Phase 3 trial of sacituzumab tirumotecan (sac-TMT; SKB264 / MK-2870) — a TROP2-directed antibody-drug conjugate — plus pembrolizumab vs pembrolizumab monotherapy as first-line therapy for advanced PD-L1-positive NSCLC. Presented at ASCO 2026: the first Phase 3 of an ADC + immune-checkpoint inhibitor combination to meet its primary PFS endpoint in first-line NSCLC.
USA
UJSF
2026ASCO
ANNUAL MEETING
---
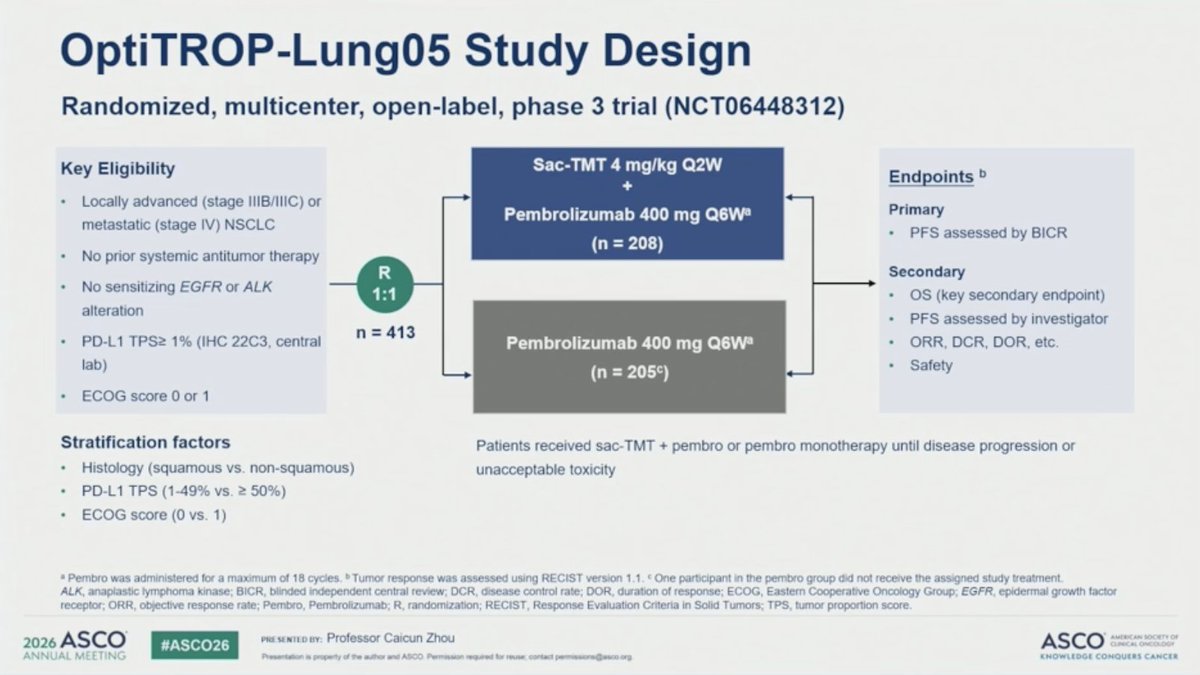
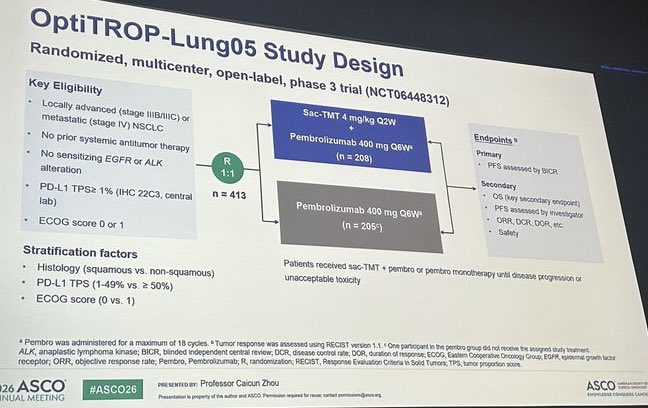
OptiTROP-Lung05 Study Design
Randomized, multicenter, open-label, phase 3 trial (NCT06448312)
Key Eligibility
Sac-TMT 4 mg/kg Q2W
Endpoints b
+
Locally advanced (stage IIIB/IIIC) or
metastatic (stage IV) NSCLC
Pembrolizumab 400 mg Q6Wa
Primary
PFS assessed by BICR
(n = 208)
No prior systemic antitumor therapy
R
Secondary
No sensitizing EGFR or ALK
1:1
OS (key secondary endpoint)
alteration
PFS assessed by investigator
n = 413
PD-L1 TPS≥ 1% (IHC 22C3, central
Pembrolizumab 400 mg Q6W
ORR, DCR, DOR, etc.
lab)
(n = 205°)
Safety
ECOG score 0 or 1
Stratification factors
Patients received sac-TMT + pembro or pembro monotherapy until disease progression or
Histology (squamous vs. non-squamous)
unacceptable toxicity
PD-L1 TPS (1-49% vs. ≥ 50%)
ECOG score (0 VS. 1)
Pembro was administered for a maximum of 18 cycles. Tumor response was assessed using RECIST version 1.1. One participant in the pembro group did not receive the assigned study treatment.
ALK, anaplastic lymphoma kinase; BICR, blinded independent central review; DCR, disease control rate; DOR, duration of response; ECOG, Eastern Cooperative Oncology Group; EGFR, epidermal growth factor
receptor; ORR, objective response rate; Pembro, Pembrolizumab; R, randomization; RECIST, Response Evaluation Criteria in Solid Tumors; TPS, tumor proportion score.
2026 ASCO
PRESENTED BY: Professor Caicun Zhou
#ASCO26
ASCO
AMERICA AN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for - contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
PFS by Investigator
Sac-TMT + pembro improved PFS vs. pembro, with a 62% reduction in risk of disease progression or death
100
Sac-TMT + Pembro
Pembro
(n = 208)
(n = 205)
80
PFS events, n (%)
69 (33.2)
124 (60.5)
Progression-Free Survival (%)
Median, mo (95% CI)
NR (11.2, NE)
6.6 (5.5, 8.2)
57.3%
60
HR 0.38 (95%CI: 0.28, 0.51)
40
27.4%
20
Sac-TMT+Pembro
Pembro
+
Censored
0
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
Time (Months)
No.at risk
Sac-TMT+Pembro
208
208
194
184
181
169
146
128
122
94
63
46
18
17
0
Pembro
205
193
154
134
128
112
87
71
66
51
32
28
10
9
1
0
2026 ASCO
PRE SENTED BY: Professor Caicun Zhou
#ASCO26
ASCO
AMERICAN SOCIETY OF
CURICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for result, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
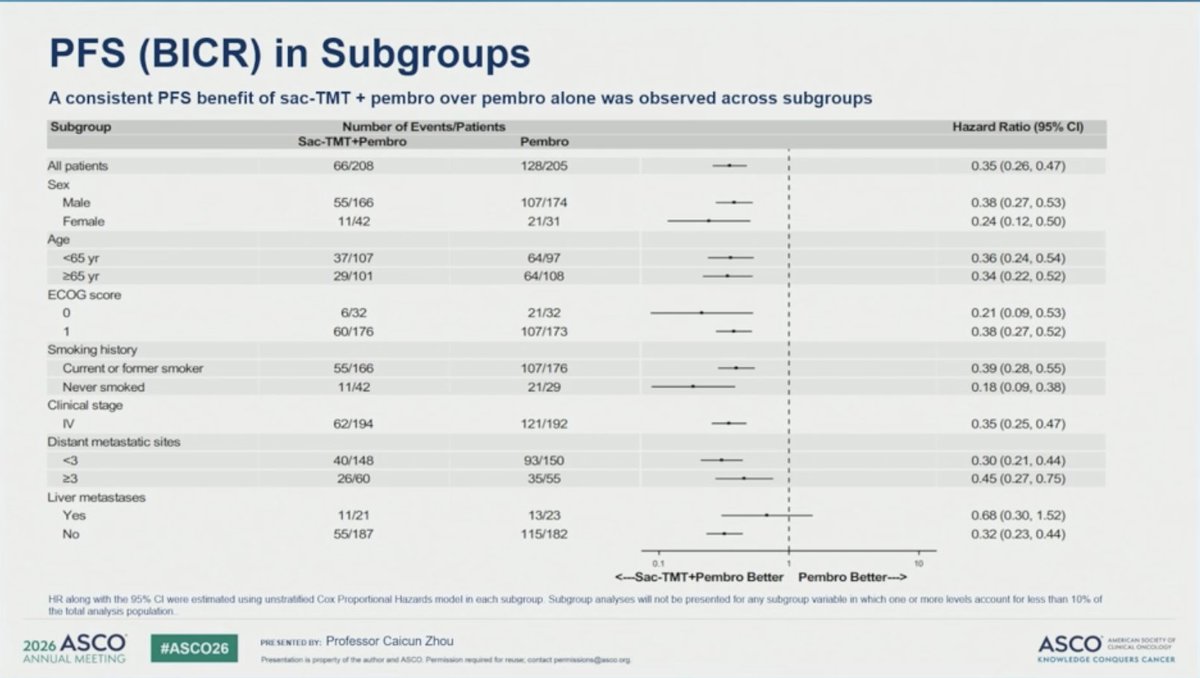
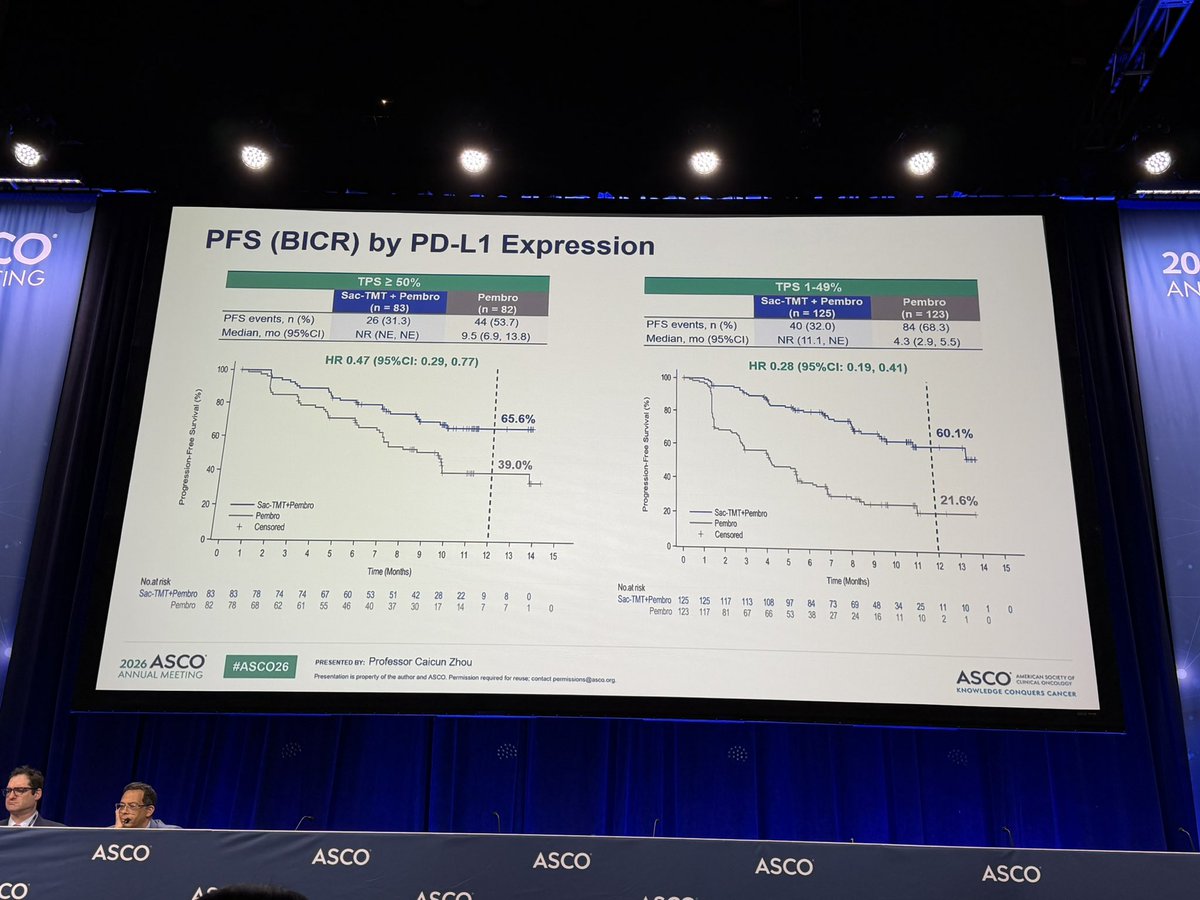
PFS (BICR) in Subgroups
A consistent PFS benefit of sac-TMT + pembro over pembro alone was observed across subgroups
Subgroup
Number of Events/Patients
Hazard Ratio (95% CI)
Sac-TMT+Pembro
Pembro
All patients
66/208
128/205
0.35 (0.26, 0.47)
Sex
Male
55/166
107/174
0.38 (0.27, 0.53)
Female
11/42
21/31
0.24 (0.12, 0.50)
Age
<65 yr
37/107
64/97
0.36 (0.24, 0.54)
>65 yr
29/101
64/108
0.34 (0.22, 0.52)
ECOG score
0
6/32
21/32
0.21 (0.09, 0.53)
1
60/176
107/173
0.38 (0.27, 0.52)
Smoking history
Current or former smoker
55/166
107/176
0.39 (0.28, 0.55)
Never smoked
11/42
21/29
0.18 (0.09, 0.38)
Clinical stage
IV
62/194
121/192
0.35 (0.25, 0.47)
Distant metastatic sites
a
40/148
93/150
0.30 (0.21, 0.44)
>3
26/60
35/55
0.45 (0.27, 0.75)
Liver metastases
Yes
11/21
13/23
0.68 (0.30, 1.52)
No
55/187
115/182
0.32 (0.23, 0.44)
0.1
to
<~Sac-TMT+Pembro Better
Pembro Better
HR along with the 95% CI were estimated using unstratified Cox Proportional Hazards model in each subgroup Subgroup analyses will not be presented for any subgroup variable in which one or more levels account for less than 10% of
the total analysis population
2026 ASCO
PRESENTED BY: Professor Caicun Zhou
#ASCO26
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact pennissions@asco.org
KNOWLEDGE CONQUERS CANCER
ASCO26
LUNG
CANCER
OncoAlert
360°
TOP TEN BY ONCOALERT
Oncology
For Collegues
By Colleagues
LBA4
HARMONI-6: IVONESCIMAB + CHEMO VS TISLELIZUMAB + CHEMO IN PREVIOUSLY UNTREATED
ADVANCED SQUAMOUS NSCLC - OS RESULTS (PHASE 3)
LBA3
LIBRETTO-432: ADJUVANT SELPERCATINIB IN STAGE IB-IIIA RET FUSION-POSITIVE NSCLC - EFS
PRIMARY RESULTS (PHASE 3)
8506
OPTITROP-LUNGO5: SACITUZUMAB TIRUMOTECAN + PEMBROLIZUMAB vs PEMBROLIZUMAB
AS 1L TREATMENT FOR PD-L1-POSITIVE ADVANCED NSCLC (RANDOMIZED PHASE 3)
8515
TRITON: TREMELIMUMAB + DURVALUMAB + CHEMO vs PEMBROLIZUMAB + CHEMO IN 1L NSQ
MNSCLC WITH STK11, KEAP1, AND/OR KRAS MUTATIONS (PHASE 2B INTERIM ANALYSIS)
LBA8500
WU-KONG28: SUNVOZERTINIB MONOTHERAPY vs PLATINUM-BASED CHEMO AS 1L TREATMENT
WWW.ONCOALERT360.COM
FOR ADVANCED NSCLC WITH EGFR EXON20INS (MULTINATIONAL PHASE 3)
8002
LORIN: NEOADJUVANT LORLATINIB IN STAGE III NSCLC HARBORING ALK FUSION (PHASE 2
MULTICENTER)
8502
CROWN: LORLATINIB vs CRIZOTINIB AS 1L TREATMENT FOR ADVANCED ALK+ NSCLC - 7-YEAR
UPDATE (PHASE 3)
8503
ALKOVE-1: NELADALKIB EFFICACY AND SAFETY IN PATIENTS WITH ADVANCED ALK+ NSCLC
LBA1510
LOW-DOSE PEMBROLIZUMAB WITH CHEMOTHERAPY IN ADVANCED NSCLC
8519
SILEVERTINIB (BDTX-1535) IN TREATMENT-NAİVE NSCLC WITH NON-CLASSICAL EGFR MUTATIONS
(PHASE 2)
ACCELERET-LUNG: PRALSETINIB AS 1L TREATMENT OF RET FUSION-POSITIVE ADVANCED/METASTATIC
8504
NSCLC (PHASE 3)
LBA8005
CONCURRENT THORACIC RADIOTHERAPY, PLATINUM/ETOPOSIDE CHEMOTHERAPY, AND DURVALUMAB
IMMUNOTHERAPY IN EXTENSIVE-STAGE SCLC (PHASE III)
Leads
Senior Faculty
Participating AF
Dr Horinouchi
Dr. özkerim
Dr Morgan
Dr. Liu
Dr Peters
Dr. Lovly
Dr. Lopes
Dr. Aggarwal
Dr. Reck
Dr. Mirallas
Med Onc
Med Onc
Clin Onc
Med Onc
Med Onc
Med Onc
Med Onc
Med Onc
Med Onc
Med Onc
ASCO
AMERICAN SOCIETY OF CLINICAL ONCOLOGY
KNOWLEDGE CONQUERS CANCER
ASCO Annual Meeting
Abstract #: 8506
Oral Abstract Session
Sacituzumab tirumotecan (sac-TMT) plus pembrolizumab (P) versus
pembrolizumab (P) as first-line treatment for PD-L1-positive
advanced non-small cell lung cancer (NSCLC): Results from the
randomized phase 3 OptiTROP-Lung05 study.
Authors: Caicun Zhou, Anwen Xiong, Wenxiu Yao, Wei Zheng, Yan Yu, Peng Chen, Hua Zhong, Hui Wang, Bolin Chen,
Haiyong Wang, Yun Fan, Yunpeng Yang, Xingxiang Pu, Qiming Wang, Xia Song, Zhangzhou Huang, Xiao-bo Du, Yan
Qing, Xiaoping Jin, Junyou Ge
Organizations: Department of Oncology, Shanghai East Hospital, Tongji University, Shanghai, China, Department of
Medical Oncology, University of Electronic Science and Technology of China, Sichuan Cancer Hospital and Institute
& Cancer, The Second People's Hospital of Sichuan Province, Chengdu, China, Department of Oncology, Shengjing
Hospital, China Medical University, Shenyang, China, Department of Medical Oncology, Harbin Medical University
Cancer Hospital, Harbin, China, Department of Thoracic Oncology, Tianjin Medical University Cancer Institute and
Hospital, Tianjin, China, Department of Respiratory and Critical Care Medicine, Shanghai Chest Hospital, Shanghai,
China, Thoracic Radiotherapy Department I, Hunan Cancer Hospital, Changsha, China, Thoracic Medicine
Department II, Hunan Cancer Hospital, Changsha, China, Department of internal Medicine-Oncology, Shandong
Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences,
Jinan, China, Department of Thoracic Oncology, Zhejiang Cancer Hospital, Hangzhou, China, Department of Medical
Oncology, Sun Yat-sen University Cancer Center, Guangzhou, China, Lung & Gastrointestinal Oncology Department,
Hunan Cancer Hospital, Changsha, China, Department of Internal Medicine, The Affiliated Cancer Hospital of
Zhengzhou University & Henan Cancer Hospital, Institute of Cancer Research, Henan Academy of Innovations in
Medical Science, Zhengzhou, China, Respiratory Department, Shanxi Province Cancer Hospital, Taiyuan, China,
Department of Thoracic Medical Oncology, Fujian Cancer Hospital, Fuzhou, China, Oncology Department, Mianyang
Central Hospital, School of Medicine, University of Electronic Science and Technology of China, Mianyang, China,
Clinical Research Center, Sichuan Kelun-Biotech Biopharmaceutical Co., Ltd., Chengdu, China, Clinical Research
Center, Sichuan Kelun-Biotech Biopharmaceutical Co., Ltd., National Engineering Research Center of Targeted
Biologics, Chengdu, China
Background:
Pembrolizumab has been the standard first-line treatment for PD-L1 positive advanced NSCLC.
Sac-TMT, a TROP2-directed antibody-drug conjugate with a unique bifunctional linker, and PD-1/
L1 inhibitors demonstrate complementary mechanisms that enhance antitumor activity in the
first-line treatment of NSCLC (Hong et al., Nat Med, 2025). Here, we report the results from the
---
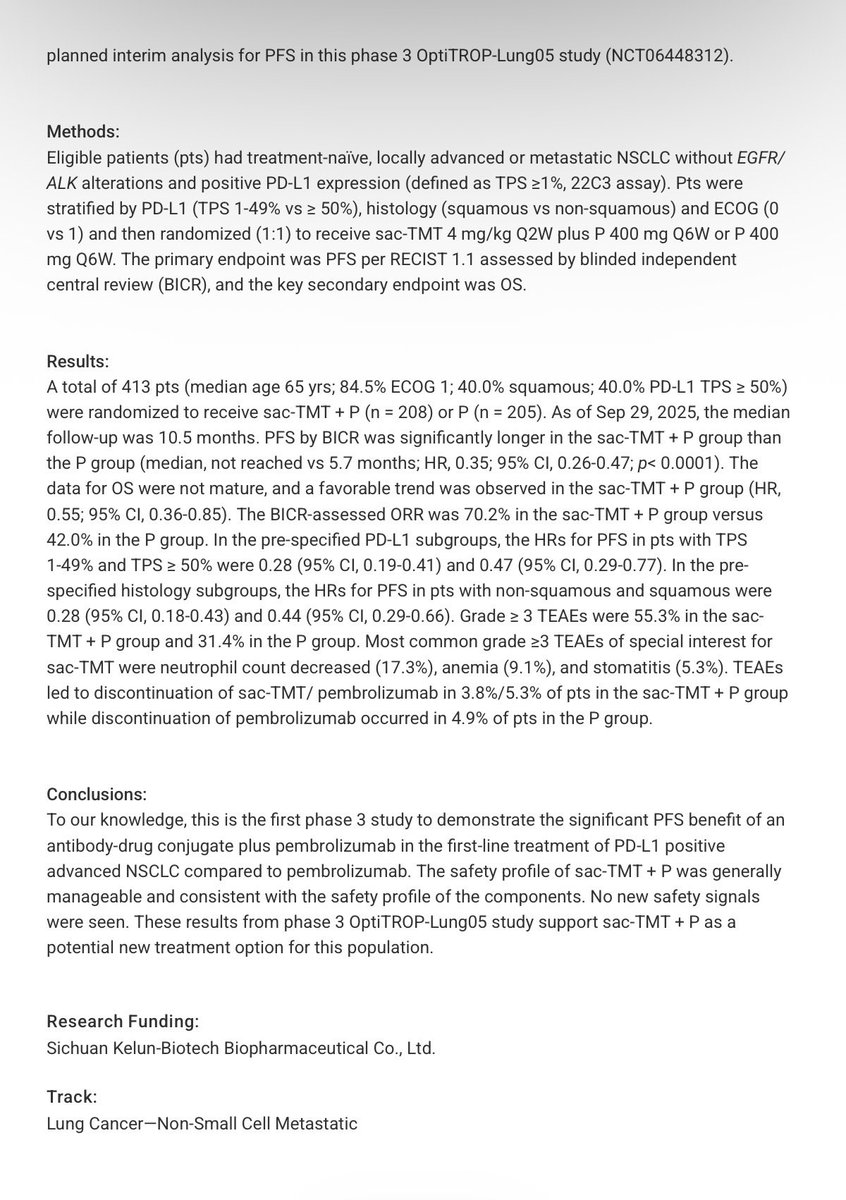
planned interim analysis for PFS in this phase 3 OptiTROP-Lung05 study (NCT06448312).
Methods:
Eligible patients (pts) had treatment-naive, locally advanced or metastatic NSCLC without EGFR/
ALK alterations and positive PD-L1 expression (defined as TPS >1%, 22C3 assay). Pts were
stratified by PD-L1 (TPS 1-49% VS ≥ 50%), histology (squamous VS non-squamous) and ECOG (0
VS 1) and then randomized (1:1) to receive sac-TMT 4 mg/kg Q2W plus P 400 mg Q6W or P 400
mg Q6W. The primary endpoint was PFS per RECIST 1.1 assessed by blinded independent
central review (BICR), and the key secondary endpoint was OS.
Results:
A total of 413 pts (median age 65 yrs; 84.5% ECOG 1; 40.0% squamous; 40.0% PD-L1 TPS ≥ 50%)
were randomized to receive sac-TMT + P (n = 208) or P (n = 205). As of Sep 29, 2025, the median
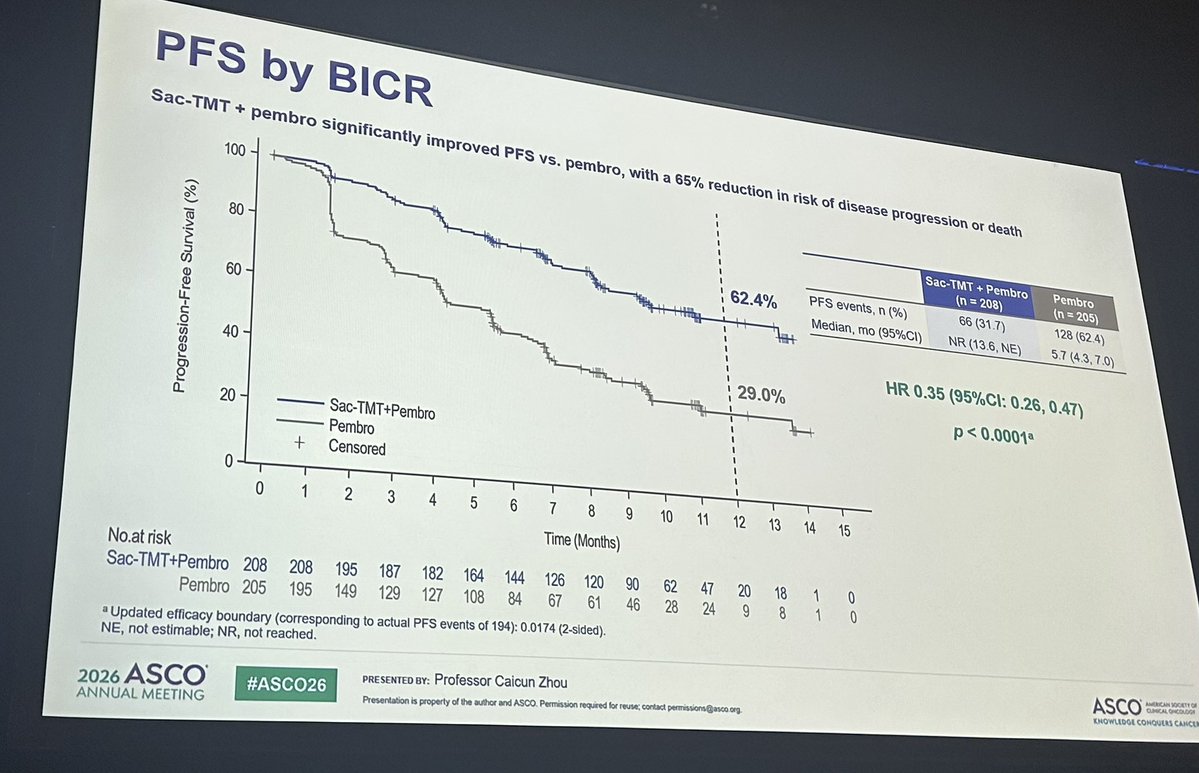
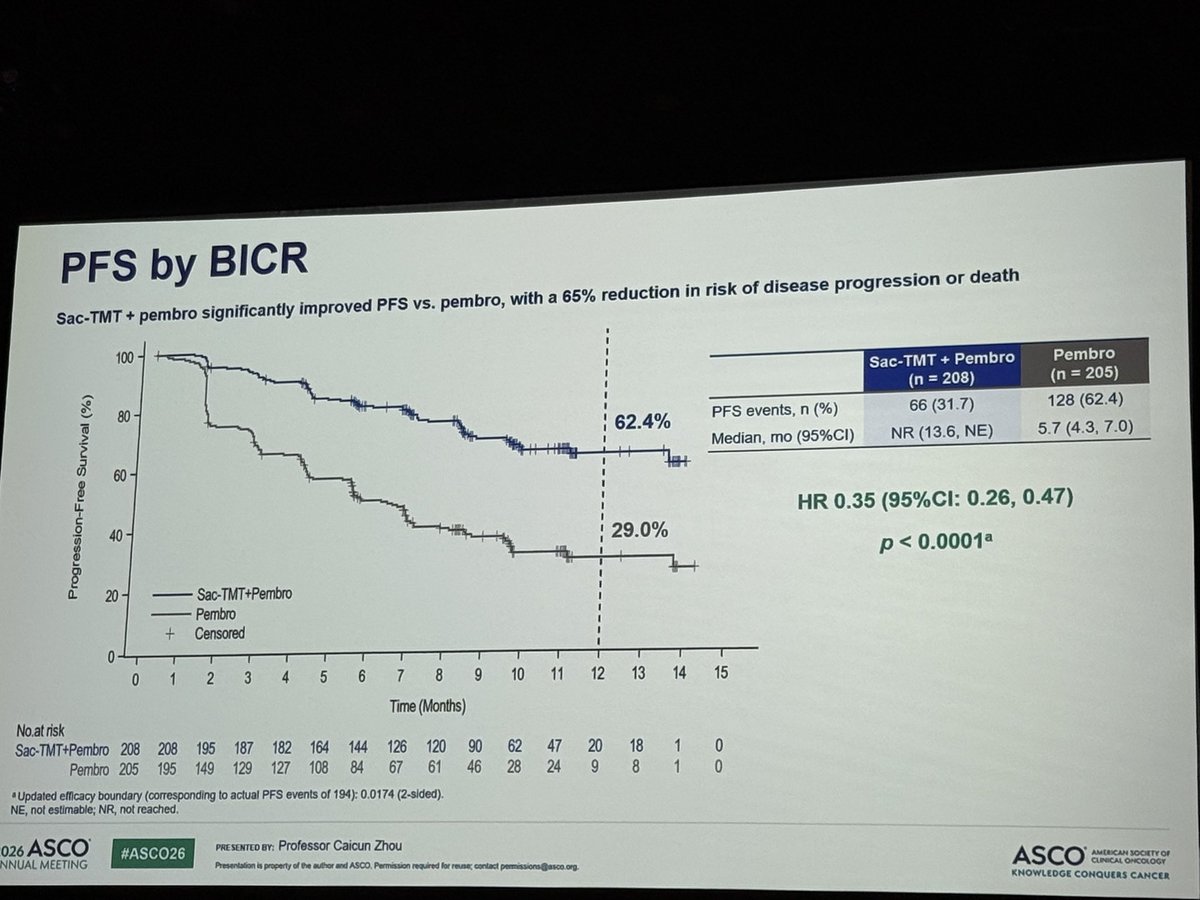
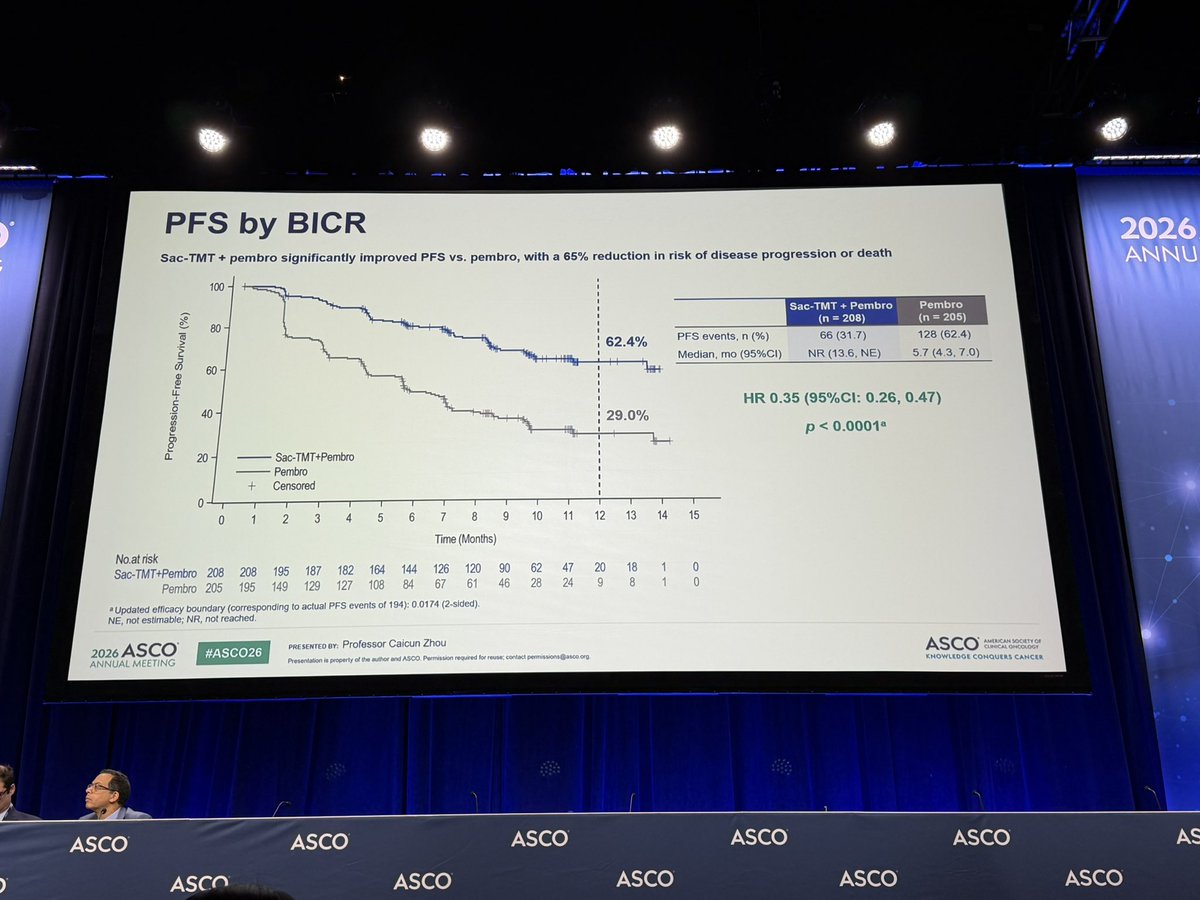
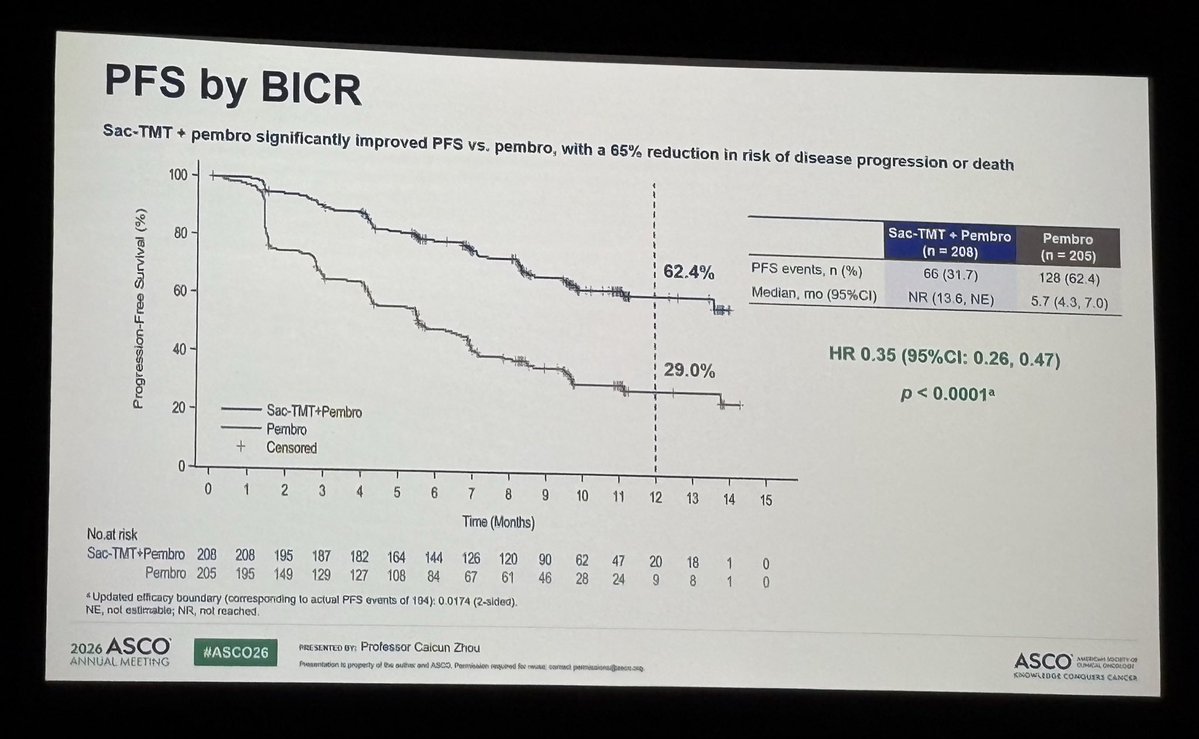
follow-up was 10.5 months. PFS by BICR was significantly longer in the sac-TMT + P group than
the P group (median, not reached VS 5.7 months; HR, 0.35; 95% CI, 0.26-0.47; p< 0.0001). The
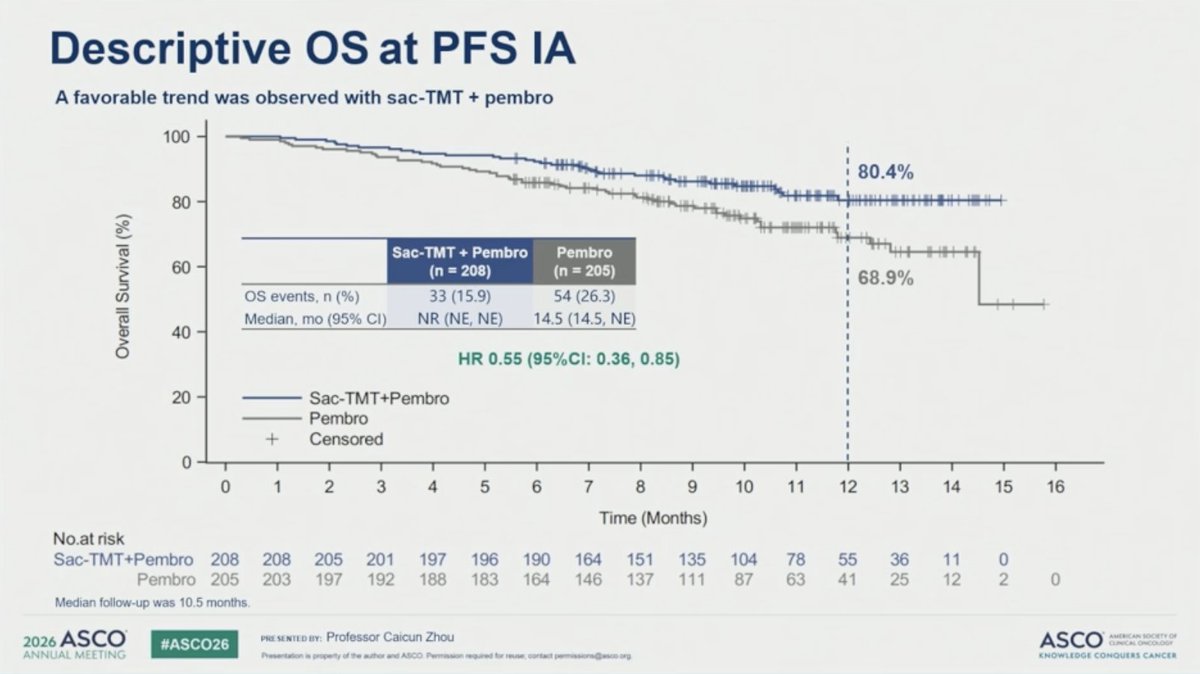
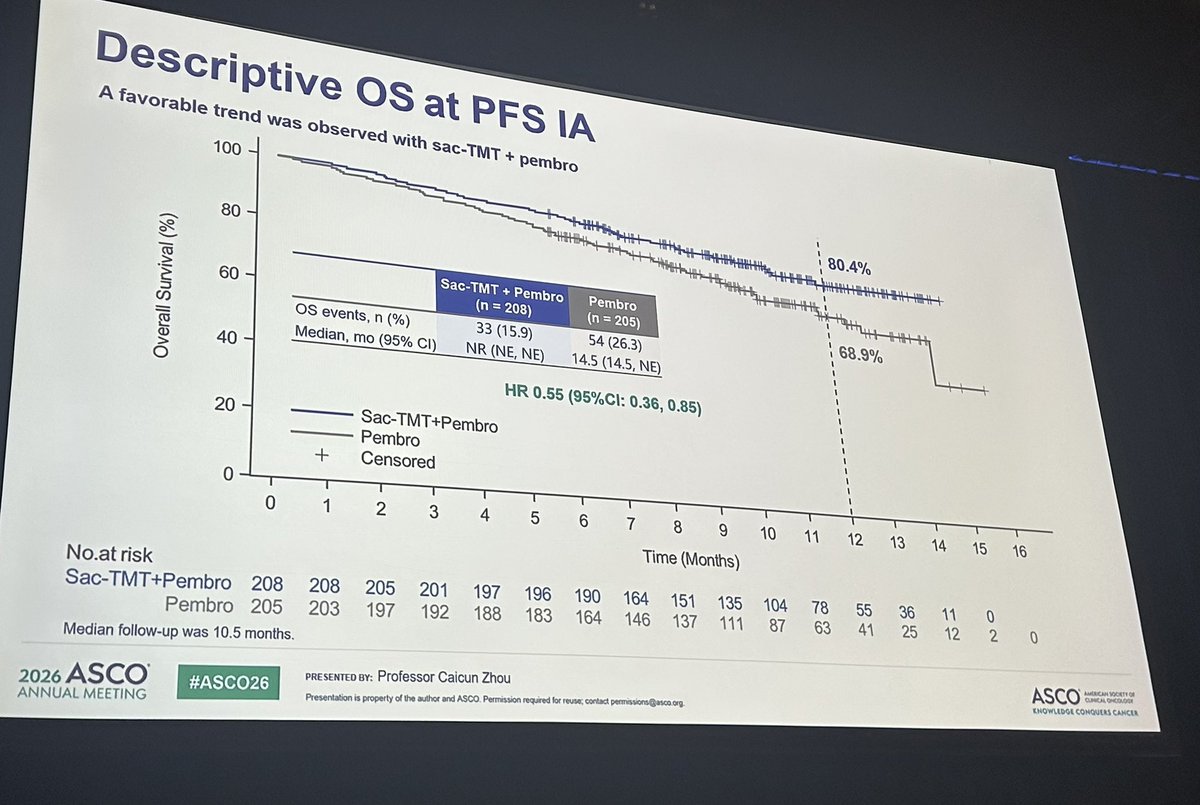
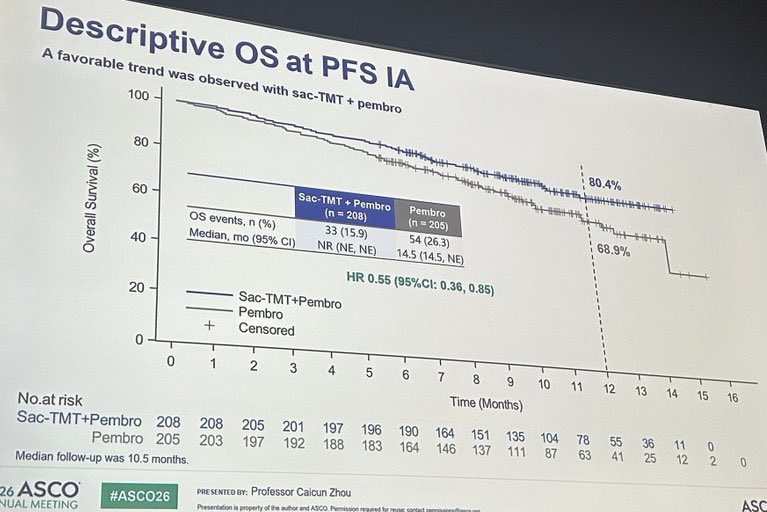
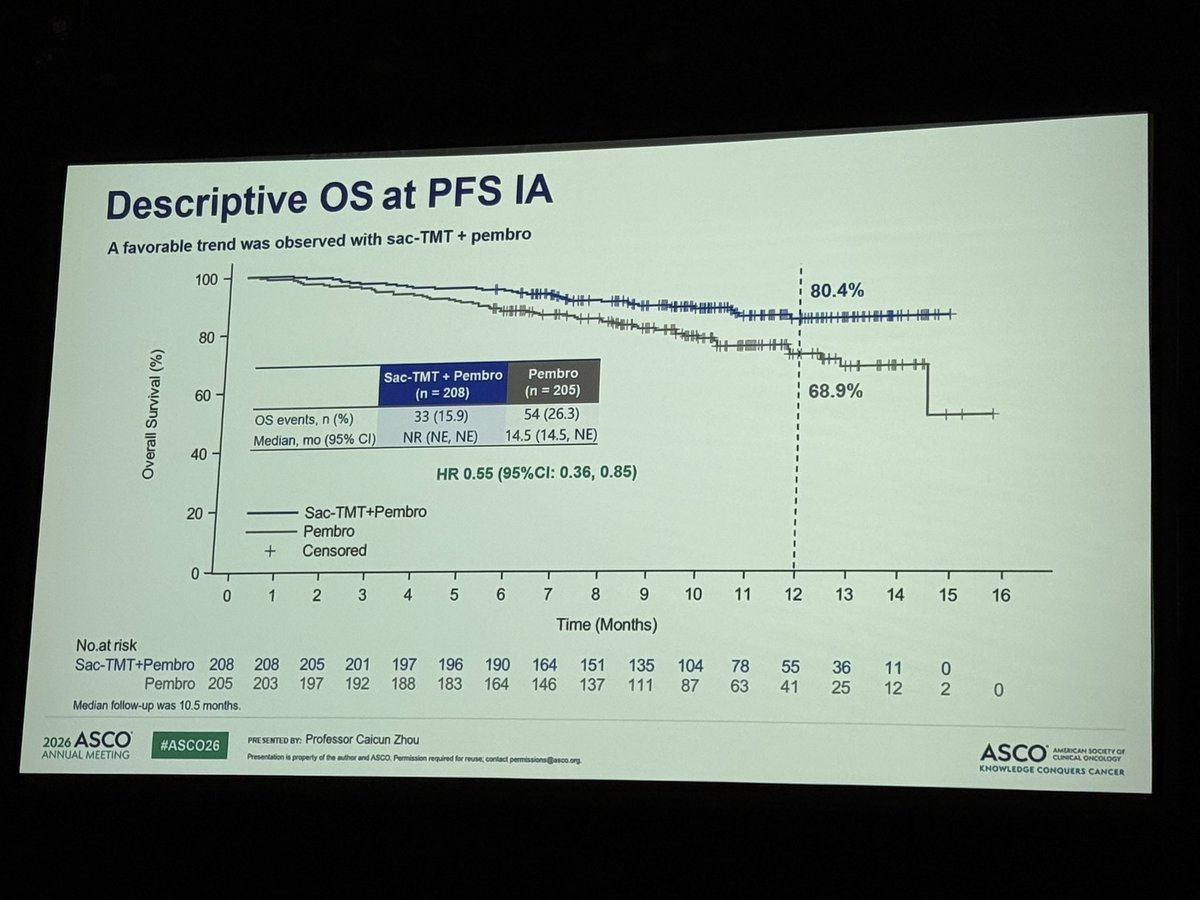
data for OS were not mature, and a favorable trend was observed in the sac-TMT + P group (HR,
0.55; 95% CI, 0.36-0.85). The BICR-assessed ORR was 70.2% in the sac-TMT + P group versus
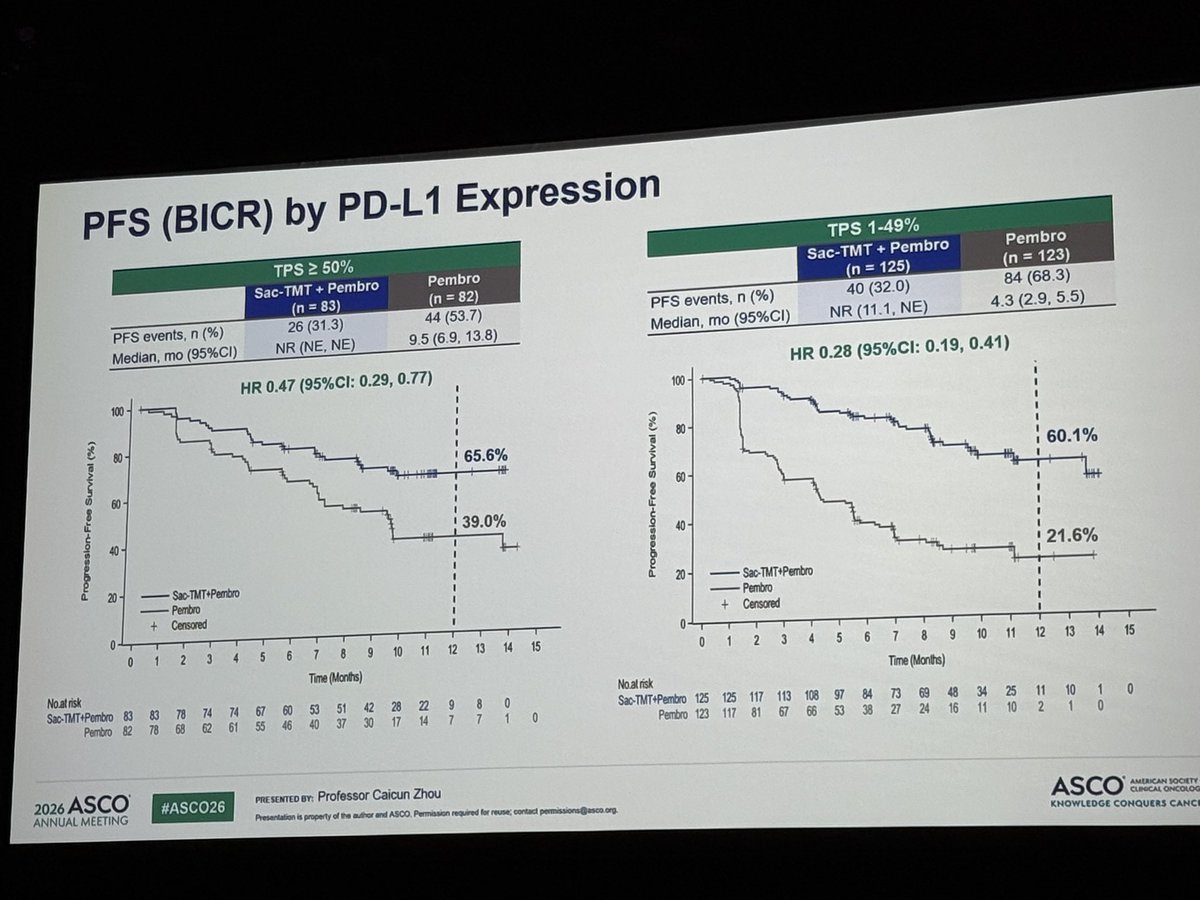
42.0% in the P group. In the pre-specified PD-L1 subgroups, the HRs for PFS in pts with TPS
1-49% and TPS ≥ 50% were 0.28 (95% CI, 0.19-0.41) and 0.47 (95% CI, 0.29-0.77). In the pre-
specified histology subgroups, the HRs for PFS in pts with non-squamous and squamous were
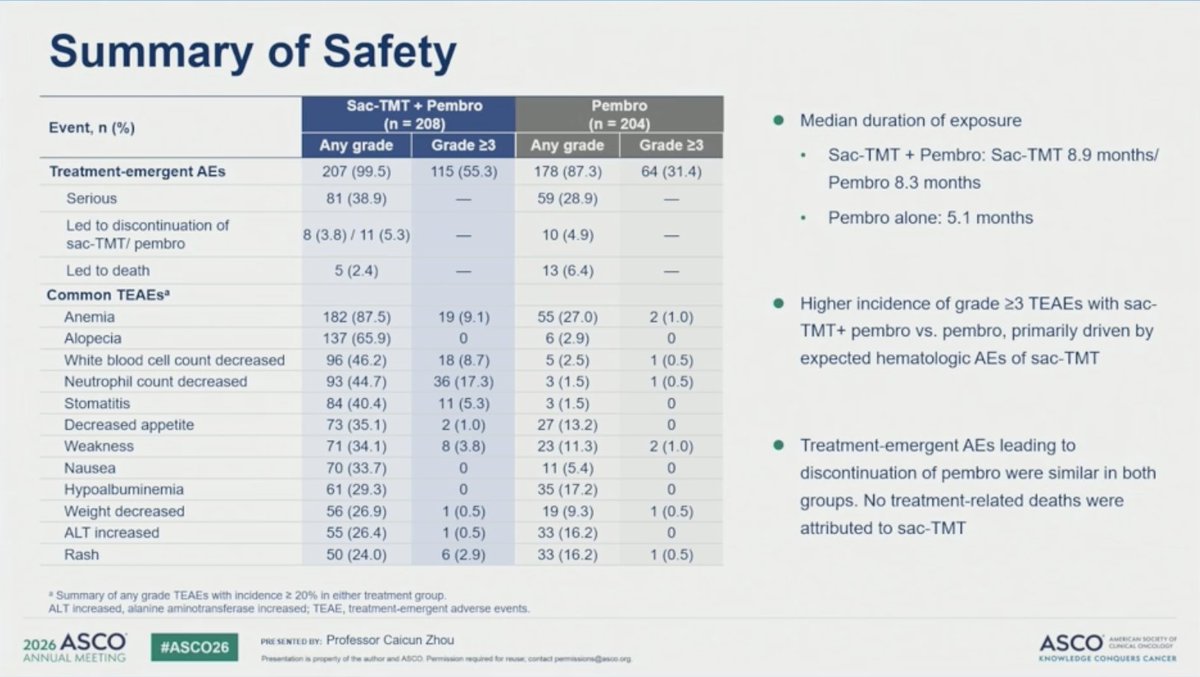
0.28 (95% CI, 0.18-0.43) and 0.44 (95% CI, 0.29-0.66). Grade ≥ 3 TEAEs were 55.3% in the sac-
TMT + P group and 31.4% in the P group. Most common grade ≥3 TEAEs of special interest for
sac-TMT were neutrophil count decreased (17.3%), anemia (9.1%), and stomatitis (5.3%). TEAEs
led to discontinuation of sac-TMT/ pembrolizumab in 3.8%/5.3% of pts in the sac-TMT + P group
while discontinuation of pembrolizumab occurred in 4.9% of pts in the P group.
Conclusions:
To our knowledge, this is the first phase 3 study to demonstrate the significant PFS benefit of an
antibody-drug conjugate plus pembrolizumab in the first-line treatment of PD-L1 positive
advanced NSCLC compared to pembrolizumab. The safety profile of sac-TMT + P was generally
manageable and consistent with the safety profile of the components. No new safety signals
were seen. These results from phase 3 OptiTROP-Lung05 study support sac-TMT + P as a
potential new treatment option for this population.
Research Funding:
Sichuan Kelun-Biotech Biopharmaceutical Co., Ltd.
Track:
Lung Cancer-Non-Small Cell Metastatic
ASCO 2026
PHASE 3 NSCLC
MV Onco
ADC + IO Enters
Frontline NSCLC
ONE CORE TAKEAWAY
PD-L1 positive advanced NSCLC
Sac-TMT + pembrolizumab VS pembrolizumab alone
ADC + IO may emerge
as a powerful
chemo-free frontline
strategy in
PD-L1 positive NSCLC.
Sac-TMT + pembrolizumab delivered
an unusually deep PFS benefit over
pembrolizumab alone.
HR 0.35
Median PFS:
not reached VS 5.7 months
ORR:
70.2% VS 42.0%
Zhou et al
ASCO 2026
OptiTROP-Lung05 (NCT05870956) is the Phase 3 trial that took sacituzumab tirumotecan (sac-TMT, SKB264 / MK-2870) — a TROP2-directed antibody-drug conjugate developed by Kelun-Biotech and globally partnered with Merck — into first-line PD-L1-positive advanced NSCLC in combination with pembrolizumab. Presented at ASCO 2026, the trial met its primary PFS endpoint with a 65% reduction in the risk of progression or death vs pembrolizumab monotherapy (p<0.0001), making this the first Phase 3 of an antibody-drug conjugate combined with an immune-checkpoint inhibitor to meet its primary endpoint in 1L NSCLC — a result KOLs are flagging as a potential paradigm shift for frontline IO+ADC combinations across multiple tumor types. Sac-TMT + pembro previously received Breakthrough Therapy Designation in China for this indication.
Population
Treatment-naïve advanced NSCLC with PD-L1 expression (1L), without actionable driver mutations.
Intervention
Sac-TMT (sacituzumab tirumotecan) + pembrolizumab vs pembrolizumab monotherapy.
Primary Endpoint
Progression-free survival by blinded independent central review (RECIST 1.1).
Key Secondary
Overall survival, objective response rate, duration of response, safety/tolerability, and PD-L1 subgroup analyses.
Efficacy & Safety
Reported Results
Progression-Free Survival (Primary Endpoint)
Sac-TMT + pembrolizumab produced a 65% reduction in the risk of progression or death vs pembrolizumab monotherapy in treatment-naïve PD-L1+ advanced NSCLC — a highly statistically significant outcome (p<0.0001). The PFS benefit was consistent in the prespecified PD-L1 subgroup analyses presented at ASCO 2026.
At the September 29, 2025 data cutoff, overall survival was immature but showed a strong trend favoring the combination — a preliminary ~45% improvement in OS in favor of sac-TMT + pembrolizumab. Mature OS data are expected at follow-up analyses.
The safety profile was generally manageable with the addition of sac-TMT: Grade 3+ TEAEs occurred in 55.3% on sac-TMT + pembrolizumab vs 31.4% on pembrolizumab alone. KOLs flagged the magnitude of PFS benefit as compelling relative to the modest additional toxicity from an ADC backbone.
STATUSInvestigational in the US · BTD granted in China for 1L PD-L1+ NSCLC
Sac-TMT + pembrolizumab in 1L PD-L1+ advanced NSCLC is currently investigational in the United States. In China, the combination received Breakthrough Therapy Designation for this indication, supported by OptiTROP-Lung05 efficacy. The sponsors have also received FDA Breakthrough Therapy Designation for sac-TMT in EGFR-mutant NSCLC (separate program); regulatory filings in the 1L PD-L1+ setting are anticipated. The combination represents the first Phase 3 evidence supporting an ADC + IO frontline regimen in NSCLC.