)
48/173 (28%)
0.80 (0-52-1-22)
Never
20/102 (20%)
28/104 (27%)
0.74 (0-41-1-31)
BCG strain
TICE
20/87 (23%)
23/75 (31%)
0-68 (0-37-1-23)
Other
46/249 (18%)
75/264 (28%)
0-66 (0-46-0-95)
Carcinoma in situ*
Yes
32/125 (26%)
33/125 (26%)
1-01 (0-62-1-64)
No
35/214 (16%)
65/215 (30%)
0.53 (0-34-0-79)
Higher-risk papillary diseaset
Yes
32/173 (18%)
57/173 (33%)
0.54 (0-35-0-83)
No
35/166 (21%)
41/167 (25%)
0.88 (0-56-1-38)
PD-L1 status:
HighS
15/81 (19%)
30/85 (35%)
0.50 (0-26-0-91)
Low or negative
44/235 (19%)
61/232 (26%)
0.72 (0-48-1-05)
Missing or non-evaluable
8/23 (35%)
7/23 (30%)
NC (NC-NC)
0-10
0-25
0-50
1-00
1.50
2.50
Favours durvalumab plus BCG (I+M) Favours BCG (I+M)
POTOMAC (NCT03528694) is the randomized, open-label, multicenter Phase 3 trial that brought durvalumab (Imfinzi, AstraZeneca) into the curative-intent setting of BCG-naïve, high-risk non-muscle-invasive bladder cancer (NMIBC). 1,018 patients were randomized 1:1:1 after transurethral resection of bladder tumor (TURBT) to receive durvalumab every 4 weeks for 13 cycles plus BCG induction and maintenance, BCG induction and maintenance alone, or an investigational comparator arm. Presented at ESMO 2025 with simultaneous publication in The Lancet and with the final analysis subsequently presented at the 2026 ASCO GU and AUA meetings, POTOMAC met its primary endpoint of investigator-assessed disease-free survival (DFS HR 0.68; 95% CI 0.50–0.93; p=0.0154). On May 28, 2026, the FDA approved durvalumab in combination with BCG induction and maintenance for adult patients with BCG-naïve, high-risk NMIBC — the first new therapy approved for this population in over three decades.
Population
1,018 adults with BCG-naïve, high-risk NMIBC following TURBT. High-risk defined as ≥1 of: T1 tumor, grade 3/high-grade tumor, carcinoma in situ (CIS), or multiple, recurrent, and large Ta tumors.
Intervention
Durvalumab 1500 mg IV every 4 weeks for 13 cycles + BCG induction & maintenance vs BCG induction & maintenance alone vs an investigational comparator arm (1:1:1).
Primary Endpoint
Investigator-assessed disease-free survival (DFS) — time from randomization to first recurrence of high-risk NMIBC, persistent CIS, muscle-invasive disease, metastatic disease, or death.
Key Secondary
Time to recurrence, time to high-risk event, time to cystectomy, overall survival, safety/tolerability, and patient-reported outcomes.
Efficacy & Safety
Reported Results
Disease-Free Survival (Primary Endpoint)
Adding 1 year of durvalumab to BCG induction and maintenance produced a 32% reduction in the risk of disease recurrence, progression, or death versus BCG alone in BCG-naïve, high-risk NMIBC (HR 0.68; 95% CI 0.50–0.93; p=0.0154). At a median follow-up of 60.7 months, 67 DFS events were observed in the durvalumab + BCG arm vs 98 in BCG alone; median DFS was not reached in either arm. Median time to high-risk event was 14.1 months with durvalumab + BCG vs 8.3 months with BCG alone (AUA 2026 update).
Among patients who ultimately underwent cystectomy, median time to surgery was 19 months with durvalumab + BCG vs 14.1 months with BCG alone. The durvalumab + BCG regimen also delayed progression to muscle-invasive or metastatic disease, supporting its curative-intent positioning.
At the planned 5-year overall survival analysis (data cutoff 03 October 2025; median follow-up 72 months), adding durvalumab to BCG induction and maintenance showed no detriment to overall survival: HR 0.81 (95% CI 0.54–1.19). The 5-year OS rate was 87.6% with durvalumab + BCG vs 86.3% with BCG alone. Deaths occurred in 45 patients (13%) in the durvalumab + BCG arm vs 56 (16%) with BCG alone; median OS was not reached in either arm. Patient-reported outcomes (EORTC QLQ-C30 and QLQ-NMIBC24) showed modest deterioration from baseline in both arms with generally similar changes between arms; durvalumab did not have a major impact on quality of life. These data were presented June 1, 2026 at the ASCO Annual Meeting by Maria De Santis, MD.
The safety profile was consistent with the known durvalumab profile with no new safety signals attributable to the combination. Grade 3/4 treatment-related adverse events: 21% (durvalumab + BCG) vs 4% (BCG alone); no treatment-related deaths were reported. Immune-mediated adverse reactions, infusion-related reactions, and embryo-fetal toxicities are included as warnings/precautions in the prescribing information.
STATUSFDA Approved · May 28, 2026 · BCG-naïve high-risk NMIBC
On May 28, 2026, the U.S. FDA approved durvalumab (Imfinzi) in combination with Bacillus Calmette-Guérin (BCG) for adult patients with BCG-naïve, high-risk non-muscle-invasive bladder cancer. The approval covers high-risk disease defined as T1 tumor, grade 3/high-grade tumor, carcinoma in situ (CIS), or multiple, recurrent, and large tumors. Approved dosing is durvalumab 1500 mg IV every 4 weeks for 13 cycles plus BCG induction and maintenance. This is the first new therapy approved for BCG-naïve, high-risk NMIBC in over 30 years and the only immunotherapy combination approved in this setting.
POTOMAC (NCT03528694) is a Phase 3, AstraZeneca-sponsored randomized trial evaluating durvalumab (Imfinzi) added to BCG induction and maintenance versus BCG alone in patients with BCG-naive, high-risk non-muscle-invasive bladder cancer (NMIBC). Disease-free survival was the primary endpoint.
What did POTOMAC show?
Adding one year of durvalumab to BCG induction and maintenance reduced the risk of disease recurrence, progression, or death by 32% versus BCG alone (hazard ratio 0.68; 95% CI 0.50-0.93; p=0.0154) at a median follow-up of 60.7 months. At the planned 5-year analysis there was no detriment to overall survival (HR 0.81; 95% CI 0.54-1.19).
Is durvalumab plus BCG FDA approved for bladder cancer?
According to this page, the FDA approved durvalumab (Imfinzi) with BCG for BCG-naive, high-risk non-muscle-invasive bladder cancer on May 28, 2026, described as the first new therapy for this setting in over 30 years. Because this approval date is recent, clinicians should verify the exact indication wording against the official FDA labeling.
What is the safety profile of durvalumab plus BCG?
Grade 3/4 treatment-related adverse events occurred in 21% of patients with durvalumab plus BCG versus 4% with BCG alone, with no treatment-related deaths reported. The safety profile was consistent with the known durvalumab profile, with immune-mediated adverse reactions managed per standard guidance.
How does POTOMAC change treatment for high-risk NMIBC?
POTOMAC positions durvalumab plus BCG as a curative-intent option that delayed progression to muscle-invasive or metastatic disease and lengthened time to cystectomy versus BCG alone, addressing a setting with few advances in decades. Featured KOLs on the page discuss its role for BCG-naive, high-risk NMIBC patients.