FDA-approved May 22, 2026 — datopotamab deruxtecan (Datroway) as first-line treatment for unresectable/metastatic TNBC in patients who are not PD-1/PD-L1 inhibitor candidates. Pivotal Phase III TROPION-Breast02: PFS HR 0.57; OS HR 0.79 (23.7 vs 18.7 mo) — a new 1L standard of care.
Discover KOL Sentiment on TROPION-Breast02 →Design - Phase 3 datopotamab deruxtecan (Dato-DXd) vs investigator's-choice chemotherapy, first-line metastatic TNBC not eligible for PD-1/PD-L1 therapy (NCT05374512); N=644 (323 vs 321).
PFS (primary) - Median 10.8 vs 5.6 mo, HR 0.57 (95% CI 0.47-0.69), P<0.0001 - primary endpoint met.
OS - Median 23.7 vs 18.7 mo, HR 0.79 (95% CI 0.64-0.98), P=0.0290 - significant; first targeted therapy to beat chemo on OS in this setting.
Response - Confirmed ORR 64% vs 30% with chemotherapy.
Regulatory - FDA approved May 22, 2026 (Datroway) - first TROP2 ADC for 1L immunotherapy-ineligible metastatic TNBC.
Sponsor / drug - Daiichi Sankyo + AstraZeneca; datopotamab deruxtecan (Datroway).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.
The U.S. FDA approved Datroway® (datopotamab deruxtecan-dlnk) for the treatment of adult patients with unresectable or metastatic triple-negative breast cancer (TNBC) who are not candidates for PD-1/PD-L1 inhibitor therapy. Datroway is the first TROP2-directed antibody-drug conjugate approved in the first-line setting for this population. The approval was supported by the pivotal Phase III TROPION-Breast02 trial.
Safety (n=319): Serious adverse reactions in 17% of patients. Most common adverse reactions (≥20%): stomatitis, increased amylase, nausea, alopecia, decreased hemoglobin, decreased white blood cells, constipation, decreased calcium, decreased lymphocytes, fatigue, and decreased neutrophils. ILD/pneumonitis monitoring remains a DXd class consideration. No companion diagnostic is required.
Daiichi Sankyo / AstraZeneca press release ↗ · TROPION-Breast02 · Annals of Oncology ↗
OS/PFS/ORR figures per FDA-approved Datroway prescribing information / Daiichi Sankyo press release (May 22, 2026). Median PFS by BICR shown; confirmed ORR.








Trial slides shared by KOLs at ESMO Breast 2026 (#ESMOBreast26). Click any image to expand. OCR text extracted via AWS Textract.

[Slide 1] PLEASE NOTE that use of this NCCN Content IS governed by the End-User License Agreement and you MAY NOT distribute this Content or use it with any artificial intelligence model or tool. National Printed by Abirami Sivapiragasam on 1/20/2026 12:48:20 PM. Copyright © 2026 National Comprehensive Cancer Network, Inc. All Rights Reserved. NCCN Guidelines Version 1.2026 NCCN Guidelines Index Comprehensive Table of Contents NCCN Cancer Invasive Breast Cancer Discussion Network® CYTOTOXIC REGIMENS FOR RECURRENT UNRESECTABLE (LOCAL OR REGIONAL) OR STAGE IV (M1) DISEASEᵃ HR-Negative and HER2-Negative (Triple-Negative Breast Cancer; TNBC) See BINV-Q 1 of 15 for Considerations for systemic therapy. Setting Subtype/Biomarker Regimen First Line PD-L1 CPS >10 regardless of germline BRCA1/2 Chemotherapy (Albumin-bound Paclitaxel, Carboplatin/Gemcitabine, or PV statusᵇ Paclitaxel,) + Pembrolizumab (category 1, preferred) Sacituzumab govitecan-hziy + Pembrolizumab (preferred) Sacituzumab govitecan-hziy (category 1, preferred) PD-L1 CPS <10 and no germline BRCA1/2 PVᵇ Datopotamab deruxtecan-dink (other recommended) Systemic chemotherapy BINV-Q 5 of 15 PD-L1 CPS <10 and germline BRCA1/2 PVᵇ PARPi (Olaparib or Talazoparib) (category 1, preferred) Platinum (Carboplatin or Cisplatin) (category 1, preferred) Second Germline BRCA1/2 PVb PARPi (category 1, preferred) Line Sacituzumab govitecan-hziy (category 1, preferred) Any Systemic chemotherapy BINV-Q 5 of 15 or targeted agents BINV-Q 7 of 15 No germline BRCA1/2 PVᵇ and HER2 (ERBB2) IHC 1+ or 2+/ISH negatived Fam-trastuzumab deruxtecan-nxkim (other recommended)
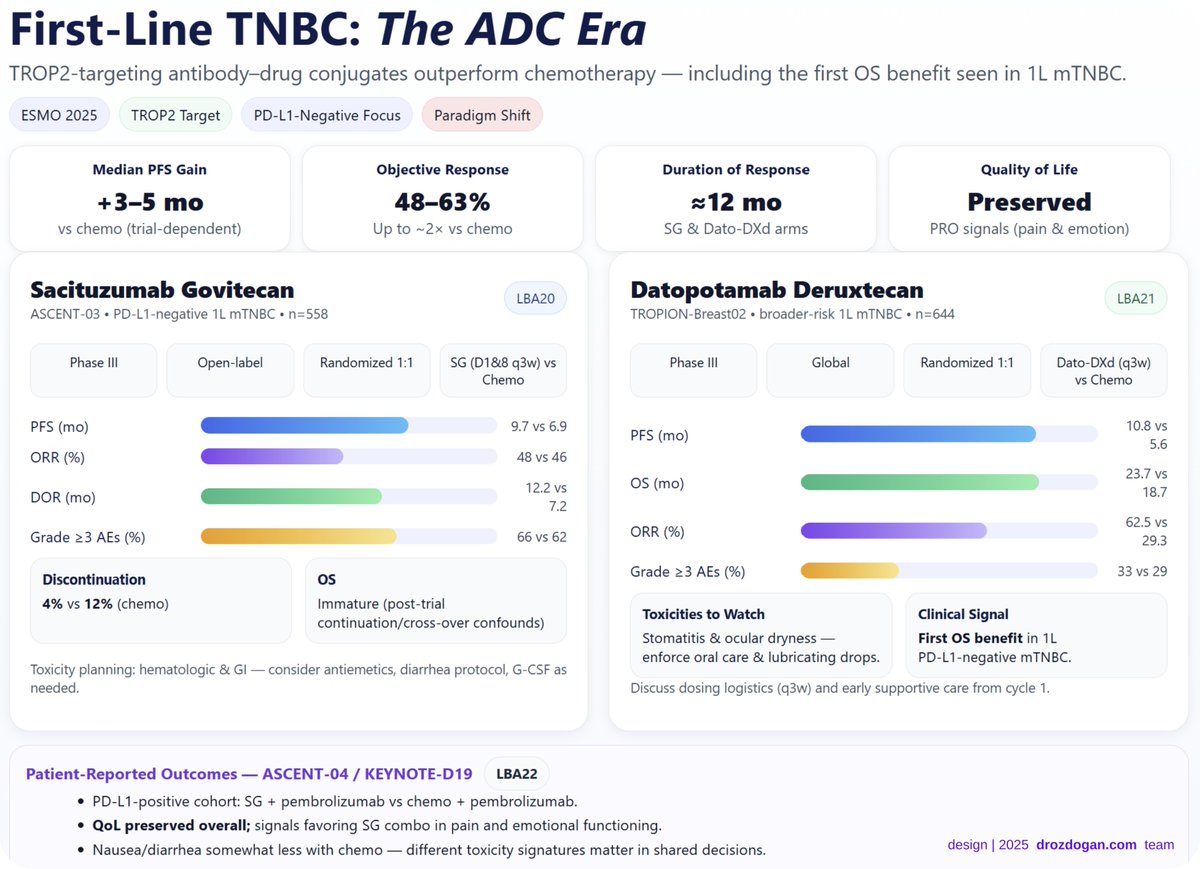
[Slide 1] First-Line TNBC: The ADC Era TROP2-targeting antibody-drug conjugates outperform chemotherapy — including the first OS benefit seen in 1L mTNBC. ESMO 2025 TROP2 Target PD-L1-Negative Focus Paradigm Shift Median PFS Gain Objective Response Duration of Response Quality of Life +3-5 mo 48-63% ≈12 ≈ mo Preserved VS chemo (trial-dependent) Up to ~2x VS chemo SG & Dato-DXd arms PRO signals (pain & emotion) Sacituzumab Govitecan LBA20 Datopotamab Deruxtecan LBA21 ASCENT-03 PD-L1-negative 1L mTNBC n=558 TROPION-Breast02 broader-risk 1L mTNBC n=644 Phase III Open-label Randomized 1:1 SG (D1&8 q3w) VS Phase III Global Randomized 1:1 Dato-DXd (q3w) Chemo VS Chemo PFS (mo) 9.7 VS 6.9 10.8 VS PFS (mo) 5.6 ORR (%) 48 vs 46 23.7 vs 12.2 VS OS (mo) DOR (mo) 18.7 7.2 62.5 VS Grade ≥3 AEs (%) 66 VS 62 ORR (%) 29.3 Discontinuation os Grade ≥3 AEs (%) 33 vs 29 4% vs 12% (chemo) Immature (post-trial Toxicities to Watch Clinical Signal continuation/cross-over confounds) Stomatitis & ocular dryness — First os benefit in 1L enforce oral care & lubricating drops. PD-L1-negative mTNBC. Toxicity planning: hematologic & GI - consider antiemetics, diarrhea protocol, G-CSF as needed. Discuss dosing logistics (q3w) and early supportive care from cycle 1. Patient-Reported Outcomes - ASCENT-04 / KEYNOTE-D19 LBA22 PD-L1-positive cohort: SG + pembrolizumab vs chemo + pembrolizumab. QoL preserved overall; signals favoring SG combo in pain and emotional functioning. Nausea/diarrhea somewhat less with chemo - different toxicity signatures matter in shared decisions. design I 2025 drozdogan.com team



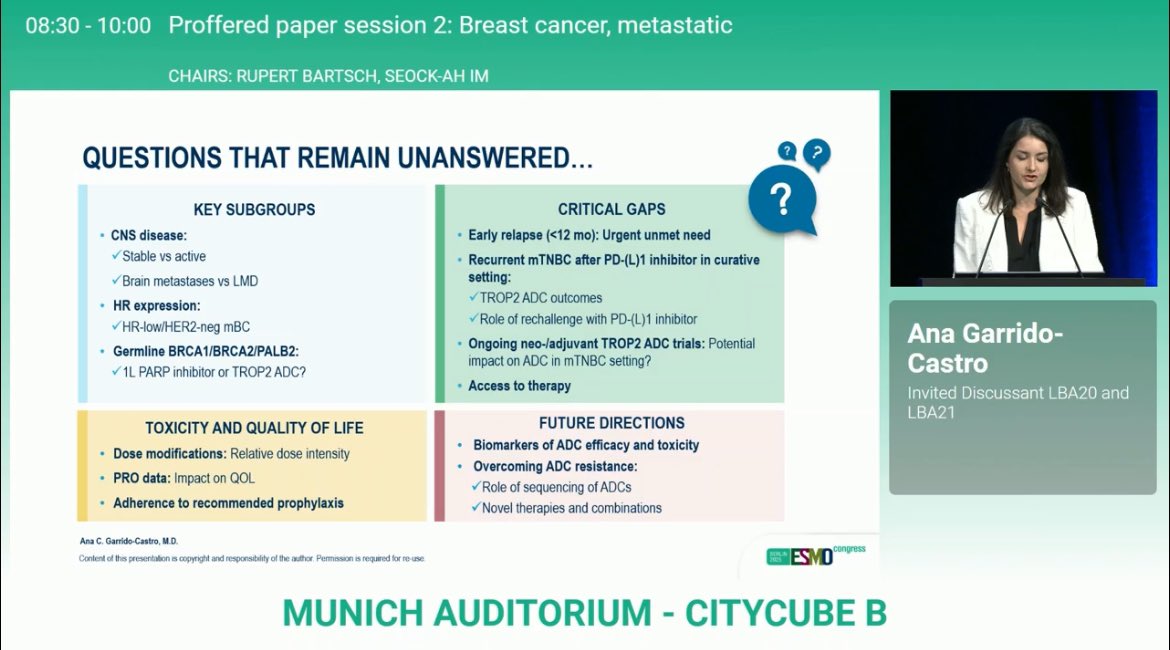
[Slide 1] 08:30 - 10:00 Proffered paper session 2: Breast cancer, metastatic CHAIRS: RUPERT BARTSCH, SEOCK-AH IM TROP2 ADC IN 1L mTNBC NOT CANDIDATE FOR aPD-(L)1 ASCENT-03 TROPION-Breast02 Sacituzumab Datopotamab govitecan (n=279) deruxtecan (n=323) (10 mg/kg IV on (6 mg/kg IV on Previously untreated, Days 1,8 of 21-day cycles) Previously untreated, Day 1 of 21-day cycles) locally advanced inoperable locally recurrent inoperable or metastatic TNBC not 1:1 or metastatic TNBC not 1:1 Ana Garrido- candidate for PD-(L)1 candidate for PD-(L)1 inhibitor *Crossover to SG allowed inhibitor ICC (n=321) Castro after BICR-verified PD paclitaxel or nab-paclitaxel Invited Discussant LBA20 and (if no prior taxane or neo-ladjuvant taxane TPC* (n=279) DFI >12 mo) OR capecitabine, LBA21 gemcitabine/carboplatin, carboplatin or eribulin Dates ESMO 2005 paclitaxel or nab-paclitaxel (if prior taxane DFI $12 mo) DFI >6 months Crossover to SG at PD Any DFI (≤12 months: 20% cap) NO crossover to Dato-DXd at PD TPC: Taxane or Primary Endpoint: PFS ICC: Taxane or Capecitabine/ Primary Endpoints (dual): Carboplatin+Gemcitabine Carboplatin/Eribulin PFS and OS Ana C. Garrido-Castro M.D. congress Content of this presentation is copyright and responsibility of the author Permission is required for re-use ESMO MUNICH AUDITORIUM - CITYCUBE B --- [Slide 2] 08:30 - 10:00 Proffered paper session 2: Breast cancer, metastatic CHAIRS: RUPERT BARTSCH, SEOCK-AH IM TRIAL DESIGN CONSIDERATIONS: THE IMPACT OF CROSSOVER Is there known benefit to the crossover therapy in a later-line setting? SG demonstrated PFS and OS benefit in 2L+ mTNBC + Are there differences in the patient population who crosses over VS not? Sensitivity analyses to evaluate robustness of OS data Is the study designed to test OS superiority? OS secondary endpoint Ana Garrido- Is there a pre-specified statistical plan to assess OS considering crossover (e.g., non-informative censoring, restricted mean survival time, IPTW)? Yes Castro Are there commercially available therapies in a later-line setting that impact OS? SG, T-DXd, eribulin Invited Discussant LBA20 and LBA21 Is there widespread access to these therapies? Approx. 60-70% participants enrolled outside of U.S./Canada/Western Europe Inclusion of crossover should be CONSIDERED for therapy with known OS advantage Assessment Overat Oncology Cince Trais - Accessed October 2125 Ana C. Garrido-Castro M.D. congress Content of this presentation is copyright and responsibility of the author Permission is required for re-use ESMO MUNICH AUDITORIUM - CITYCUBE B --- [Slide 3] 08:30 - 10:00 Proffered paper session 2: Breast cancer, metastatic CHAIRS: RUPERT BARTSCH, SEOCK-AH IM HOW TO SELECT 1L TROP2 ADC FOR A PATIENT WITH PD-L1-NEGATIVE mTNBC? Sacituzumab govitecan Datopotamab deruxtecan PFS benefit PFS benefit OS data immature (impact of crossover?) OS benefit 1 Neutropenia: G-CSF primary prophylaxis for 1 Response rate Ana Garrido- (at least) patients at increased risk of febrile 1 Ocular surface toxicity: Eye drops, avoid contact neutropenia lenses, baseline eye exam Castro 1 Nausea 1 Oral mucositis/stomatitis: Mouthwash Invited Discussant LBA20 and 1 Diarrhea ILD monitoring LBA21 Two infusions per 21-day cycle One infusion per 21-day cycle 1 Longer total infusion time 1 Shorter total infusion time Ana C. Garrido-Castro M.D. congress Content of this presentation is copyright and responsibility of the author Permission is required for re-use ESMO MUNICH AUDITORIUM - CITYCUBE B --- [Slide 4] 08:30 - 10:00 Proffered paper session 2: Breast cancer, metastatic CHAIRS: RUPERT BARTSCH, SEOCK-AH IM QUESTIONS THAT REMAIN UNANSWERED ? ? KEY SUBGROUPS CRITICAL GAPS ? CNS disease: Early relapse (<12 mo): Urgent unmet need Stable VS active Recurrent mTNBC after PD-(L)1 inhibitor in curative Brain metastases VS LMD setting: TROP2 ADC outcomes HR expression: HR-low/HER2-neg mBC Role of rechallenge with PD-(L)1 inhibitor Ana Garrido- Germline BRCA1/BRCA2/PALB2: Ongoing neo-/adjuvant TROP2 ADC trials: Potential impact on ADC in mTNBC setting? 1L PARP inhibitor or TROP2 ADC? Castro Access to therapy Invited Discussant LBA20 and LBA21 TOXICITY AND QUALITY OF LIFE FUTURE DIRECTIONS Biomarkers of ADC efficacy and toxicity Dose modifications: Relative dose intensity Overcoming ADC resistance: PRO data: Impact on QOL Role of sequencing of ADCs Adherence to recommended prophylaxis Novel therapies and combinations Ana C. Garrido-Castro, M.D. congress Content of this presentation is copyright and responsibility of the author Permission is required for re-use ESMO MUNICH AUDITORIUM - CITYCUBE B



[Slide 1] PATIENT POPULATION ASCENT-03 TROPION-Breast02 (Cortés, ESMO 2025) (Dent, ESMO 2025) SG VS TPC Dato-DXd vs ICC Positive PD-L1 0.4% 10% Negative 99.5% 90% White 64% 44% Asian 23% Race or ethnic group 44% Black 3% 4% Other/Not specified 10% 8% U.S./Canada/Western Europe 32% 37% Geographic region Other regions 68% 63% De novo mBC 31% 34% Curative treatment-free Recurrent 0-6 mo - 15% interval Recurrent 6-12 mo 21% 5% Recurrent >12 mo 48% 45% Lung 60% NR Sites Liver 27% 30% Brain 5% 10% Ana C. Garrido-Castro, M.D. NR: Not reported Content of this presentation is copyright and responsibility of the author. Permission is required for re-use BERLIN avs ESMO congress --- [Slide 2] PATIENT POPULATION ASCENT-03 TROPION-Breast02 (Cortés, ESMO 2025) (Dent, ESMO 2025) SG vs TPC Dato-DXd vs ICC Taxane 58% 57% Prior neo-/adjuvant Capecitabine* 19% 27% chemotherapy Platinum 18% 16% Prior PD-(L)1 inhibitor 4% 5% Taxane 55% 82% Carboplatin/Gemcitabine 45% - Chemotherapy selection Carboplatin - 4% No doublet CT prior to randomization Capecitabine - 2% Eribulin - 12% Median follow-up, months (range) 13.2 (<0.1-29.2) 27.5 (13.3-38.7) "In TB02, pair pynimidine analogues reported 27% in A03, prior capecitabine reported 19% Ana C. Garrido-Castro, M.D. Content of this presentation is copyright and responsibility of the author. Permission is required for re-use. BERLIN ESMO congress 2025 --- [Slide 3] TROP2 ADC IMPROVES PFS vs TPC in 1L mTNBC ASCENT-03 TROPION-Breast02 1.0 HR: 0.62 HR: 0.57 130 0.9 NO Median PFS: 2.8 mo. 0.8 Median PFS: 5.3 mo.* 82 0.7 70 6-mo PFS: 65% VS 53% 6-mo PFS: NR 0.5 Probability Progression-From Probability of PFS 0.6 62 12-mo PFS: 41% VS 24% 12-mo PFS: 46% VS 26% so 0.4 & 0.3 30 0.2 OOD 20 0.1 00 12 0 0 0 2 4 $ # 10 12 x 16 18 20 22 24 % 29 30 0 3 6 9 12 15 18 21 24 27 30 33 36 39 Time (months) - I 21/13) I I ! DATE 2/10 I INS Number at risk Time from randomisation (months) 2 an 24.00 I 10.30 18,08 NOT - : (3) was 06/118 - - N/A 21,790 V/W 7(19) 3(9) 1(w) Data-DXd 323 265 191 150 116 84 56 41 24 20 10 5 1 0 ICC 321 191 107 64 46 29 19 16 8 6 1 0 0 0 SG TPC Dato-DXd ICC Median follow-up (range), mo 13.2 (<0.1-29.2) Median follow-up (range), mo 27.5 (13.3-38.7) N PFS events (%) 349 (63) N PFS events (%) 408 (63) Median PFS (95% CI), mo 9.7 (8.1-11.1) 6.9 (5.6-8.2) Median PFS* (95% CI), mo 10.8 (8.6-13.0) 5.6 (5.0-7.0) Stratified HR (95% CI) 0.62 (0.50-0.77), P <0.0001 Stratified HR (95% CI) 0.57 (0.47-0.69), p <0.0001 Conis 108 ESMO 2028 Dont . ESMO 2028 Conis 2-m * Lancer 2022,396 1817-28 Numbers shown in table are rounded: median PFS 10.84 with Date OXd: $.55 with ICC; A529 months. Ana C. Garrido-Castro, M.D. BERLIN Content of this presentation is copyright and responsibility of the author. Permission is required for re-use. 2025 ESMO congress
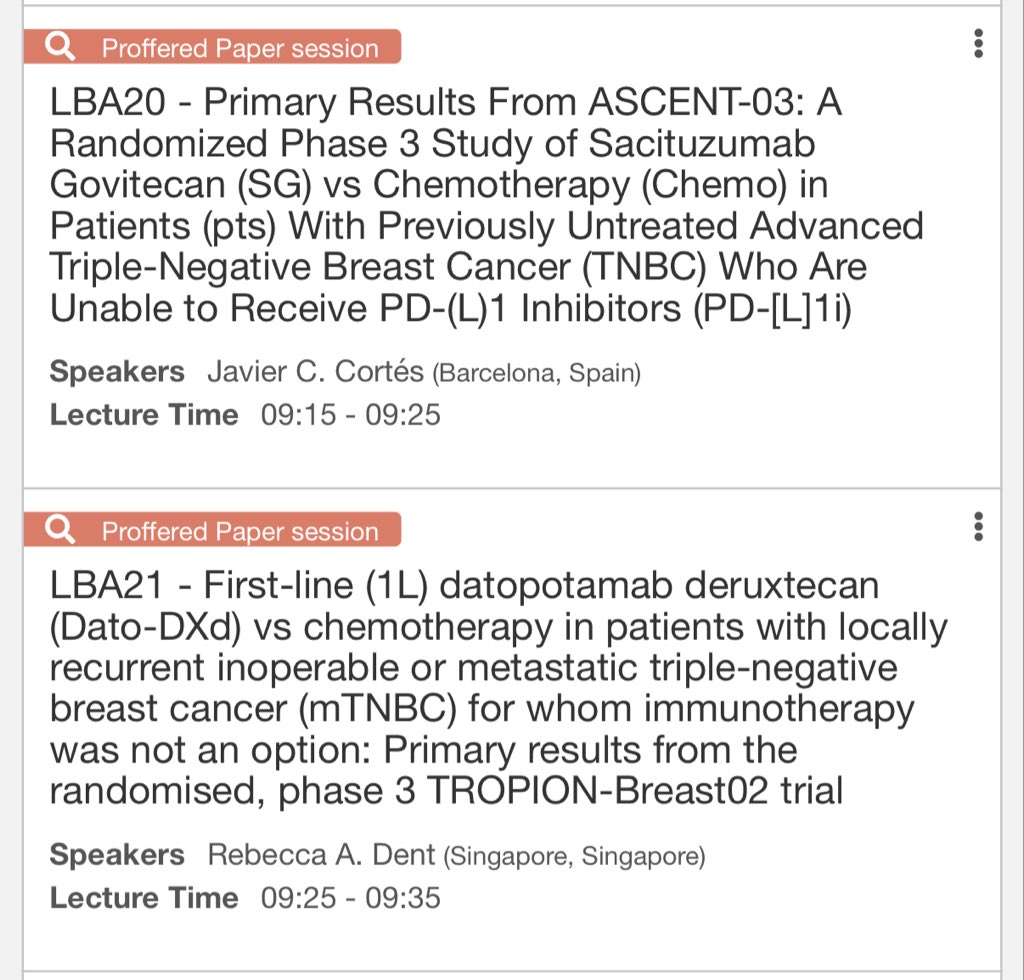
[Slide 1] Proffered Paper session LBA20 - Primary Results From ASCENT-03: A Randomized Phase 3 Study of Sacituzumab Govitecan (SG) vs Chemotherapy (Chemo) in Patients (pts) With Previously Untreated Advanced Triple-Negative Breast Cancer (TNBC) Who Are Unable to Receive PD-(L)1 Inhibitors (PD-[L]1i) Speakers Javier C. Cortés (Barcelona, Spain) Lecture Time 09:15 - 09:25 Proffered Paper session LBA21 - First-line (1L) datopotamab deruxtecan (Dato-DXd) vs chemotherapy in patients with locally recurrent inoperable or metastatic triple-negative breast cancer (mTNBC) for whom immunotherapy was not an option: Primary results from the randomised, phase 3 TROPION-Breast02 trial Speakers Rebecca A. Dent (Singapore, Singapore) Lecture Time 09:25 - 09:35
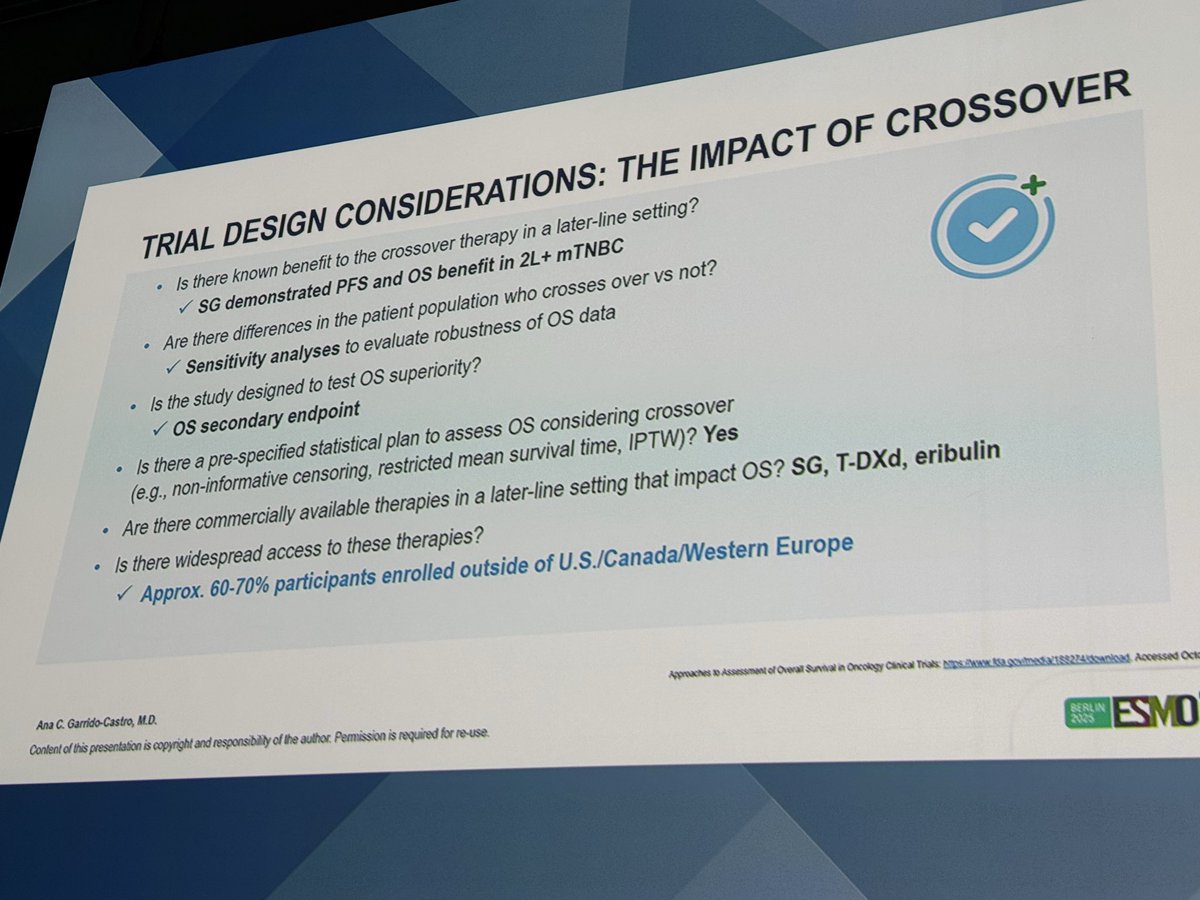
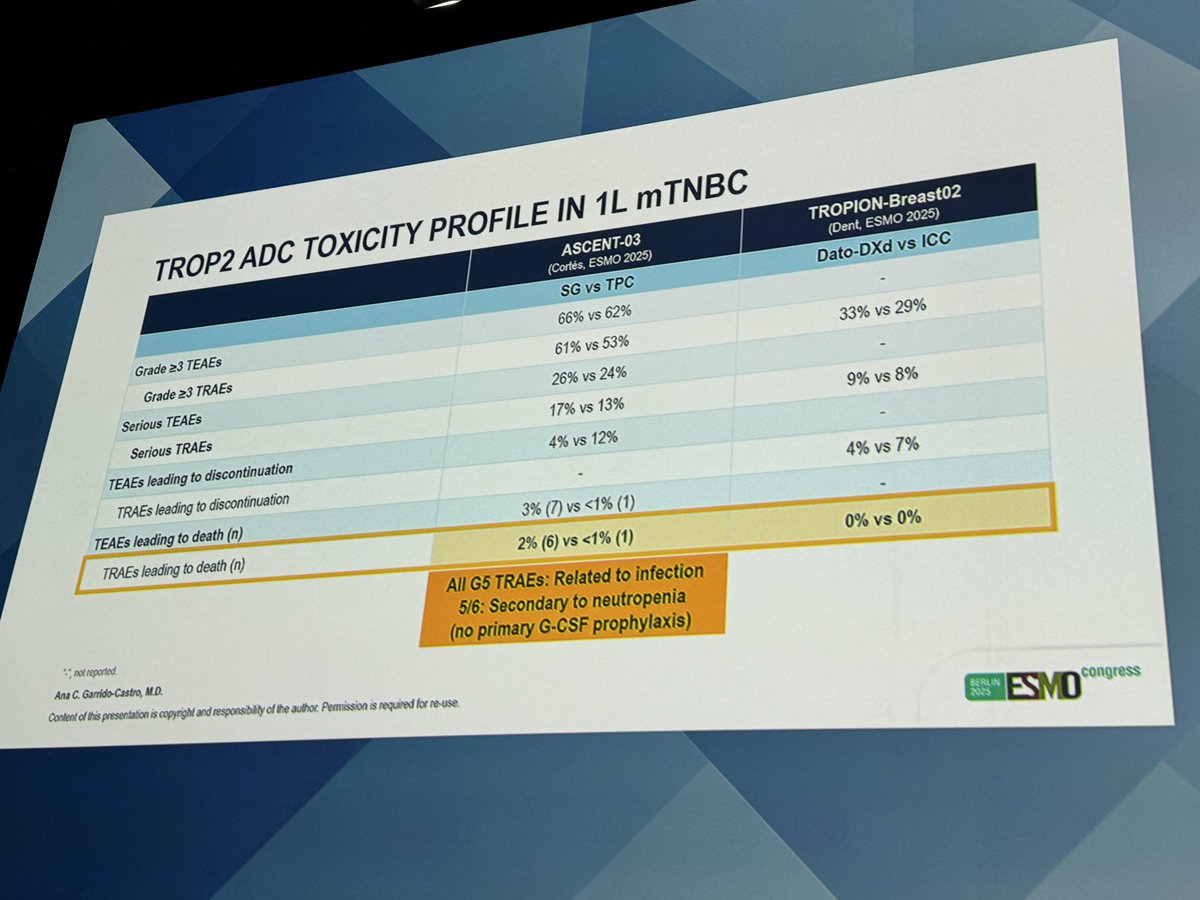
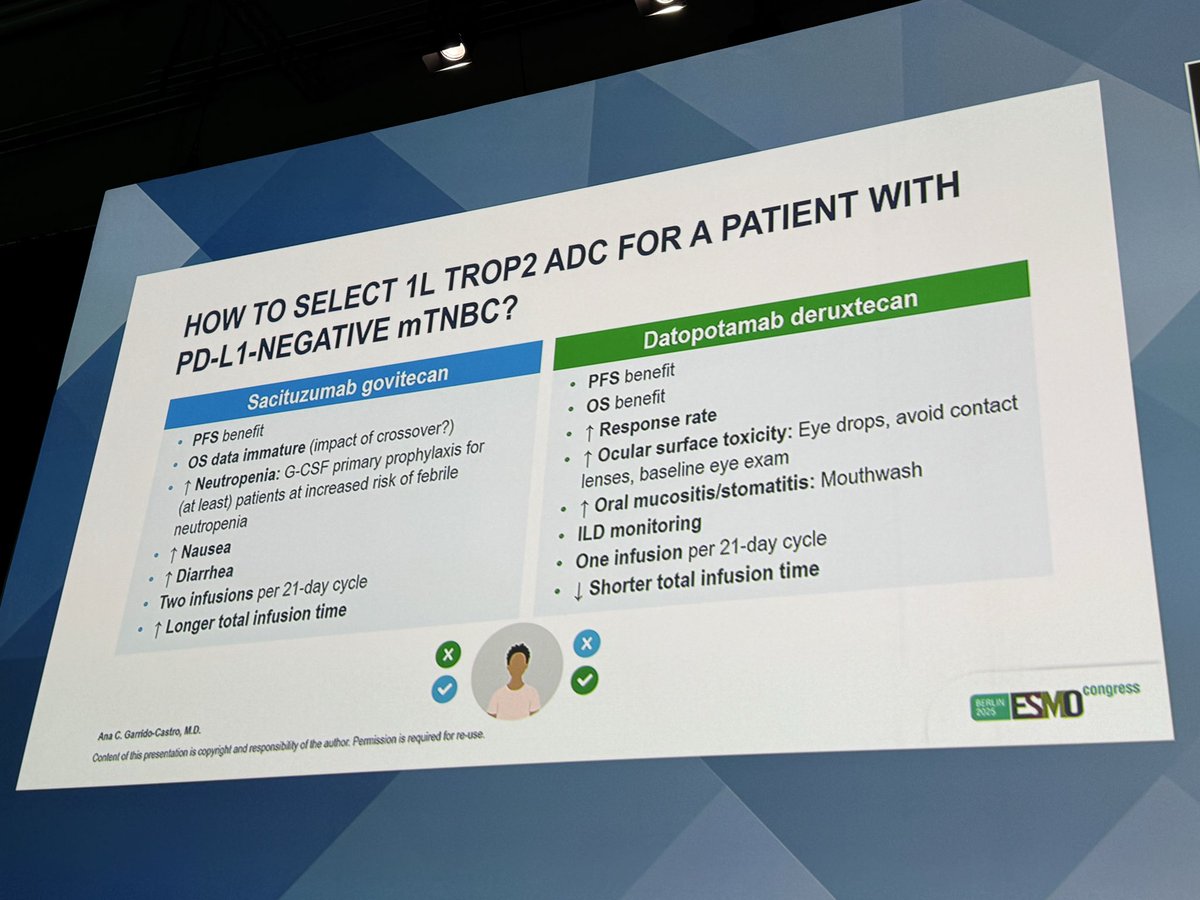
[Slide 1] TRIAL DESIGN CONSIDERATIONS: THE IMPACT OF CROSSOVER Is there known benefit to the crossover therapy in a later-line setting? SG demonstrated PFS and OS benefit in 2L+ mTNBC + Are there differences in the patient population who crosses over VS not? Sensitivity analyses to evaluate robustness of OS data Is the study designed to test OS superiority? os secondary endpoint Is there a pre-specified statistical plan to assess OS considering crossover (e.g., non-informative censoring, restricted mean survival time, IPTW)? Yes Are there commercially available therapies in a later-line setting that impact OS? SG, T-DXd, eribulin Is there widespread access to these therapies? Approx. 60-70% participants enrolled outside of U.S./Canada/Western Europe Approaches 30 Assessment of Overall Survival in Oncology Clinical Trials Accessed Oct Ana C. Garrido-Castro, M.D. Content of this presentation is copyright and responsibility of the author. Permission is required for re-use BERLIN 2025 ESMO --- [Slide 2] TROP2 ADC TOXICITY PROFILE IN 1L mTNBC ASCENT-03 TROPION-Breast02 (Cortés, ESMO 2025) (Dent, ESMO 2025) SG vs TPC Dato-DXd vs ICC Grade ≥3 TEAEs 66% VS 62% - Grade ≥3 TRAEs 61% VS 53% 33% VS 29% Serious TEAEs 26% VS 24% - Serious TRAEs 17% VS 13% 9% VS 8% TEAEs leading to discontinuation 4% VS 12% - TRAEs leading to discontinuation - 4% VS 7% TEAEs leading to death (n) 3% (7) VS <1% (1) - TRAEs leading to death (n) 2% (6) vs <1% (1) 0% vs 0% All G5 TRAEs: Related to infection 5/6: Secondary to neutropenia (no primary G-CSF prophylaxis) :- not reported Ana C. Garrido-Castro, M.D. Content of this presentation is copyright and responsibility of the author. Permission is required for re-use BERLIN 2025 ESMO congress --- [Slide 3] HOW TO SELECT 1L TROP2 ADC FOR A PATIENT WITH PD-L1-NEGATIVE mTNBC? Sacituzumab govitecan Datopotamab deruxtecan PFS benefit PFS benefit os data immature (impact of crossover?) os benefit Neutropenia: G-CSF primary prophylaxis for Response rate (at least) patients at increased risk of febrile Ocular surface toxicity: Eye drops, avoid contact neutropenia lenses, baseline eye exam Nausea Oral mucositis/stomatitis: Mouthwash Diarrhea ILD monitoring Two infusions per 21-day cycle One infusion per 21-day cycle Longer total infusion time Shorter total infusion time x x Ana C. Garrido-Castro, M.D. BERLIN Content of this presentation is copyright and responsibility of the author. Permission is required for re-use. 2025 ESMO congress à


Highest-engagement tweets about this trial, ranked by KOL discussant count (replies + quote-tweets). Replies in green, quote-tweets in blue. Wall Street, stock-promo, and non-substantive replies excluded.
Not sure of the reasoning behind the different recommendation categories for SG and Dato-DXd in PDL1- disease, despite OS advantage with Dato-DXd? 🤷♂️ https://t.co/ch5kxV8Yf5
Ah. Why is cross trial comparison inevitable among trialists/specialists? We know better. Dangerous assumption in my humble opinion. Decisions should be made based on factors such as toxicity, tolerance for individuals a

We need better algorithms/decision trees… Hopefully something we can do together.. @MedwatchKate @MedicalwatchHQ @OncoAlert @OncBrothers I find the NCCN guidelines helpful but ‘clunky’. We need something more user and mo

Agree, Dato-DXd show better OS with inclusion of a significant proportion of very high-risk patints

TB-02 is not yet published. I suspect that is reason for the different recommendation category. Once published in peer reviewed journal, I suspect it will have a similar recommendation. OS advantage differences likely ju
I was wondering about the same.

Crossover is the answer.

Spannend, wie Leitlinien unterschiedlich gewichten! Dato-DXds OS-Vorteil ist klar, aber vielleicht fehlen Langzeitdaten oder die Toxizitätsbilanz spricht für SG? #sabcs25
Interesting move in the new NCCN guidelines: ADCs are now listed as a first-line option in mTNBC, even before FDA approval. Highlights how rapidly the treatment landscape is evolving. #sabcs25 @ASCO @SABCSSanAntonio #MedTwitter @OncBrothers @TotalHealthConf @PTarantinoMD https://

FDA approval represents a legal endpoint. NCCN guidelines, by contrast, serve as a framework for clinical decision-making. The inclusion of a drug in NCCN guidelines prior to FDA approval is not an exception but a delibe

Big pharma bribing NCCN.

The guidelines for melanoma are also changing so rapidly with immunotherapy being the go to treatment for advanced staged or unresectable tumors!

Thank you for sharing

https://t.co/bBcotw4cTT Here's the data provided to NCCN to make the decision pre-approval
Fantastic highlights of the diff between #ASCENT03 and #TB02 In TB-02: 📍poorer prognosis pts, 15% relapsed within 6 mo of neoadj/adj thpy 📍no doublet chemo 📍no crossover to ADC 📍dato didn't look to have OS in areas where there wasTROP2 ADC access #ESMO25 #ESMOAmbassadors http
Fantastic discussion by Dr. Garrido-Castro @DFCI_BreastOnc on TROP-2 ADC presentations. We have 2 highly efficacious TROP-2 ADCs with some differences. Side effect profile, ORR, schedule etc will all come into play 👩

Agree. 2 adcs that have improved activity compared with chemo in 1st line tnbc. Pick your favorite and use it as soon as it gets approved instead of chemo. For pdl1 pos use sg with pembro.







 +4
+4
It’s official: ASCENT-03 and TROPION-Breast02 will be both presented at #ESMO25. Two positive trials, taking Trop2 ADCs to the 1L and improving outcomes for one of the greatest unmet needs in breast oncology — metastatic TNBC. Discussion by Ana Garrido-Castro @DFCI_BreastOnc. htt

Looking forward to these presentations

Dr Paolo, Whats your take on Trop2 testing and immunopet prior to datodxd? Is it done regularly out of trials/in practice? Would it be a new biomarker to guide therapy?

https://t.co/TSkdzp5pdj
Paradigm Shift in 1L TNBC We may be witnessing the end of chemotherapy’s monopoly in PD-L1–negative metastatic TNBC. Dato-DXd delivers the first OS benefit in this setting. SG shows a robust PFS advantage and prolonged DOR ≈ 12 mo. Next frontier → sequencing & chemo-free http







 +4
+4
At #ESMO25 Ana Garrido-Castro discusses results of ASCENT-03 and TROPION-Breast02 🔸Crossover was allowed in Ascent, but not in TB02, potentially impacting OS 🔸Pts with more aggressive disease included in TB02 ➡️choice to be guided by safety profile of each ADC? @OncoAlert https:
I think choice can be guided by the safety profile and infusion schedule. Personally the ORR of Dato-Dxd was quite higher in a higher risk population. https://t.co/CW0AZAKuxw
8. #TROPIONBreast02: Ph III, 1L mTNBC in PDL1 negative or IO ineligible, DatoDXd vs. Chemo. - mPFS 10.8 vs 5.6 mos (HR: 0.57) - mOS 23.7 vs. 18.7 mos (HR: 0.79) - ORR 62.5% vs. 29.3% - AEs: mucositis and occular toxic







 +4
+4TROPION-Breast02 is a global Phase III randomized open-label trial evaluating first-line datopotamab deruxtecan (Dato-DXd, Datroway — TROP2-targeting ADC with DXd payload) versus investigator's choice chemotherapy (ICC) in patients with locally recurrent inoperable or metastatic triple-negative breast cancer (TNBC) for whom immunotherapy is not an option. Primary results presented at ESMO 2025 (LBA21) demonstrated statistically significant and clinically meaningful improvements in both PFS and OS, supporting Dato-DXd as a new first-line standard of care in this population. At ESMO Breast 2026, PRO data confirmed substantial QoL preservation.
Population: Adults with locally recurrent inoperable or metastatic TNBC, no prior chemotherapy or targeted therapy in metastatic setting, ECOG 0-1, immunotherapy not considered an appropriate option (e.g., PD-L1 negative or contraindicated).
Interventions: Dato-DXd 6 mg/kg IV every 3 weeks. Investigator's choice chemotherapy: paclitaxel, nab-paclitaxel, capecitabine, eribulin, or carboplatin per investigator selection.
Endpoints: Dual primary: PFS by BICR; OS in ITT. Secondary: ORR, DoR, safety, patient-reported outcomes (PROs).
PFS by BICR: HR 0.57 (p<0.0001); 12-month PFS rate 45.6% vs 25.6%; 18-month 32.7% vs 16.8%. Investigator-assessed PFS: 9.6 vs 5.2 months (HR 0.56). OS: median 23.7 months Dato-DXd (95% CI 19.8-25.6) vs 18.7 months ICC (95% CI 16.0-21.8); HR 0.79 (95% CI 0.64-0.98; p=0.0291) — 21% reduction in death risk. 12-mo OS 75.2% vs 67.8%; 18-mo 61.2% vs 51.3%. Confirmed ORR 62.5% vs 29.3% (Δ33.2%). Median DoR 12.3 vs 7.1 months. PRO update at ESMO Breast 2026: median TTD global health 23.5 vs 8.3 months (HR 0.64); arm symptoms HR 0.51; physical function HR 0.67.
Treatment duration was substantially longer with Dato-DXd vs ICC, yet PROs consistently favoured Dato-DXd across global health, physical functioning, arm symptoms, and pain domains. Safety profile consistent with prior Dato-DXd experience: stomatitis, nausea, fatigue, alopecia. ILD/pneumonitis monitoring critical (DXd-class effect). Patient-reported symptomatic AEs aligned with clinician-reported safety.
Mutlu Demiray (@ozdogan_md) framed the readout as a “Paradigm Shift in 1L TNBC” in which the field “may be witnessing the end of chemotherapy’s monopoly in PD-L1–negative metastatic TNBC,” noting “Dato-DXd delivers the first OS benefit in this setting” while “SG shows a robust PFS advantage and prolonged DOR ≈ 12 mo.” Erika Hamilton drew the head-to-head contrast with ASCENT-03, noting TROPION-Breast02 had “poorer prognosis pts, 15% relapsed within 6 mo of neoadj/adj thpy,” “no doublet chemo,” and “no crossover to ADC.” Paolo Tarantino flagged a discordance in guideline interpretation: “Not sure of the reasoning behind the different recommendation categories for SG and Dato-DXd in PDL1- disease, despite OS advantage with Dato-DXd?” Elisa Agostinetti relayed discussant Ana Garrido-Castro’s ESMO 2025 side-by-side comparison of ASCENT-03 and TROPION-Breast02, noting that crossover was allowed in ASCENT-03 but not in TROPION-Breast02 — potentially impacting OS — and that TROPION-Breast02 enrolled patients with more aggressive disease. Garrido-Castro framed the practical takeaway as a choice to be guided by the safety profile of each ADC.
TROPION-Breast02 is a Phase 3 randomized trial (NCT05374512) of datopotamab deruxtecan (Datroway, a TROP2-directed antibody-drug conjugate) versus investigator's choice of chemotherapy as first-line treatment for unresectable or metastatic triple-negative breast cancer in patients who are not candidates for PD-1/PD-L1 immunotherapy. It enrolled 644 patients (323 versus 321).
Datopotamab deruxtecan significantly improved both endpoints: median progression-free survival was 10.8 versus 5.6 months (HR 0.57; 95% CI 0.47-0.69; P<0.0001), and median overall survival was 23.7 versus 18.7 months (HR 0.79; 95% CI 0.64-0.98; P=0.0290). The confirmed overall response rate was 64% versus 30% with chemotherapy. This was the first time a targeted therapy showed a significant overall-survival advantage over chemotherapy in this population.
Yes. On May 22, 2026 the FDA approved datopotamab deruxtecan (Datroway) for adults with unresectable or metastatic triple-negative breast cancer who are not candidates for PD-1/PD-L1 inhibitor therapy and who have not received prior chemotherapy or systemic therapy for metastatic disease. It is the first TROP2-directed antibody-drug conjugate approved in this first-line, immunotherapy-ineligible metastatic TNBC setting.
The approval applies to first-line unresectable or metastatic triple-negative breast cancer in patients who are not candidates for PD-1/PD-L1 inhibitor therapy - for example, those with PD-L1-low tumors or contraindications to immunotherapy - and who have not yet received chemotherapy or other systemic therapy for metastatic disease.
The safety profile was consistent with prior datopotamab deruxtecan experience, with stomatitis/oral mucositis, nausea, fatigue, and alopecia among the most common events, and interstitial lung disease/pneumonitis requiring monitoring. Despite longer treatment duration than chemotherapy, patient-reported outcomes consistently favored datopotamab deruxtecan across global health, physical functioning, arm symptoms, and pain.
