LIBRETTO-432 Key Takeaways
Design - Phase 3 adjuvant selpercatinib (Retevmo) vs placebo, resected stage IB-IIIA RET fusion-positive NSCLC, n=151 (NCT04819100); primary endpoint event-free survival.
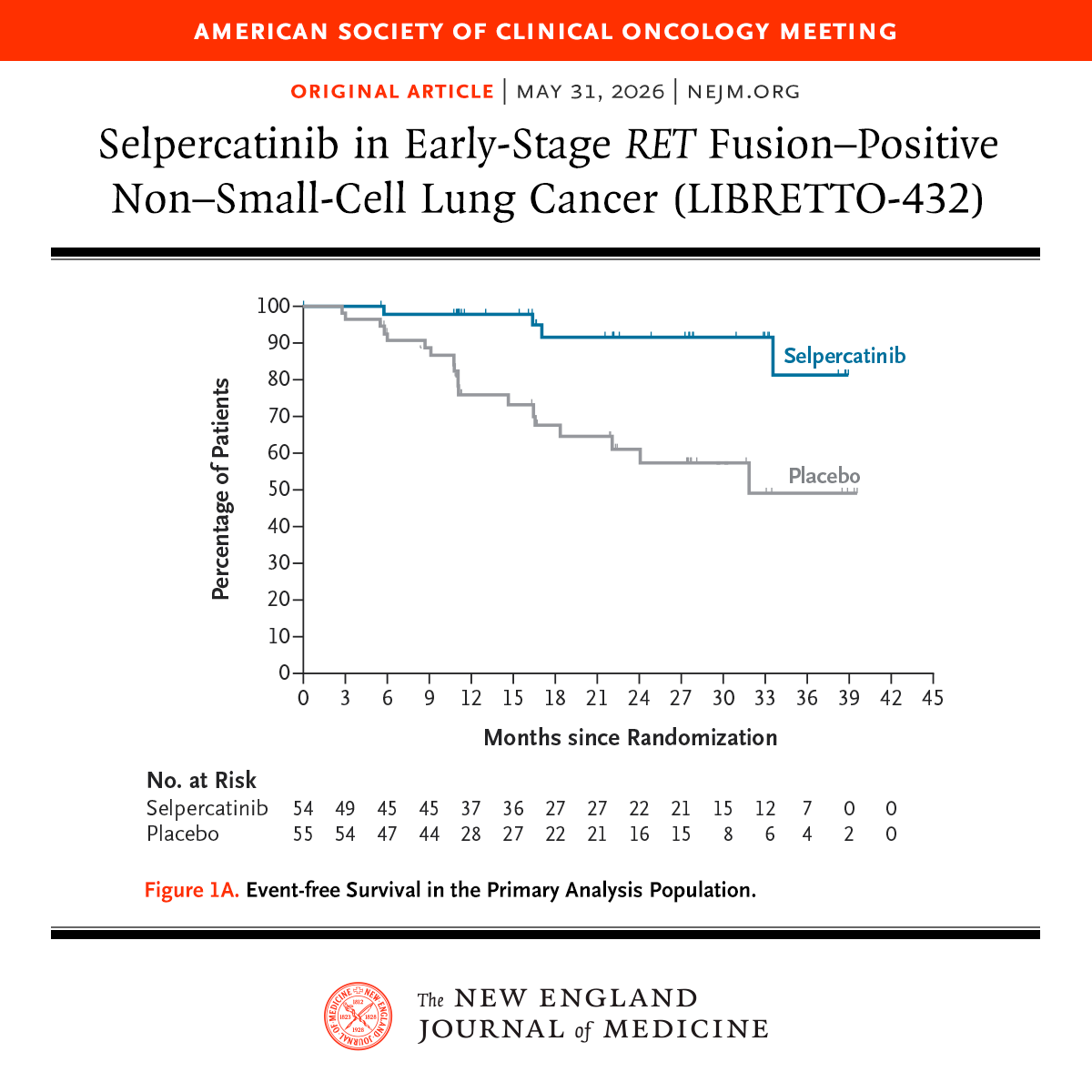
EFS (primary, ASCO 2026 LBA3) - MET - stage II-IIIA HR 0.172 (95% CI 0.058-0.509), P=0.0003 (an 83% reduction); 2-yr EFS 91.5% vs 61.1%. Overall IB-IIIA: 93.8% vs 69.6%, HR 0.165.
OS - Secondary, immature - low event count; trend favors selpercatinib but not yet interpretable.
Safety - Grade >=3 TEAEs 66.7% vs 23.7%; grade >=3 ALT 17.3% / AST 18.7%; AE discontinuation 17.3% vs 1.3%; no treatment-related deaths.
Regulatory - Investigational (adjuvant) - not FDA approved; Retevmo is FDA approved in advanced/metastatic RET+ NSCLC (LIBRETTO-001).
Sponsor / drug - Loxo@Lilly (Eli Lilly); selpercatinib (Retevmo).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.
KOLs Discussing LIBRETTO-432
LIBRETTO-432 Key Slides & Visuals
Slides shared by KOLs at ASCO 2026 plenary (LBA3, presented by Jonathan W. Goldman, MD, UCLA) plus earlier social conversation. Click any image to expand.






















Top LIBRETTO-432 Tweets

#ASCO26 Plenary Session is happening today! 🌟 Five major studies across four disease sites will be presented in the Plenary Session. Several plenary studies have already been published online: 📘 LIBRETTO-432 — NEJM Adjuvant selpercatinib in early-stage RET fusion–positive

Day 3 #ASCO26 5 plenary highlights: 1. #PROTEUS: PeriOp/PostOp Apa in Prostate Ca 2. #SARC041: Adj Abema in dediff liposarcoma 3. #LIBRETTO432 : Adj Selpercatinib in NSCLC 4. #HARMONi6: 1L Ivonescimab in Sq mNSCLC 5. #RASolute302: 2L Daraxonrasib in Panc Ca @ASCO 1/6

Ladies and gentlemen, we officially have a NEW standard of care in resectable RET fusion+ NSCLC. LIBRETTO-432: Adjuvant selpercatinib x 3 yrs vs placebo: 🔹Stage II–IIIA 2-yr EFS: 92% vs 61% 🔹HR 0.17, P<0.001 Overall stage IB–IIIA: 🔹2-yr EFS: 94% vs 70% 🔹HR 0.16 #ASCO26

🔥🚨@OncoAlert Hot off the press. Just published @NEJM In conjunction with presentation @ASCO #ASCO26. ⭐️Results of #PracticeChanging #LIBRETTO432 Trial of: #Adjuvant #Selpercatinib vs #Placebo in Early-Stage (IB-IIIA) #RET+ Non-Small-Cell #LungCancer. ✅⬆️#EFS ❇️#HR:

🔥🔥🔥Perhaps the most remarkable aspect of LIBRETTO-432 is not the hazard ratio. It’s how far the field has come. A decade ago, RET fusions were largely undruggable. Today, a highly selective RET inhibitor reduces the risk of recurrence or death by nearly 83% in patients

🚨 PRACTICE CHANGING DATA at #ASCO26 🚨 LIBRETTO-432 Adjuvant selpercatinib vs placebo: ✅ HR 0.172 (p=0.0003) ✅ 24-mo EFS: 91.5% vs 61.1% ✅ Consistent across ALL subgroups This is why we TEST EVERY patient. Every. Single. One. 🧬

First positive adjuvant pIII study wth selpercatinib in stage IB–IIIA RET-positive NSCLC: LIBRETTO-432. Impressive results!, now in #NEJM. Nicely discussed @christine_lovly TKI duration, MRD, screening, and broader biomarker testing in early-stage #ASCO26 #NSCLC #RETfusion
🚨 #ASCO26 Plenary | LIBRETTO-432 #️⃣LBA3 📚Simultaneously published in NEJM https://t.co/yIPxmCTvA1 🧬 Phase 3, global, double-blind trial Stage IB–IIIA RET fusion+ NSCLC after definitive therapy Selpercatinib vs placebo 👥 N=151 ✅ Primary endpoint met Adjuvant selpercatinib
3. LIBRETTO-432: PhIII, adjuvant Selpercatinib (for 3yrs) in Stg IB-IIIA RET fusion positive NSCLC: - 2yrs EFS: 94% vs. 70% (HR: 0.17) - ~90% received adj chemo - AEs: ⬆️LFTs - New SoC in adj NSCLC for RET fusion 4/6
🔥🚨@OncoAlert Hot off the press. Just presented @ASCO #ASCO26 (#Plenary Presentation) by Dr. Jonathan Goldman. ⭐️Results of #PracticeChanging #LIBRETTO432 Trial of: #Adjuvant #Selpercatinib vs #Placebo in Early-Stage (IB-IIIA) #RET+ Non-Small-Cell #LungCancer. ✅⬆️#EFS

Dr. Jonathan Goldman presents analysis from LIBRETTO-432 at #ASCO26 plenary: adjuvant selpercatinib 160mg bid vs placebo x 3y in pts with resected RET fusion-positive NSCLC (n=151). Chemo permitted but not mandated. Primary endpoint EFS in stage II-IIIA - where >90% had chemo.

🆙 #ASCO26 #LCSM Plenary Session 🔥LIBRETTO-432: Event-Free Survival with Adjuvant Selpercatinib in Stage IB-IIIA RET Fusion-Positive NSCLC ✅Stage II-IIIA EFS HR 0.172 (95%CI 0.058-0.509; p=0.0003) ✅2-yr EFS 91.5% vs 61.1%; mEFS NR vs 31.8mo ✅No deaths on study treatment 🎙️Dr.
Overview
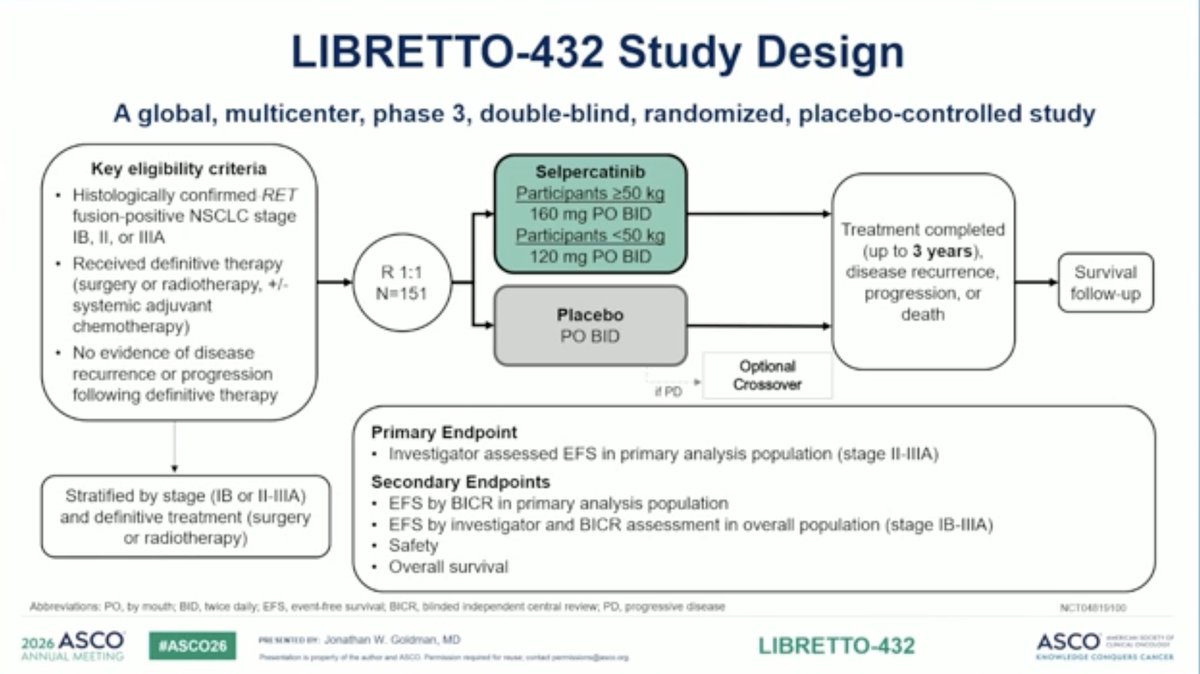
LIBRETTO-432 (NCT04819100) is a Phase 3, global, multicenter, randomized, double-blind, placebo-controlled trial of adjuvant selpercatinib (Retevmo) in patients with resected stage IB–IIIA RET fusion-positive non-small cell lung cancer following completion of definitive surgery or radiotherapy, with or without adjuvant chemotherapy/durvalumab. The trial enrolled 151 patients randomized 1:1 to selpercatinib 160 mg twice daily or placebo for up to 3 years. The primary endpoint is investigator-assessed event-free survival (EFS) in the stage II–IIIA primary analysis population. Full primary results were presented at the #ASCO26 Plenary Session (LBA3) by Jonathan W. Goldman, MD (UCLA).
Study Design
Phase 3, global (22 countries), randomized 1:1, double-blind, placebo-controlled. Stratified by disease stage (IB/II/IIIA) and prior definitive therapy. Maximum treatment duration 3 years. Crossover allowed for placebo patients with recurrence.
Population
n=151 with histologically confirmed Stage IB/II/IIIA NSCLC, RET fusion-positive by PCR/NGS, prior definitive locoregional therapy with curative intent, ECOG 0-1. Max 26 weeks from definitive therapy to randomization.
Intervention
Experimental: Selpercatinib 160 mg PO BID (120 mg if <50 kg) in continuous 28-day cycles for up to 3 years. Control: Matched placebo.
Endpoints
Primary: Investigator-assessed EFS in the primary analysis population (stage II–IIIA). Secondary: EFS by BICR; EFS in the overall population (stage IB–IIIA); safety; overall survival.
Primary Results — #ASCO26 Plenary (LBA3)
Event-Free Survival (Primary Endpoint — MET)
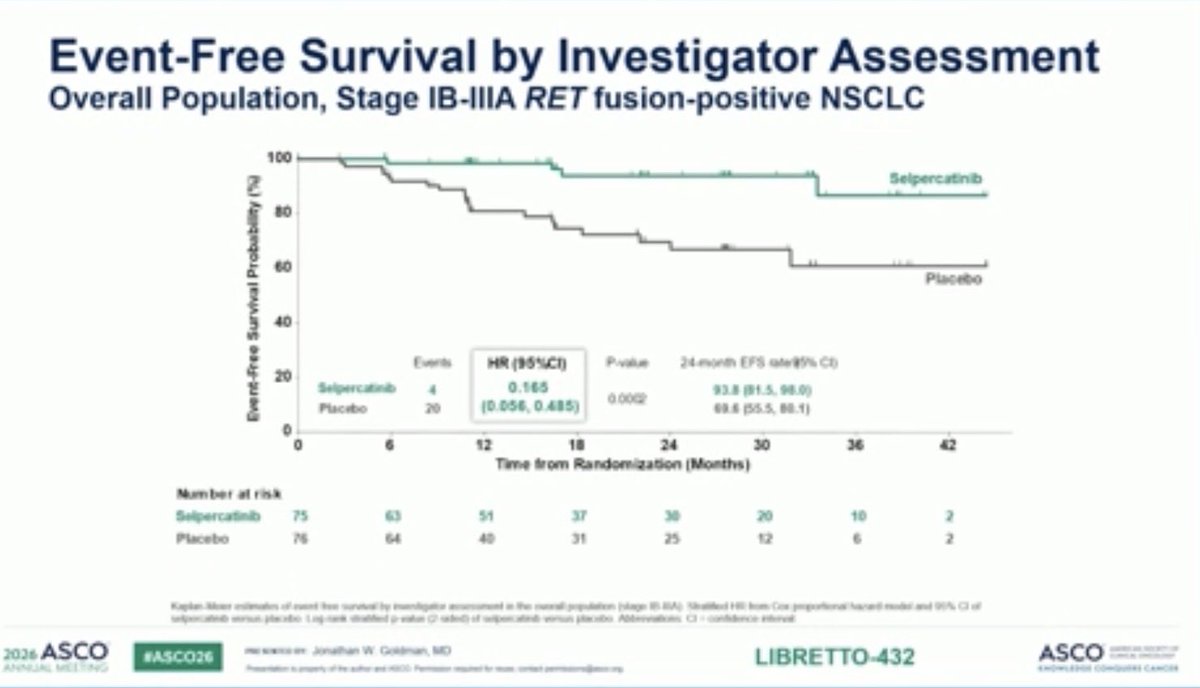
Adjuvant selpercatinib produced a statistically significant and clinically meaningful improvement in investigator-assessed EFS in the stage II–IIIA primary analysis population, with a hazard ratio of 0.172 (95% CI 0.058–0.509; P=0.0003) — an 83% reduction in the risk of disease recurrence, progression, or death versus placebo (events: 4 selpercatinib vs 19 placebo). Median EFS was not reached with selpercatinib versus 31.8 months with placebo, and the 2-year EFS rate was 91.5% vs 61.1%. The benefit extended to the overall stage IB–IIIA population (HR 0.165, 95% CI 0.056–0.485; P=0.0002; 2-year EFS 93.8% vs 69.6%) and was consistent by blinded independent central review and across predefined subgroups. The magnitude aligns with the precedents set by adjuvant osimertinib in ADAURA (HR 0.17) and adjuvant alectinib in ALINA (HR 0.24).
Stage II–IIIA: 2-yr EFS 91.5% vs 61.1% · HR 0.172 · Overall IB–IIIA: 93.8% vs 69.6% · HR 0.165Sources: ApexOnco ASCO 2026 plenary coverage (Goldman LBA3) · The ASCO Post (Abstract LBA3) · Wu et al., NEJM, May 31, 2026 (doi:10.1056/NEJMoa2602628)Overall Survival (Secondary — Immature)
Overall survival data remain immature at this analysis due to a low number of OS events; the trend favored selpercatinib but is not yet interpretable. OS in both the primary analysis population and overall stage IB–IIIA population is a gated secondary endpoint and will continue to be followed.
OS immature — trending favorable, follow-up ongoingSources: ApexOnco ASCO 2026 plenary coverage (Goldman LBA3) · The ASCO Post (Abstract LBA3) · Targeted OncologySafety & Tolerability (Overall Population, n=75 vs 76)
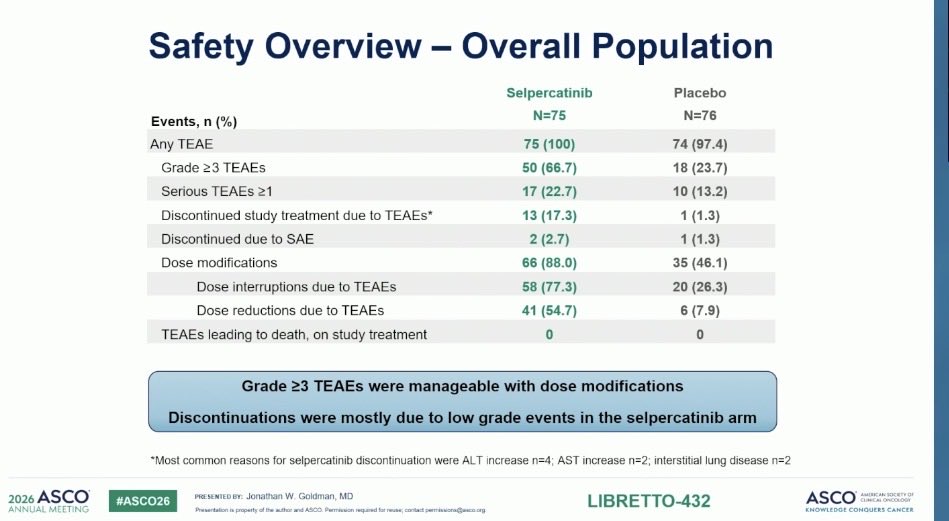
The safety profile was generally consistent with the established selpercatinib experience in advanced RET+ NSCLC, with no treatment-related deaths in either arm. Grade ≥3 TEAEs occurred in 66.7% of selpercatinib patients vs 23.7% on placebo; serious TEAEs in 22.7% vs 13.2%. Treatment discontinuation due to TEAEs was 17.3% (selpercatinib) vs 1.3% (placebo) — most commonly from ALT increase (n=4), AST increase (n=2), and interstitial lung disease (n=2). Dose reductions occurred in 54.7% vs 7.9% and dose interruptions in 77.3% vs 26.3%. The most common Grade ≥3 adverse events were the expected selpercatinib transaminase elevations — ALT increase Grade ≥3 in 17.3% (vs 1.3% placebo) and AST increase Grade ≥3 in 18.7% (vs 2.6%); hypertension Grade ≥3 occurred in 10.7% vs 2.6%. Per the investigators, Grade ≥3 events were manageable with dose modifications, and the discontinuations were mostly driven by low-grade events (ALT increase n=4, AST increase n=2, interstitial lung disease n=2).
G≥3 TEAE 66.7% vs 23.7% · G≥3 ALT 17.3% / AST 18.7% · D/C due to TEAE 17.3% vs 1.3% · 0 treatment-related deathsSources: Goldman LBA3 ASCO 2026 plenary Safety slide (Overall Population) · Wu et al., NEJM, May 31, 2026 (LIBRETTO-432)Clinical Implications
LIBRETTO-432 extends the adjuvant targeted-therapy paradigm (previously established for EGFR by ADAURA and ALK by ALINA) to the ~1–2% of NSCLC patients with RET fusions. The magnitude of EFS benefit reinforces the case for routine comprehensive genomic profiling in resectable Stage IB–IIIA disease — not just metastatic NSCLC. Pending regulatory filings and OS maturity, multiple KOLs (including Goldman in his plenary remarks) framed adjuvant selpercatinib as a candidate new standard of care for this molecularly defined subgroup.
Candidate new SoC · Reinforces mandate for adjuvant RET testingSources: OncUpdates ASCO 2026 preview · CancerNetwork · ApexOnco plenary coverageKey KOL Sentiments — LIBRETTO-432











































LIBRETTO-432 FAQ
What is the LIBRETTO-432 trial?
LIBRETTO-432 is a Phase 3 global, double-blind trial (NCT04819100; n=151) of adjuvant selpercatinib (Retevmo, a selective RET inhibitor) versus placebo in patients with resected stage IB-IIIA RET fusion-positive NSCLC following definitive surgery or radiotherapy. Event-free survival was the primary endpoint.
What did LIBRETTO-432 show at ASCO 2026?
The primary endpoint was met with a striking magnitude of benefit. In the stage II-IIIA primary analysis population, adjuvant selpercatinib produced an event-free survival hazard ratio of 0.172 (95% CI 0.058-0.509; P=0.0003) - an 83% reduction in the risk of disease recurrence or death - with a 2-year event-free survival of 91.5% versus 61.1%. In the overall stage IB-IIIA population, 2-year event-free survival was 93.8% versus 69.6% (HR 0.165).
Is adjuvant selpercatinib FDA approved for lung cancer?
Not in the adjuvant setting. Adjuvant selpercatinib in resected RET fusion-positive NSCLC (the LIBRETTO-432 setting) is investigational and not FDA approved. Selpercatinib (Retevmo) is FDA approved for locally advanced or metastatic RET fusion-positive NSCLC based on LIBRETTO-001; the adjuvant use remains under regulatory evaluation.
What is the safety profile in LIBRETTO-432?
The safety profile was consistent with the established selpercatinib experience in advanced RET+ NSCLC, with no treatment-related deaths in either arm. Grade 3 or higher treatment-emergent adverse events occurred in 66.7% of selpercatinib patients versus 23.7% on placebo, including grade 3 or higher ALT (17.3%) and AST (18.7%) elevations; adverse events led to discontinuation in 17.3% versus 1.3%.
Why is LIBRETTO-432 clinically important?
LIBRETTO-432 extends the adjuvant targeted-therapy paradigm - previously established for EGFR by ADAURA and for ALK by ALINA - to the roughly 1-2% of NSCLC patients with RET fusions. The magnitude of the event-free survival benefit reinforces the case for routine comprehensive genomic profiling (including RET testing) in resectable stage IB-IIIA NSCLC so eligible patients can be identified.