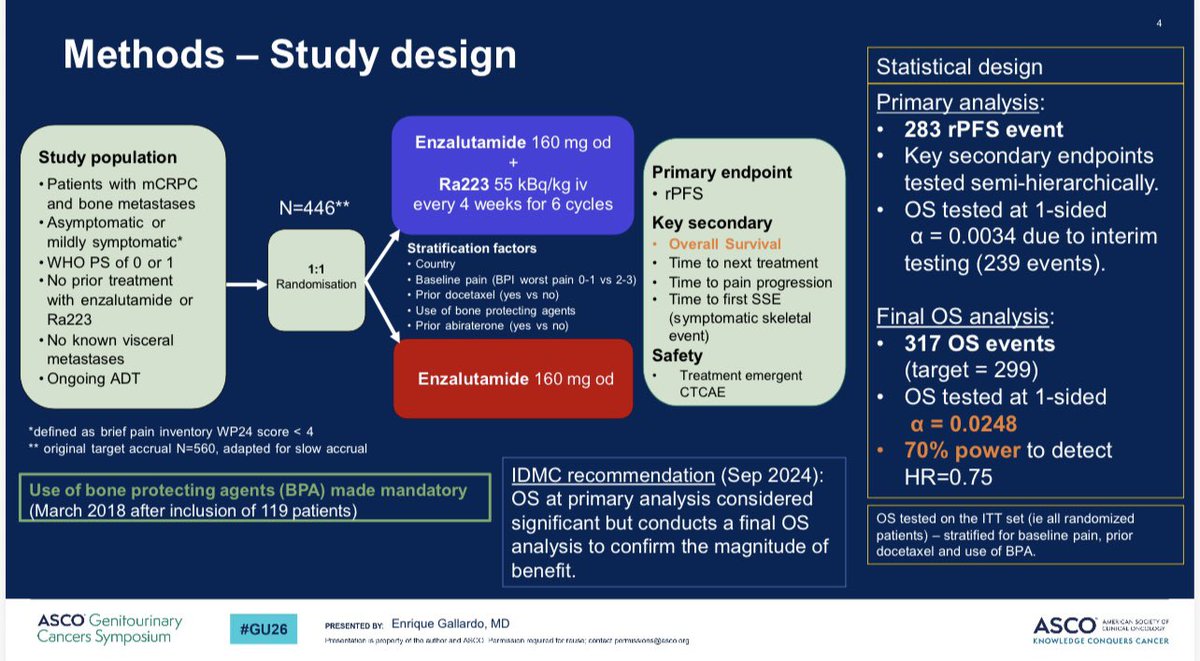
PEACE-3 (EORTC-1333; NCT02194842) is a Phase 3 trial of radium-223 (Xofigo) added to enzalutamide (Xtandi) versus enzalutamide alone in metastatic castration-resistant prostate cancer with bone metastases. Adding radium-223 improved radiographic progression-free survival (HR 0.69; p=0.0009) and overall survival (HR 0.76; p=0.0096; 5.6-month median gain), with mandatory bone-protective agents preventing prior fracture concerns. The combination is investigational. Sponsor: EORTC.
Discover KOL Sentiment on PEACE-3 →Design — Phase 3 randomized (EORTC-1333); radium-223 (Xofigo) + enzalutamide (Xtandi) vs enzalutamide alone, mCRPC with bone metastases, with mandatory bone-protective agents (NCT02194842). (ESMO 2024 / ASCO GU 2026)
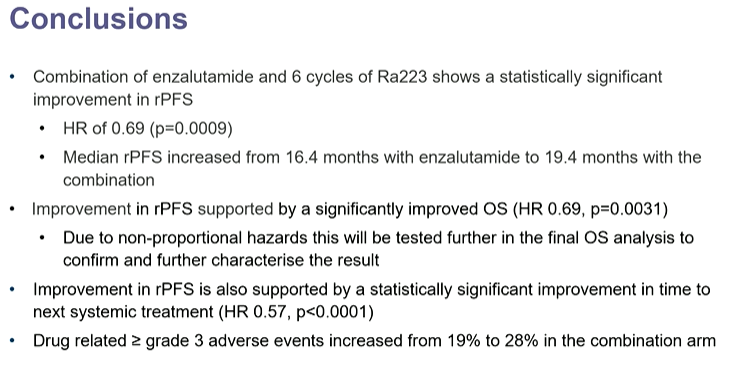
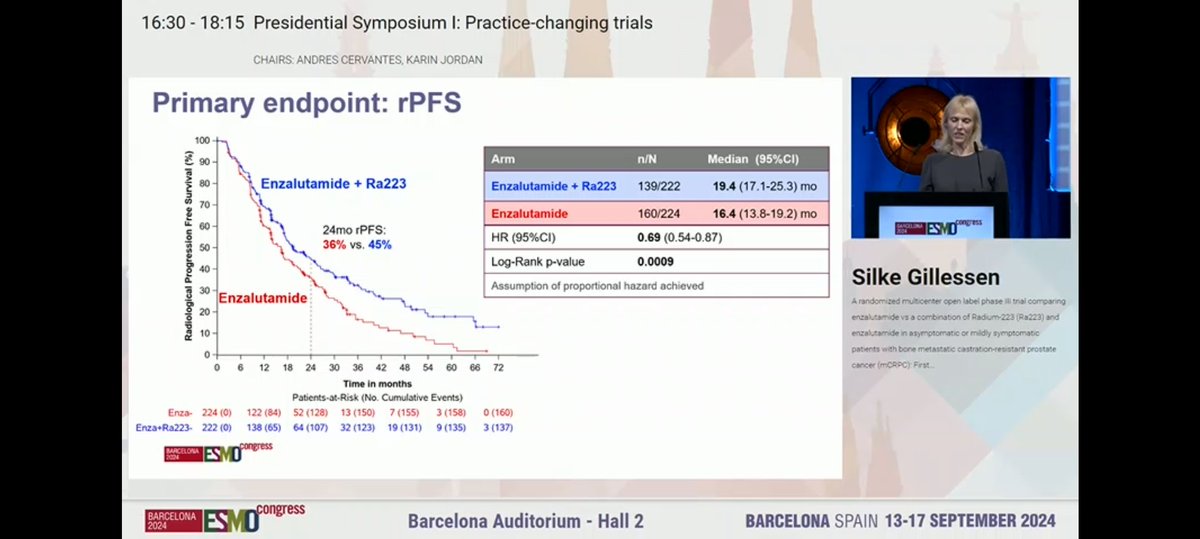
rPFS (primary) — Radiographic progression-free survival HR 0.69 (95% CI 0.54-0.87; p=0.0009) favoring the radium-223 + enzalutamide combination. (ESMO 2024)
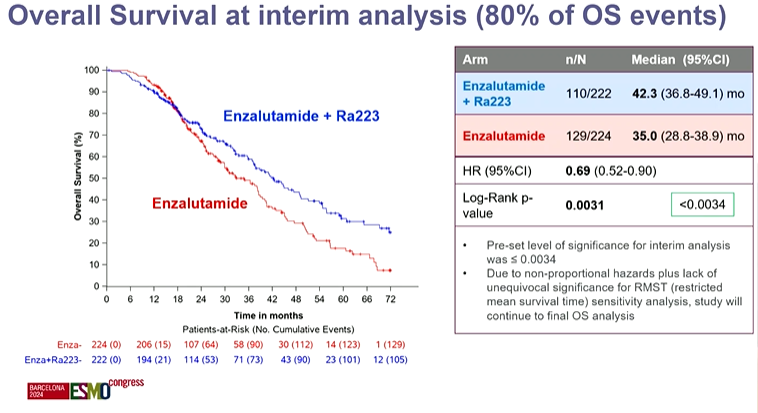
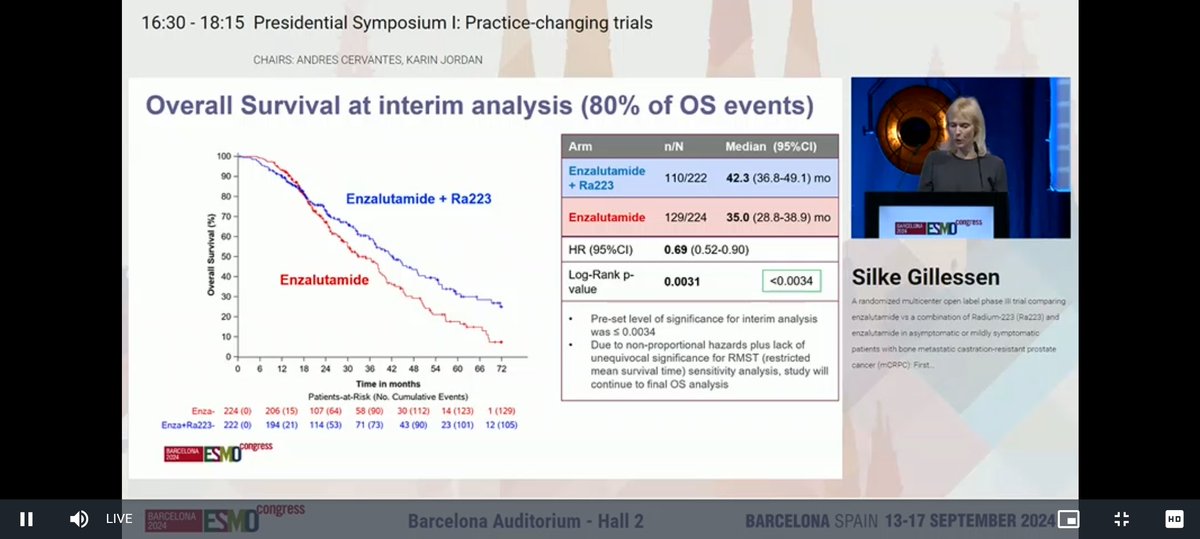
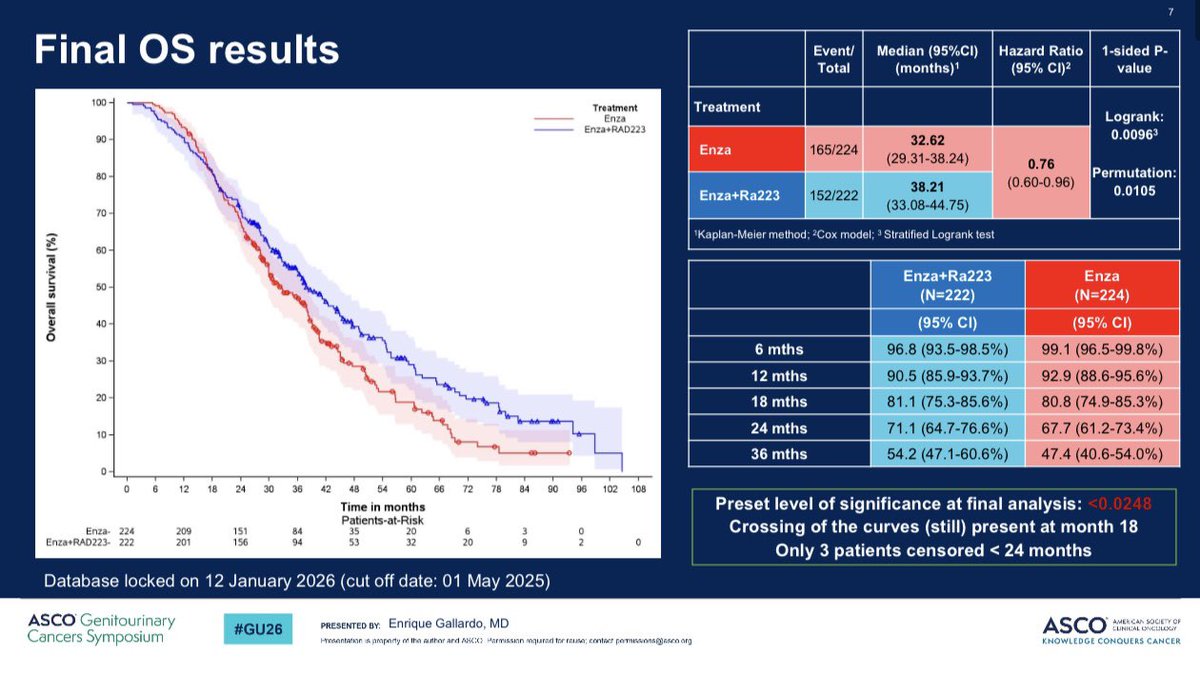
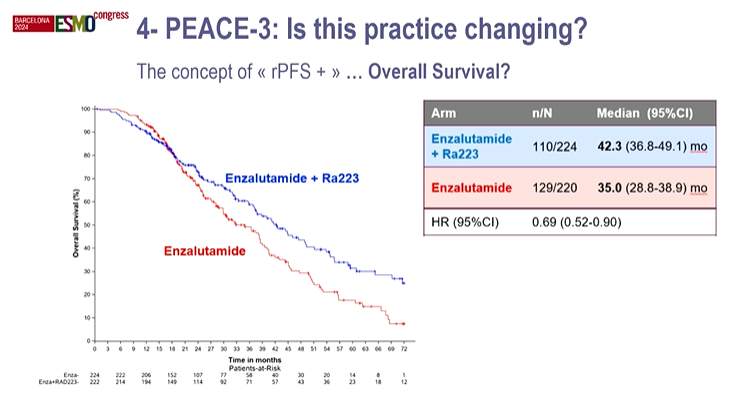
Overall survival — Final OS HR 0.76 (95% CI 0.60-0.96; p=0.0096); median gain 5.6 months; median follow-up 58 months; 317 deaths — first Phase 3 OS benefit for radium-223 plus an androgen-receptor pathway inhibitor. (ESMO 2024 / ASCO GU 2026)
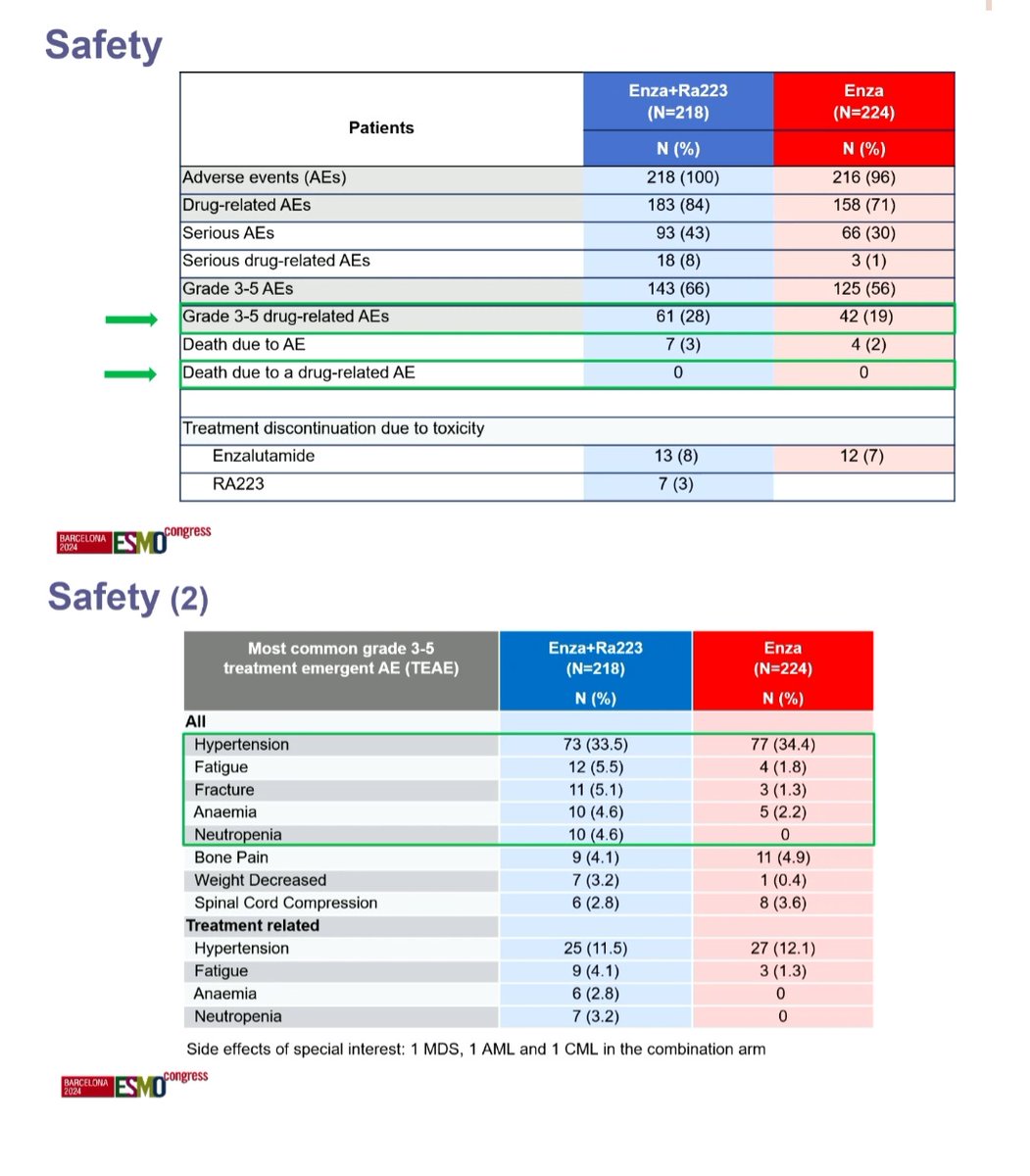
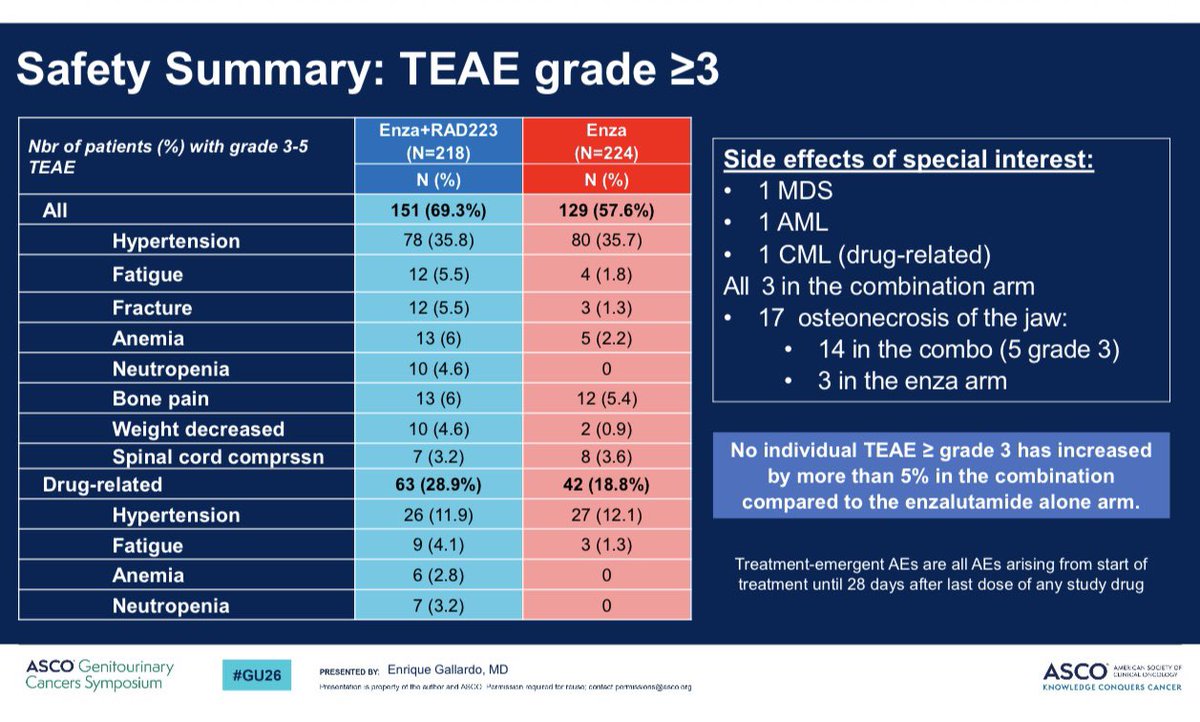
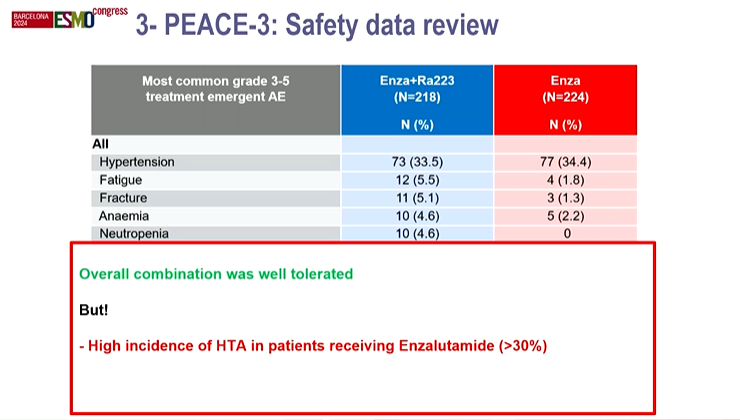
Safety — Grade >=3 treatment-emergent AEs 69.3% vs 57.6%; Grade >=3 treatment-related AEs 28.9% vs 18.8%; most frequent Grade >=3 event hypertension. (ESMO 2024)
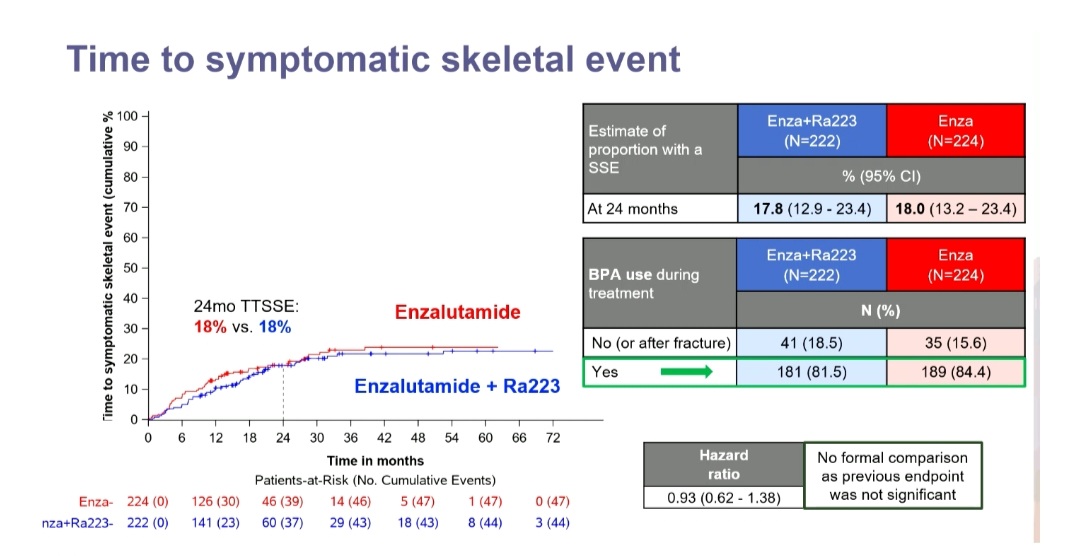
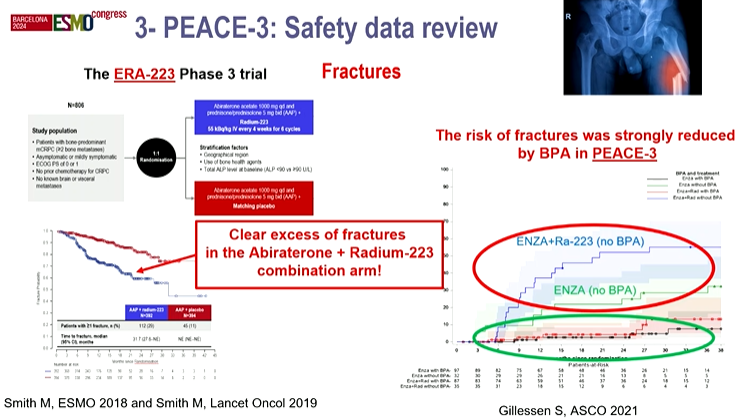
Fracture safety — Mandatory bone-protective agents (denosumab or zoledronic acid) prevented the fracture excess seen in the earlier ERA-223 trial. (ESMO 2024)
Regulatory / Sponsor — INVESTIGATIONAL combination — radium-223 + enzalutamide is not an FDA-approved regimen (each agent approved separately). EORTC, with Bayer and Astellas. (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.











Top tweets by impressions — click to view on X
Outstanding talk from @Silke_Gillessen elegantly presenting PEACE-3 phase 3 trials first results.
Adding 6 cycles of Ra223 to enzalutamide as first-line therapy for mCRPC showed significant rPFS…
PEACE-3 reinvigorating the role of Radium-223? Improves rPFS and likely OS as first line treatment in mCRPC in combination with enza. Results much more impressive than I expected!…
💫🌟💡 FANTASTIC! 👩🎓🔝#ESMO24 Presidential Symposium I: PEACE-3 Trial – Practice-Changing Results! 🎯
🔗 Presented by the GREAT!! @SilkeGillessen @APCCC_Lugano
@OncoAlert @myESMO
🔹 Combination of…
Significant OS (HR 0.76 CI:0.76-0.96) for PEACE-3 #GU26 . Enzalutamide +/- Radium-223 in metastatic CRPC (ARPI naive). This is its 2nd study with OS, but the clinical population is diminished as…
@Silke_Gillessen @myESMO @OncoAlert @urotoday @DrYukselUrun @yekeduz_emre @RashadNawfal @marc_eid @MarcMachaalani @ReneeSaliby @chadihc98 @BradMcG04 @VincentWenxinXu Followed by a thought-provoking…

What a great Day 1 at #ASCOGU26! Meeting friends & colleagues & learning about latest data in #ProstateCancer
Key Takeaways
👉PEACE-3: ARPI + radium-223 improves OS in mCRPC
👉BRCAAway:…
Dear Colleagues at #ESMO24 An honor to present our #OncoALertAF Barbara Melao @bavilima 🇧🇷 and Karine Martins da Trindade @karinemtrindad🇧🇷Chair of @LACOG_group GU and one of the PIs of PEACE-3…

🆕#ASCOGU26 concomitant publication: Final overall survival results from EORTC 1333/PEACE-3 trial of enzalutamide plus radium-223 in metastatic castration-resistant prostate cancer @Silke_Gillessen…
#ASCO #GU26
mCRPC finally getting durable OS signals?
@OncoAlert 🚨
Two abstracts. Two strategies.
One shared message: overall survival is moving.
🔵 PEACE-3 (Abstract 15)
Enzalutamide ± Radium-223
▪️…

ASCO GU prostate cancer updates 🎧
Dr. Evan Yu joins the Uromigos to discuss final OS results from PEACE-3, crossing survival curves, and the expanding role of radioligand therapy and PARP…
First phase 3 to demonstrate OS benefit combining radium-223 with a next-generation androgen receptor pathway inhibitor in mCRPC with bone mets. 5.6-month median OS improvement. Key caveat: mandatory bone-protective agents prevented the fracture excess seen in prior ERA-223 trial.
rPFS HR 0.69 (95% CI 0.54-0.87, P=0.0009) favoring enzalutamide + radium-223 over enzalutamide alone. First phase 3 combining radium-223 with a next-generation androgen receptor pathway inhibitor in mCRPC with bone metastases.
Final overall survival: HR 0.76 (95% CI 0.60-0.96, P=0.0096). Median OS benefit of 5.6 months with the combination. Median follow-up 58 months; 317 deaths at final analysis.
Grade ≥3 TEAEs: 69.3% with combination vs. 57.6% with enzalutamide alone. Grade ≥3 TRAEs: 28.9% vs. 18.8%. Most frequent G≥3 AE was hypertension. Mandatory bone-protective agents (denosumab / zoledronic acid) prevented the fracture excess seen in prior ERA-223 trial.
✅ Practice-informing OS benefit in mCRPC with bone mets. First phase 3 to demonstrate OS benefit combining radium-223 with a next-generation androgen receptor pathway inhibitor in mCRPC with bone mets. 5.6-month median OS improvement. Key caveat: mandatory bone-protective agents prevented the fracture excess seen in prior ERA-223 trial.
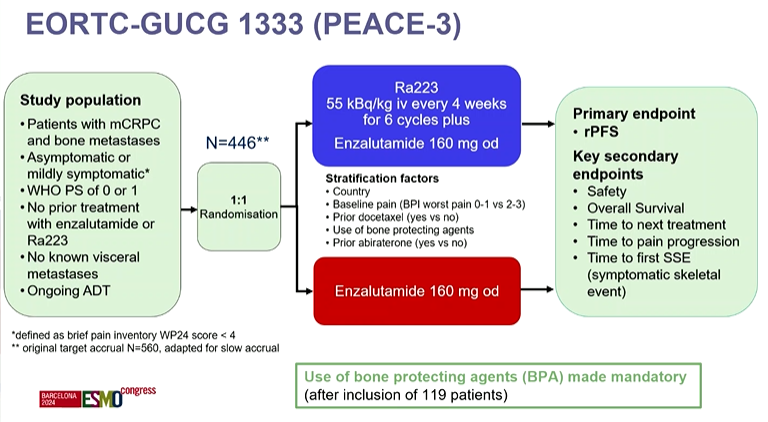
PEACE-3 (EORTC-1333; NCT02194842) is a Phase 3, randomized trial evaluating the alpha-emitting radiopharmaceutical radium-223 (Xofigo) combined with the androgen-receptor pathway inhibitor enzalutamide (Xtandi) versus enzalutamide alone in patients with metastatic castration-resistant prostate cancer and bone metastases. It was run by the EORTC, with Bayer and Astellas.
Adding radium-223 to enzalutamide improved radiographic progression-free survival (HR 0.69; p=0.0009) and overall survival (HR 0.76; p=0.0096), with a median overall-survival gain of 5.6 months at a median follow-up of 58 months. PEACE-3 is the first Phase 3 trial to show an overall-survival benefit from combining radium-223 with a next-generation androgen-receptor pathway inhibitor.
No. The specific radium-223 (Xofigo) plus enzalutamide (Xtandi) combination studied in PEACE-3 is investigational and not an FDA-approved regimen. Radium-223 is separately approved for castration-resistant prostate cancer with symptomatic bone metastases and no visceral disease, and enzalutamide is separately approved across prostate cancer settings, but the combination is not.
An earlier trial (ERA-223) combining radium-223 with abiraterone showed an excess of fractures. PEACE-3 made bone-protective agents (denosumab or zoledronic acid) mandatory, which prevented that fracture excess — an important design lesson that allowed the survival benefit of the radium-223 combination to be realized safely.
Grade 3 or higher treatment-emergent adverse events occurred in about 69.3% of combination patients versus 57.6% with enzalutamide alone, and Grade 3 or higher treatment-related events in 28.9% versus 18.8%. The most frequent Grade 3 or higher event was hypertension. With mandatory bone-protective agents, the fracture excess seen in prior radium-223 combination trials was avoided.