[Slide 1]
ONC
Brother
Top 10 Anticipated Practice Changing/Informing Abstracts for ASCO 2025
from Community Oncology's (@OncBrothers) perspective
1. #Plenary Session: #ATOMIC Ph III, Adj FOLFOX VS. Atezolizumab +
FOLFOX for dMMR Stage III resected colon cancer.
2. #Plenary Session: #MATTERHORN Ph III, PeriOp Durvalumab + FLOT (and
postOP Durva + FLOT
Durva) VS PeriOP and PostOP FLOT for resectable
gastric/gastroesophageal junction cancer.
3. #PlenarySession: #SERENA6 Ph III, Camizestrant + CDK 4/6i VS AI + CDK 4/6i in
1L HR+/HER2- at the time of ESR1 emergence and prior to progression in
metastatic breast cancer. #VERITAC2, Ph III data for ARV-471 (an oral PROTAC
ER degrader) also being presented.
4. #ASCENT04: Ph III, Sacituzumab + Pembrolizumab VS. Chemo + Pembro in 1L
locally advanced or metastatic with PDL1+ (CPS≥10) triple negative breast
cancer.
5. #DESTINY-Breast09: Ph III, Trastuzumab Deruxtecan +/- Pertuzumab VS. THP in
1L locally advanced or metastatic HER2+ (IHC3+ or FISH+) breast cancer.
6. #IMforte: Ph III, Carbo + Etop + Atezoluzmab
Atezo + Lurbinectedin VS.
Atezo alone in maintenance 1L for extensive stage small cell lung cancer.
#DeLLphi304, Ph III, Tarlatamab in 2L also being presented.
7. #CheckMate816: Update, Ph III, Neoadjuvant Nivolumab + Chemotherapy
(approved in March 2022) VS. Chemo alone in resectable non-small cell lung
cancer.
8. #NIAGARA: Ph III, use of ctDNA in patients who received periOP durvalumab
(PeriOp/PostOp Durvalumab got approved in March 2025) muscle-invasive
bladder cancer.
9. #Plenary Session: #NIVOPOSTOP: Ph III, Adj Chemo + XRT + Nivolumab VS
Chemo + XRT in high risk resected head and neck squamous cell carcinoma
10. #Plenary Session: #VERIFY Ph III, Rusfertide (hepcidin mimetic agent) +
ongoing therapy VS Placebo in patients requiring frequent therapeutic
phlebotomies for Polycythemia Vera
www.oncbrothers.com
@Oncbrothers
O
@Oncbrothers
@Oncbrothers
[Slide 1]
CYSTECTOMY FOR ALL VS BLADDER SPARING
1 year
2 year
% alive and metastases free
Study
pTO
cCR
2 year os %
with bladder intact and not
MFS
MFS
radiated
AMVAC
COXEN: 32%
C: 75%
COXEN: 62%
COXEN: 82%
Cystectomy for All
-
0
VESPER:42%
V: 82%
VESPER: 73%
VESPER: 83%
(COXEN / VESPER)
AMVAC
Cystectomy by Allocation
-
36%
83%
73%
84%
17%
(RETAIN)
GC + Nivolumab pre/post
Cystectomy by Allocation
-
46%
90%*
82%*
88%*
32%*
(HCRN 16-257)
GC+ Durva pre/post
82%
74%
Cystectomy for all
37%
-
censoring those who
censoring those who
82%
0
(NIAGRA)
did not undergo RC
did not undergo RC
GC
COXEN: 34%
COXEN: 62%
COXEN: 57%
COXEN: 77%
Cystectomy for All
VESPER: 36%
-
VESPER: 76%
VESPER: 61%
VESPER: 78%
0
(COXEN / VESPER/NIAGRA)
NIAGRA: 28%
NIAGRA: 79%
NIAGRA: 87%
NIAGRA: 75%
Flaig T.W. et al. Clin Cancer Res 2021;27:2435-41
Pfister C. et al. Journal of Clinical Oncology 2023;41:LBA4507-LBA
Geynisman DM et al. GU ASCO Oral Presentation. Journal of Clinical Oncology 2023;41:438
Galsky MD, et al. Nature Medicine 2023
Powles et al. ESMO 2024
[Slide 1]
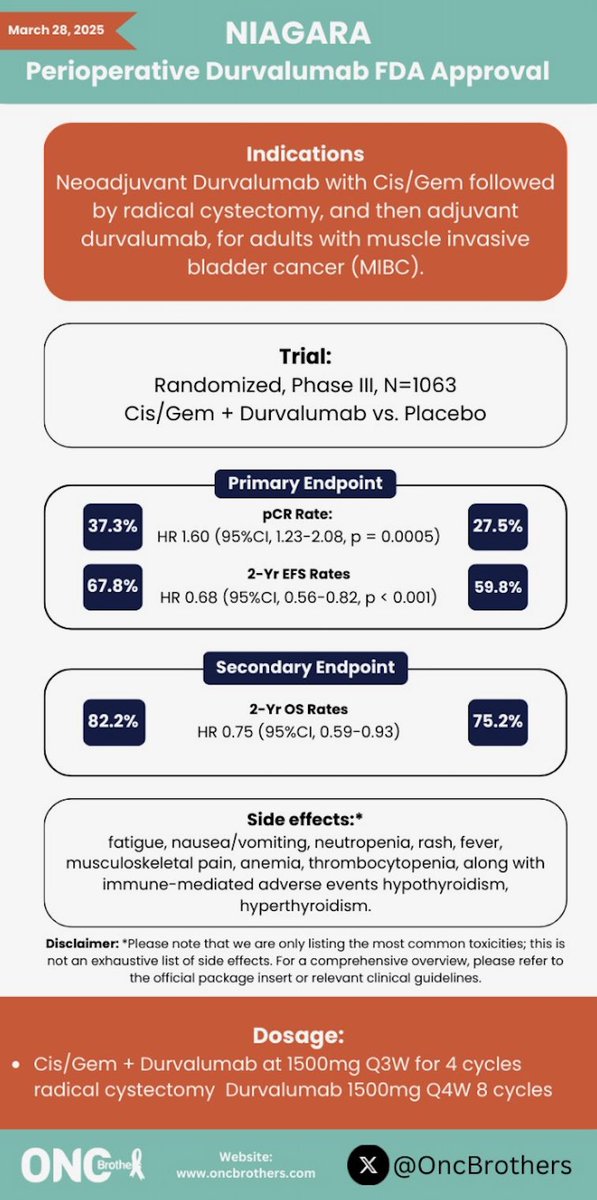
March 28, 2025
NIAGARA
Perioperative Durvalumab FDA Approval
Indications
Neoadjuvant Durvalumab with Cis/Gem followed
by radical cystectomy, and then adjuvant
durvalumab, for adults with muscle invasive
bladder cancer (MIBC).
Trial:
Randomized, Phase III, N=1063
Cis/Gem + Durvalumab VS. Placebo
Primary Endpoint
pCR Rate:
37.3%
27.5%
HR 1.60 (95%CI, 1.23-2.08, p = 0.0005)
2-Yr EFS Rates
67.8%
59.8%
HR 0.68 (95%CI, 0.56-0.82, p < 0.001)
Secondary Endpoint
2-Yr OS Rates
82.2%
75.2%
HR 0.75 (95%CI, 0.59-0.93)
Side effects:*
fatigue, nausea/vomiting, neutropenia, rash, fever,
musculoskeletal pain, anemia, thrombocytopenia, along with
immune-mediated adverse events hypothyroidism,
hyperthyroidism.
Disclaimer: *Please note that we are only listing the most common toxicities; this is
not an exhaustive list of side effects. For a comprehensive overview, please refer to
the official package insert or relevant clinical guidelines.
Dosage:
Cis/Gem + Durvalumab at 1500mg Q3W for 4 cycles
radical cystectomy Durvalumab 1500mg Q4W 8 cycles
ONC
Website:
Brothe
www.oncbrothers.com
X
@OncBrothers
First trial to demonstrate OS benefit with perioperative immunotherapy in cisplatin-eligible MIBC. Immediately practice-changing. Debate centers on optimal sequencing vs. adjuvant nivolumab (CheckMate-274) and patient selection across the perioperative/adjuvant/observation options.
FDA APPROVED Imfinzi — Durvalumab (Imfinzi) with gemcitabine and cisplatin as neoadjuvant treatment, followed by single-agent durvalumab as adjuvant treatment after radical cystectomy, in adult patients with muscle-invasive bladder cancer.
2-year EFS was 67.8% in the durvalumab+GC arm vs. 59.8% with chemotherapy alone (HR 0.68, 95% CI 0.56-0.82, P<0.0001). pCR rate: 37.3% vs. 27.5% (OR 1.6, P=0.0005).
Overall survival HR was 0.75 (95% CI 0.59-0.93, P=0.0106) favoring perioperative durvalumab. First trial demonstrating OS benefit with perioperative immunotherapy in MIBC.
Immune-related adverse events consistent with durvalumab monotherapy profile. No new safety signals. Radical cystectomy completion rates comparable between arms — perioperative durvalumab did not compromise surgical outcomes.
✓ No new safety signals; surgical outcomes preserved
✅ First OS-positive perioperative immunotherapy in cisplatin-eligible MIBC. First trial to demonstrate OS benefit with perioperative immunotherapy in cisplatin-eligible MIBC. Immediately practice-changing. Debate centers on optimal sequencing vs. adjuvant nivolumab (CheckMate-274) and patient selection across the perioperative/adjuvant/observation options.