TRITON Key Takeaways
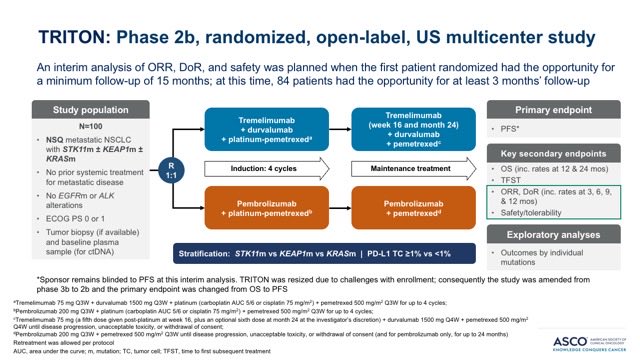
Design - Phase 2b randomized US study: tremelimumab + durvalumab + chemo vs pembrolizumab + chemo, 1L non-squamous NSCLC with STK11/KEAP1/KRAS mutations (NCT06008093; AstraZeneca; n=84; PI F. Skoulidis, MD Anderson).
PFS (primary - BLINDED) - The primary endpoint of progression-free survival remained blinded to the sponsor at this ASCO 2026 interim analysis; data too immature to evaluate.
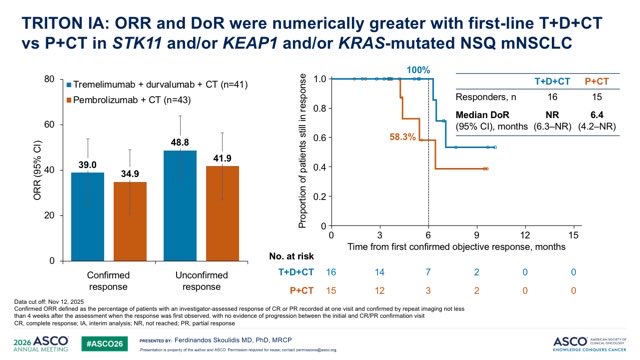
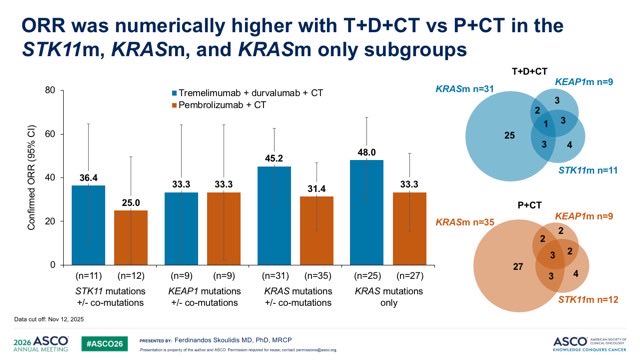
ORR (secondary) - Confirmed ORR 39.0% (T+D+chemo) vs 34.9% (pembro+chemo), overlapping confidence intervals; in the prespecified KRAS-mutant subgroup 48.0% vs 33.3%.
DoR (secondary) - Median duration of response not reached (T+D+chemo) vs 6.4 months (pembro+chemo); at the 6-month landmark 100% vs 58.3% of responders remained in response - the most differentiated efficacy signal.
Safety - Grade 3/4 adverse events broadly comparable: 41.5% (T+D+chemo) vs 41.9% (pembro+chemo).
Regulatory - Investigational; primary PFS blinded. Sponsor AstraZeneca; tremelimumab (Imjudo) + durvalumab (Imfinzi).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.
KOLs Discussing TRITON
TRITON Key Slides & Visuals
Slides shared by KOLs at ASCO 2026 (Rapid Oral Abs 8515, presented by @FSkoulidis). Click any image to expand.
























Top Tweets on TRITON

Day 2 #ASCO26 highlights: Breast Cancer: 1. #KN522 (update): IO + Chemo TNBC 2. #OPTIMA: Adj Chemo HR+ 3. #lidERA: Adj SERD HR+ 4. #SENOMAC: ALND omission Prostate Ca 5. #TALAPRO3: PARPi NSCLC: 6. #TRITON: Dual ICI mNSCLC #OncTwitter @ASCO @OncoAlert 1/7 https://t

Alright. Abstracts are out. This is one of the studies I really wanted to see… and I’m disappointed. TRITON IA (T+D+CT vs P+CT, STK11/KEAP1/KRAS NSQ mNSCLC): only ORR + DoR reported, PFS still blinded. ORR within noise (39% vs 35%) but durability intriguing (100% vs 58% in https:

🆙 #ASCO26 #LCSM Rapid Oral 🔥TRITON: Tremelimumab + durvalumab + CT vs pembro + CT in 1L NSQ NSCLC with STK11, KEAP1, and/or KRAS mut ✅ORR 39% vs 34.9% ✅KRAS: ORR 48% vs 33.3% 🎙️ @FSkoulidis 🔢8515 ☑️NCT06008093 🔗 https://t.co/XCafTEYOfG @OncoAlert @Larvol @ASCO @KRASKickers https:

#ASCO26 #TRITON @FSkoulidis I’m struggling to understand the value of highlighting secondary endpoints while the primary endpoint remains blinded. The reported improvements in ORR and DoR for tremelimumab + durvalumab + chemotherapy versus pembrolizumab + chemotherapy are https:

Dr. @FSkoulidis presents randomized phase 2b TRITON study at #ASCO26: chemo + durvalumab + tremelimumab vs chemo + pembro in non-squamous NSCLC with STK11, KEAP1, and/or KRAS mutations. RR numerically favors dual checkpoint in the challenging STK11 and KRAS subsets. PFS pending.

🚨 #ASCO26 | TRITON interim analysis Tremelimumab + durvalumab + chemo vs pembrolizumab + chemo 1L NSQ mNSCLC with STK11/KEAP1/KRAS mutations #️⃣Abstr 8515 🧬 Phase 2b randomized US study T+D+CT n=41 vs P+CT n=43 IA focused on ORR, DoR, and safety 🎯 Response: ・cORR 39.0% vs https

🫁 #ASCO26 TRITON asks the uncomfortable question in 1L NSCLC: Can CTLA-4 rescue the “cold” STK11/KEAP1/KRAS-mutant subgroup? 👀 📌 Phase 2b, n=84 📌 1L non-squamous mNSCLC 📌 STK11 and/or KEAP1 and/or KRAS mutated ⚔️ T+D+chemo vs pembro+chemo 📊 Key signal: ✅ ORR: 39.0% vs https:/

✅ Some NSCLC subgroups continue to challenge our current immunotherapy strategies more than others. At #ASCO26, the TRITON study explores whether adding anti-CTLA-4 can improve outcomes in STK11-, KEAP1-, and KRAS-mutated nonsquamous mNSCLC — a population often associated ht

New data from the phase 2b TRITON study suggest that adding tremelimumab to durvalumab + chemotherapy may improve response outcomes in patients with STK11-, KEAP1-, and/or KRAS-mutated metastatic non-squamous NSCLC. Presented by Dr. Ferdinandos Skoulidis at #ASCO26, interim http

TRITON IA: in 1L NSQ mNSCLC with STK11/KEAP1/KRAS alterations, Tremelimumab+Durvalumab+CT showed generally numerically higher ORRs vs Pembro+CT. Eagerly awaiting further data including PFS/OS. #ASCO26 https://t.co/oi38QjJXnJ

TRITON study at #ASCO26: chemo + durva + treme vs chemo + pembro in non-squamous NSCLC w/ STK11, KEAP1, and/or KRAS mutations. ⬆️ORR w/ dual ICI, except KEAP1-mutant outcomes appear similar. Small pt #’s & overlapping co-mutations make these exploratory signals. PFS pendin

😳TIL you can present a Kaplan Meier curve @ASCO with confidence intervals wide as an ocean, number at risk < 20 in both groups, & primary endpoint unknown.
Overview
TRITON (NCT06008093) is a Phase 2b randomized U.S. trial testing whether dual checkpoint blockade with tremelimumab (anti-CTLA-4) + durvalumab (anti-PD-L1) + platinum chemotherapy outperforms pembrolizumab + chemotherapy as first-line treatment in non-squamous metastatic NSCLC patients carrying STK11, KEAP1, and/or KRAS mutations — a subgroup historically associated with poor response to single-agent anti-PD-1 therapy. The trial is led by Ferdinandos Skoulidis, MD PhD (MD Anderson). Interim analysis was presented as a Rapid Oral at #ASCO26 (Abstract 8515) on May 30, 2026; the primary endpoint of PFS remains blinded.
Study Design
Phase 2b randomized, open-label U.S. trial. 84 patients randomized at the November 2025 data cut-off (full target enrollment 100 per CT.gov). Primary endpoint PFS remains blinded at this interim analysis.
Population
Treatment-naïve metastatic non-squamous NSCLC with STK11, KEAP1, and/or KRAS mutations — a population historically resistant to anti-PD-1 monotherapy and chemo-IO combos.
Intervention
Experimental: Tremelimumab + Durvalumab + platinum-pemetrexed chemo. Control: Pembrolizumab + platinum-pemetrexed chemo.
Endpoints (per CT.gov)
Primary: PFS (randomized; 6-mo; 12-mo) — BLINDED at IA. Secondary: OS (12/24-mo; overall + mutation subset), ORR, DoR, TFST, AEs. Interim reported ORR, DoR, and Grade 3/4 AE rates.
Reported Interim Results
Objective Response Rate (Secondary)
Confirmed ORR was 39.0% with T+D+CT vs 34.9% with P+CT (95% CI 24.1–54.0 vs 20.6–49.1 — single-source OncUpdates) — confidence intervals overlap substantially in the overall population. In the prespecified KRAS-mutant subgroup, ORR was 48.0% vs 33.3%, numerically favoring the dual-checkpoint arm. STK11- and KEAP1-only subgroup ORRs were reported on the Skoulidis slide but are not in any indexed public recap and should be read from the slide deck above.
Overall ORR 39.0% vs 34.9% · KRAS subset 48.0% vs 33.3%Sources: OncoDaily TRITON oncolibrary · OncUpdates ASCO 2026 preview (Skoulidis Abs 8515) — both confirm overall ORR; KRAS subset confirmed by OncoDaily; CIs single-source OncUpdatesDuration of Response (Secondary)
Median DoR was not reached (NR) with T+D+CT vs 6.4 months with P+CT. At the 6-month landmark, 100% of responders in the T+D+CT arm remained in response vs 58.3% in the P+CT arm — the most differentiated efficacy signal in the interim readout. Both numbers are independently confirmed across two sources.
Median DoR NR vs 6.4 mo · 6-mo landmark 100% vs 58.3%Sources: OncoDaily TRITON oncolibrary · OncUpdates ASCO 2026 preview — dual-confirmedProgression-Free Survival (Primary — BLINDED)
The primary endpoint of PFS remains blinded to the sponsor at this interim analysis — the data are too immature to evaluate. Per ClinicalTrials.gov, the trial's primary endpoints are PFS in randomized participants, PFS at 6 months, and PFS at 12 months. As @GlopesMd noted: "ORR within noise (39% vs 35%) but durability." @Alfdoc2 flagged the limit of interpreting secondary endpoints while PFS is blinded.
PFS BLINDED at interim · primary endpoint per CT.govSources: OncoDaily · OncUpdates · ClinicalTrials.gov NCT06008093 — all confirm PFS is primary and blinded at IAOverall Survival (Secondary — Immature)
OS data are too immature to evaluate at this interim. OS at 12 and 24 months — both overall and in the STK11/KEAP1/KRAS mutation subset — are prespecified secondary endpoints per ClinicalTrials.gov. (Note: one secondary source — GeneOnline — incorrectly labels OS as the trial's primary endpoint; CT.gov, OncoDaily, OncUpdates, and the AstraZeneca ASCO 2026 schedule all confirm PFS is primary.)
OS Not reported at IA · immatureSources: ClinicalTrials.gov NCT06008093 · OncoDaily · OncUpdatesSafety & Tolerability
Grade 3/4 adverse events were broadly comparable between arms: 41.5% with T+D+CT vs 41.9% with P+CT (dual-confirmed). Additional safety detail (single-source OncoDaily): treatment-related AEs leading to discontinuation 2.4% vs 4.7%; treatment-related deaths 0% vs 2.3%. Specific immune-mediated AE rates are not in any indexed source and should be read from the Skoulidis slide deck above. KOL recaps from @SuyogCancer, @HHorinouchi, @M_Torasawa describe safety as "broadly comparable" between arms.
G3/4 AEs 41.5% vs 41.9% · TRAE d/c 2.4% vs 4.7% · TRAE deaths 0% vs 2.3%Sources: OncoDaily TRITON oncolibrary (TRAE discontinuation + deaths — single-source) · OncUpdates ASCO 2026 preview (G3/4 AEs — dual-confirmed)TRITON FAQ
What is the TRITON trial?
TRITON (NCT06008093) is a Phase 2b randomized US study, sponsored by AstraZeneca, comparing tremelimumab plus durvalumab plus chemotherapy against pembrolizumab plus chemotherapy as first-line treatment of non-squamous non-small cell lung cancer with STK11, KEAP1, and/or KRAS mutations - a subgroup historically resistant to immunotherapy. The principal investigator is Ferdinandos Skoulidis (MD Anderson).
What did the TRITON interim analysis show?
At the ASCO 2026 interim analysis (Abstract 8515), confirmed objective response rate was 39.0% with tremelimumab-durvalumab-chemotherapy versus 34.9% with pembrolizumab-chemotherapy (overlapping confidence intervals), and 48.0% versus 33.3% in the prespecified KRAS-mutant subgroup. Median duration of response was not reached versus 6.4 months, with 100% versus 58.3% of responders still in response at 6 months. The primary endpoint of progression-free survival remained blinded.
Is the TRITON regimen FDA approved?
No. TRITON is an investigational Phase 2b trial and its primary endpoint (progression-free survival) is still blinded, so the tremelimumab-durvalumab-chemotherapy regimen is not FDA approved in this first-line NSCLC setting. Tremelimumab (Imjudo) and durvalumab (Imfinzi) are approved in other indications.
Why is the STK11/KEAP1/KRAS-mutant population important?
Non-squamous NSCLC with STK11, KEAP1, and/or KRAS mutations has historically responded poorly to standard PD-1/PD-L1-based immunotherapy. TRITON tests whether adding the anti-CTLA-4 antibody tremelimumab to durvalumab plus chemotherapy can improve outcomes in this immunotherapy-resistant subgroup versus pembrolizumab plus chemotherapy.
What are the safety findings so far?
At the interim analysis, grade 3/4 adverse events were broadly comparable between arms: 41.5% with tremelimumab-durvalumab-chemotherapy versus 41.9% with pembrolizumab-chemotherapy. Additional single-source detail reported treatment-related discontinuations of 2.4% versus 4.7% and no treatment-related deaths in the experimental arm versus 2.3% in the comparator.




