ASCENT-04 (KEYNOTE-D19) is a Phase 3 trial showing sacituzumab govitecan (Trodelvy; Gilead) plus pembrolizumab (Keytruda; Merck) improved progression-free survival versus pembrolizumab plus chemotherapy (11.2 vs 7.8 months; ~35% risk reduction) in first-line PD-L1-positive (CPS≥10) metastatic triple-negative breast cancer. On this basis the FDA approved the combination in June 24, 2026.
FDA APPROVED June 24, 2026 — first-line PD-L1+ (CPS≥10) metastatic TNBC
The FDA approved sacituzumab govitecan (Trodelvy, Gilead) in combination with pembrolizumab (Keytruda, Merck) for first-line PD-L1-positive (CPS≥10) unresectable locally advanced or metastatic triple-negative breast cancer — based on the Phase 3 ASCENT-04/KEYNOTE-D19 trial (published in NEJM).
Presentation figures and KOL infographics, grouped by congress and readout. The #ASCO26 biomarker-subgroup analysis (Abstract 1013, Tolaney) is called out first, followed by the PFS2 / subsequent-therapy readout (Kalinsky), the ESMO 2025 PRO/QoL data (de Azambuja), and the ASCO 2025 primary PFS readout (LBA109, Tolaney). Click any image to expand.
The ASCO 2026 biomarker analysis (Tolaney, Abstract 1013): SG + pembrolizumab extended median PFS over chemo + pembrolizumab across every prespecified biomarker subgroup — all four Trop-2 H-score quartiles (HRs 0.46–0.81), regardless of tumor BRCA (tBRCA WT HR 0.67 / mutant 0.88) and HER2-IHC0 vs HER2-low status — supporting the SG + pembro regimen for the broad PD-L1+ 1L mTNBC population without further biomarker selection.
[Slide 1]
2026
ASCO
ANNUAL MEETING
ASCENT-04: Analysis of Efficacy by Biomarker Subgroups With
Sacituzumab Govitecan + Pembrolizumab vs Chemotherapy +
Pembrolizumab in Participants With Previously Untreated
PD-L1+ Metastatic Triple-Negative Breast Cancer
Sara M Tolaney¹, Peter Schmid², Evandro de Azambuja³, Kevin Kalinsky⁴, Sung-Bae Kim5, Clinton Yam6,
Bernardo Rapoport⁷.⁸, Seock-Ah Im9, Barbara Pistilli10, Wassim Mchayleh11, David W Cescon¹², Junichiro Watanabe¹³,
Manuel Alejandro Lara Banuelas14, Ruffo Freitas-Junior15, Alain Lortholary¹⁶, Catherine Lai17, Ann Chen¹⁷,
Meghna Das Thakur¹⁷, Yajia Zhang¹⁷, Sherene Loi18
Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA, USA; Centre for Experimental Cancer Medicine, Bart's Cancer Institute, Queen Mary University of London,
London, UK; Pinstitut Jules Bordet, Hopital Universitaire de Bruxelles (H.U.B), Université Libre de Bruxelles (U.L.B.), Brussels, Belgium; "Winship Cancer Institute, Emory University,
Atlanta, GA, USA; Asan Medical Center, University of Ulsan College of Medicine, Seoul, Republic of Korea; The University of Texas MD Anderson Cancer Center, Houston, TX, USA;
The Medical Oncology Centre of Rosebank, Clinical and Translational Research Unit (CTRU). Saxonworld, South Africa; "Department of Immunology, Faculty of Health Sciences,
University of Pretoria, Pretoria, South Africa; Seoul National University Hospital, Cancer Research Institute, Seoul National University College of Medicine, Seoul National University,
Seoul, Republic of Korea: "Gustave Roussy, IHU-National PReciSion Medicine Center in Oncology, Villejuif, France; "AdventHealth Cancer Institute, Orlando, FL, USA; Princess
Margaret Cancer Centre/UHN, Toronto, ON, Canada; "Juntendo University Graduate School of Medicine, Tokyo, Japan; SCIENTIA Investigación Clinica, Chihuahua, Mexico:
"Advanced Center for Diagnosis of Breast Diseases Federal University of Goias, Goias, Brazil; "Groupe d'Investigateurs National des Etudes des Cancers Ovariens et du sein
(GINECO) and Hôpital Prive du Confluent Nantes, France: "Gilead Sciences, Inc., Foster City, CA, USA; Peter MacCallum Cancer Centre, Melbourne, Australia
2026 ASCO
#ASCO26
PSS SENTED RY: Sara M Tolaney, MD. MPH, FASCO
ASCO
AMERICAN SOCITY OF
CLINICAL
ANNUAL MEETING
Presentation property the - and MCO Permission - for - contact
ENOWLEDGE CONQUERS CANCER
2026
ASCO
ANNUAL MEETING
---
[Slide 2]
PFS by Trop-2 H-score Quartilesᵃ
SG + Pembro
Chemo + Pembro
Subgroup
HR (95% CI)
n
mPFS, mo
n
mPFS, mo
ITT Population1,b
221
11.2 (9.3-16.7)
222
7.8 (7.3-9.3)
0.65 (0.51-0.84)
Trop-2 BAS
204
11.7 (9.3-16.8)
196
7.8 (7.3-9.3)
0.63 (0.48-0.82)
Trop-2 H-score
Quartiles
Q1
48
9.3 (7.4-19.4)
47
9.0 (6.0-10.9)
0.81 (0.48-1.36)
Q2
50
9.6 (7.3-16.7)
50
7.4 (6.9-9.7)
0.73 (0.44-1.22)
Q3
55
13.5 (9.3-NE)
50
8.4 (5.6-10.8)
0.46 (0.27-0.80)
Q4
51
16.6 (8.1-NE)
49
9.2 (5.5-11.3)
0.57 (0.33-0.99)
0.25
0.5
1
2
Favors SG
+
Pembro
Favors Chemo
+
Pembro
PFS was longer with SG + pembro vs chemo + pembro across all Trop-2 subgroups
*Trop 2H score quartion Q1 0-224, C2. 225-279 03 04, HK value is stratulied HR values are underabled
BAS bromarker analysis set, chemo, chemotherapy HR, hazard rabo, ITT. intent to theat mo, months mPFS, metastatic progression tree survival NE, not entimable, pembro, pembrolizumab PFS progression free survival, Q. quartite; SG govdecan
1. Tokiney SM et al al. Engl. Med. 2026,394 354-66
2026 ASCO
#ASCO26
PIE SENTED un: Sara M Tolaney, MD, MPH. FASCO
ASCO
AMERICAN
ANNUAL MEETING
Presentation property of the - and ABCO Permission request for - contact permissions@son.org
KNOWLEDGE CONQUERS CANCER
2026 ASCO
ANNUAL MEETING
---
[Slide 3]
PFS by Trop-2 H-Score Quartilesᵃ
Q1
SG +
Chemo +
Q2
SQ+
Chamo +
Pembro
Pembro
Pembro
Pembro
100
(n = 48)
(n - 47)
100
(n = 60)
50)
Events
29
78
Events
27
33
80
80
PFS Probability (%)
Median
by
BICR,
(95%
CI),
the
9.3.(7.4-19.4)
PFS Probability (%)
Median
PFS
PFS
((6.0-10.9)
by
BICR,
CI),
9.8(7,3-16.7)
60
Unstratified HR nos C)
0.81 (0.45-1.36)
60
0.73(0.44-1.22)
40
40
20
20
0
0
0
2
4
6
8
10
12
14
16
18
20
22
24
26
20
10
0
2
I
6
a
10
12
14
15
18
20
22
24
26
28
30
Time (months)
Time (months)
No.
No alma (events)
41.00
*
17
22)
100
20%
9.128
42 (1)
17
7.05)
(27)
3 (27)
(27)
1.(27)
0(27)
47
0
(5)
(2%)
40%)
100
Cheese
E
17
DE
Q3
SQ +
Chemo +
Q4
SQ+
Chemo
Pembro
Pembro
Pembro
Pembro
100
55)
n - 50)
100
(n
$1)
(n = 49)
Events
Events
80
80
PFS Probability (%)
Median
PFS
by
SICR
(15%
CI),
no
8.4.(5.6-10.8)
PFS Probability (%)
Medium
PFS
by
BICR,
CI),
mo
60
Understitied HR CI)
0.46 (0.27.0.80)
60
Unitratied HR 30%
99)
40
40
20
20
0
0
0
2
4
6
8
10
12
14
16
18
20
22
24
26
28
30
0
2
I
6
8
10
12
14
16
18
20
22
24
26
28
30
Time (months)
Time (months)
No. (renth)
No. (reats)
(1)
(21)
2(21)
1.(21)
9(25)
49(2)
42.07)
4(22)
2 (22)
1(22)
1027)
(22)
Cheme
postro
50
Rd
44
(53)27
2022
6(32)
402)
2.00
104)
9(34)
Chemo
permites
a
100
(34)
200
-
0.00
SG + pembro treatment was associated with consistently improved PFS vs chemo + pembro
across Trop-2 expression quartiles, with trends toward greater separation of KM curves in Q3 and Q4
*Trop-2 B-score parties Q1 0-224; 12 225-279 Q3, 280-298 04 259-300
BICR blinded independent central review chemo chemotherapy HR harand ratio, KM Kaplan Moior, mo months NE not entimable pembro, PFS progression from survival; Q. quartile; SG, sachanamab govitecan
2026 ASCO
#ASCO26
иа SUNTED RY Sara M Tolaney, MD, MPH, FASCO
ASCO
AMERICAN
CLINICAL
ANNUAL MEETING
Presentation " property the who and ABCO Permission - to - COMMET
KNOWLEDGE CONQUERS CANCER
---
[Slide 4]
PFS by tBRCA Subgroups
Mut
SG + Pembro Chemo + Pembro
WT
(n 39)
(n 32)
SG + Pembro
Chemo + Pembro
Events
18
16
(n 130)
(n 131)
Median PFS by BICR (95% CI), mo
16.6
12.9
100
Events
69
90
100
(7.5-NE)
(7.1-NE)
9.6
Median PFS by BICR (95% CI), mo
7.4
Unstratified HR (95% CI)
0.88 (0 45-1.74)
(7.6-16.7)
(6.9-9.2)
Unstratified HR (95% CI)
0.67 (0.49-0.91)
80
80
PFS Probability (%)
60
60
40
PFS Probability (%)
40
20
20
0
0
0
2
4
6
8
10
12
14
16
18
20
22
24
26
0
2
4
6
8
10
12
14
16
18
20
22
24
26
Time (months)
Time (months)
No. at nsk
No. at risk
WT so persons
130
119
130
78
58
42
50
15
WT. Chemo person
113
ED
"
:
:
0
Mill SG permites
39
36
33
28
21
16
11
10
131
R
71
47
R
21
15
13
1
0
Mut, Chemo permises
32
30
29
22
19
14
9
=8
6
2
0
0
0
0
0
PFS improvement with SG + pembro vs chemo + pembro was observed across tBRCA subgroups
BICR blinded independent central review, chemo, chemotherapy, HR. hazand ratio, mBC, metastate breast cancer, me, months, mut mutant, NE, not estimable pembro, pembrolizume PFS, progression tree survival, SG, sectuzumab govitecan IBRCA
humor BRCA WT. wid type
2026 ASCO
#ASCO26
na SENTED BY Sara M Tolaney, MD. MPH, FASCO
ASCO
ENCOLOGY
ANNUAL MEETING
Presentation is property the who and AACO Permission - for - contact permissions@ass.org.
ENOWLEDGE CONQUERS CANCER
PFS2 & Subsequent Therapies#ASCO26 · Kalinsky
A separate ASCO 2026 readout (Kalinsky): progression-free survival after the next line of therapy (PFS2). Median PFS2 was not reached with SG + pembro vs 21.0 months with chemo + pembro (stratified HR 0.67, 95% CI 0.48–0.95) — the benefit held despite a high rate of crossover from the control arm to SG, with longer time to first and second subsequent therapies.
[Slide 1]
Key Takeaway Points:
ASCENT-04 PFS2 and Subsequent Therapies
In the ASCENT-04 study, PFS2 was longer in the SG + pembro group
compared with the chemo + pembro group, indicating sustained
long-term benefit beyond first progression
Despite the high rate of crossover from the control group to SG, time to first and
second subsequent therapies suggest that participants receiving 1L SG + pembro
experience longer initial disease control and delayed need for subsequent therapy
These results support SG + pembro as a new 1L standard of care
for patients with PD-L1+ mTNBC
1L first ino, chemo, chemotherapy; mTNBC metastatic triple negative broast cancor, PD-L1, programmed death ligand 1, pembro, pembrolizumab PFS2 progression froo survival 2. SG sactuzumab govtecan
2026 ASCO
#ASCO26
PNI SENTED BY: Kevin Kalinsky, MD, MS, FASCO
ASCO
ANNUAL MEETING
Presentation - property of the author and ASCO Permission required for reuse, contact permissora@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 2]
PFS After Next Line of Treatment (PFS2)
100
90
71.9% (95% CI, 64.5-78.0)
80
63.7% (95% CI, 51.1-73.9)
70
Event-Free Probability (%)
60
50
+++
40
53.0% (95% CI, 44.5-60.8)
45.6% (95% CI, 35.6-55.1)
30
SG Pembro
Chemo + Pembro
(n 221)
(n 222)
20
PFS2 events, n
55
83
10
Median PFS2, months (95% CI)
NR (NR-NR)
21.0 (16.0-NR)
Stratified HR (95% CI)
0.67 (0.48-0.95)
0
0
2
4
6
8
10
12
14
16
18
20
22
24
26
28
30
Time (months)
No. of Patients Still at Risk (Events)
SG pembro
221 (0)
216(5)
209 (12)
205 (16)
186 (25)
154 (33)
128 (41)
97 (48)
76 (52)
(52)
31 (54)
17 (54)
12 (55)
5 (55)
1 (55)
(55)
Chemo pembro
222(0)
218(2)
213(7)
208(11)
186 (21)
154 (39)
129 (49)
101 (59)
70 (74)
46 (79)
32 (80)
16 (83)
10 (83)
5
(83)
0(83)
PFS2 was longer in the SG + pembro group compared with the chemo + pembro group despite the high rate of
crossover in the chemo + pembro group, with a 33% reduction in risk of a PFS2 event with SG + pembro
*PFS2 is defined as time from randomization to first documented progression on next line therapy per investigator assessment, or death due to any cause, whichever occurred first
Chemo, chemotherapy HR hazard ratio, NR not reached pembro perbrolizumab PFS2 progression from survival 2. SG sactuzumab govitecan
2026 ASCO
#ASCO26
PM SENTED BY: Kevin Kalinsky, MD, MS, FASCO
ASCO
AMERICAN
CIRICAL DRICOLOGY
ANNUAL MEETING
Presentation property of the author and ASCO Permission required for - contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
:
---
[Slide 3]
Subsequent Therapy
Subsequent Therapies in the Second Line
Subsequent Therapies in the Third Line
Chemo +
Chemo +
SG + Pembro
SG + Pembro
Pembro
Pembro
(n = 221)
(n = 221)
(n = 222)
(n = 222)
Any subsequent therapy, n
69
119
Any subsequent therapy, n
69
119
Any subsequent therapy in 2L,a n (%)
68 (99)b
119 (100)
Any subsequent therapy in 3L,a n (%)
18 (26)b
29 (24)
Taxanes
23 (33)
8 (7)
Taxanes
5 (7)
3 (3)
Platinum agents
18 (26)
3 (3)
Anthracyclines
4 (6)
2 (2)
ADC
7 (10)
94 (79)
Platinum agents
3 (4)
5 (4)
Trastuzumab deruxtecan
5 (7)
2 (2)
ADC
2 (3)
6 (5)
Sacituzumab govitecan
2 (3)
92 (77)c
Trastuzumab deruxtecan
2 (3)
3 (3)
PD-(L)1 inhibitors
6 (9)
7 (6)
Sacituzumab govitecan
0 (0)
3 (3)e
Anthracyclines
4 (6)
5 (4)
PD-(L)1 inhibitors
1 (1)
2 (2)
PARPi
3 (1)
1 (1)
PARPi
0 (0)
1 (1)
Otherd
40 (58)
14 (12)
Other
11 (16)
18 (15)
Median TFST, months (95% CI)
17.3 (12.7-NR)
9.8 (8.7-10.9)
Median TSST, months (95% CI)
NR (22.9-NR)
21.0 (16.6-NR)
Stratified HR (95% CI)
0.59 (0.46-0.76)
Stratified HR (95% CI)
0.82 (0.59-1.14)
The majority of participants on chemo + pembro received 2L SG; in the SG + pembro group, most received 2L chemo.
Long-term benefit was observed with SG + pembro VS chemo + pembro, with substantially longer median time to
second subsequent treatment, despite high crossover rates
Percentages are calculated based on the number of participants who received any subsequent therapy "One participant who received any subsequent therapy did not have the line of therapy documented and was excluded from the second line- and third line-
specific analyses Includes both commercial use of SG in 2L (n 15) and crossover to SG on study (n 77) Includes capecitabine (n 20). gemcitabine and bevacizumab (n 7 each), cyclophosphamide (n 3), enbulin (n 2); enbulin mesylate, etoposide,
gemcitabine hydrochlonde, investigational agent, letrozole, ribociclib, trastuzumab, and vinorelbine (n =1 each) in the SG pembro group and cyclophosphamide (n 6), capecitabine (n 4); gemcitabine (n 2); bevacizumab and enbulin mesylate (n 1 each)
in
the chemo+ pembro group. *One patient in the chemo pembro group received SG beyond 3L Includes cyclophosphamide (n 3), capecitabine and bevacizumab (n 2 each); and enbulin, gemcitabine, vinorelbine, enbulin mesylate, fluorouracil,
pertuzumab/trastuzumab, and investigational drug (n each), in the SG pembro group, and capecitabine and enbulin (n 4 each); gemcitabine and cyclophosphamide (n 2 each); and bevacizumab, vinorelbine, Bt 8009, gemcitabine hydrochlonde, letrozole,
regoratenib, and investigational agent (n 1 each) in the chemo pembro group 2L second Ine; 3L third line; ADC antibody drug conjugate; chemo, chemotherapy, HR, hazard ratio, NR, not reached, PARPI, poly ADP nbose polymerase inhibitor, PD-(L)1,
programmed death (ligand) 1, pembro, pembrolizumab SG, sacituzumab govitecan, TFST, time to first subsequent therapy, TSST, time to second subsequent therapy
2026 ASCO
#ASCO26
PRESENTED BY: Kevin Kalinsky, MD, MS, FASCO
ASCO
AMERICAN SOCIETY or
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 4]
Conclusions
PFS2 was improved in the SG + pembro group compared with the
Median PFS2
chemo + pembro group despite the high rate of crossover, indicating
NR VS 21.0 months
sustained long-term benefit beyond first progression
HR, 0.67 (95% CI, 0.48-0.95)
Subsequent therapy in any line
The most frequent 2L+ subsequent therapy was chemo in the
Chemo + pembro group: SG (81%)
SG + pembro group and SG in the chemo + pembro group
SG + pembro group: chemo (88%)
Despite the high rate of crossover from the control group to SG,
Median TFST & TSST
time to first and second subsequent therapies suggest that
TFST: 17.3 VS 9.8 months
participants receiving 1L SG + pembro experience longer initial
TSST: NR VS 21.0 months
disease control and delayed need for subsequent therapy
These results from the ASCENT-04 study further support 1L SG + pembro use
for patients with PD-L1+ mTNBC
1L first line, 2L+, second line and later, chemo, chemotherapy, HR, hazard ratio, mTNBC, metastatic triple negative breast cancer, NR, not reached, PD-L1, programmed cell death ligand 1. pembro pembrolizumab; PFS2, progression- free survival 2; SG,
sacituzumab govitecan, TFST, time to first subsequent therapy, TSST, time to second subsequent therapy
2026 ASCO
#ASCO26
PRE SENTED BY: Kevin Kalinsky, MD, MS, FASCO
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
[Slide 1]
ASCENT-04/KEYNOTE-D19: Study Design
Treatment was continued until BICR-verified
progression or unacceptable toxicity
SG + pembroᶜ
Previously untreated, locally
(SG 10 mg/kg IV, days 1 and 8 of 21-day cycles;
advanced unresectable, or
Local standard of care
N = 443
pembro 200 mg, day 1 of 21-day cycles)
metastatic TNBCᵃ.b:
n = 221
R
PD-L1+ (CPS ≥ 10)
1:1
≥ 6 months since treatment
Chemo + pembroᶜ
Participants offered 2L SG
in curative setting (prior
(paclitaxel OR nab-paclitaxel
monotherapy provided through
anti-PD-[L]1 use allowed)
OR gemcitabine + carboplatin)
study® following BICR-verified
n = 222
disease progression
Primary end point: PFS by BICRd
Secondary end points: OS, ORR, and DOR by
BICRd; Safety; QOL
Exploratory end points included PFS2, TFST, and TSST
Clinical Trials gov identifier NCT05382286 *TNBC status determined according to standard American Society of Clinical Oncology College of American Pathologists cntena Up to 35% de novo m INBC Pembro was administered for a maximum of 35 cycles
Per RECIST v1 Participants could have also received SG in any subsequent line commercially; other subs treatments per local practice were also permitted.
2L, second-line; BICR, blinded independent central review, chemo, chemotherapy, CPS, combined positive score DOR, duration of response IV. intravenously, mTNBC metastatic triple-negative breast cancer, ORR, objective response rate; OS, overall
survival; PD-(L)1, programmed cell death (ligand) 1; pembro, pembrolizumab; PFS, progression free survival; PFS2, progression free survival 2; QOL quality of life, R. randomized, RECIST v1.1, Response Evaluation Criteria in Solid Tumors, version 1.1; SG,
sacituzumab govitecan, TFST, time to first subsequent therapy, TNBC, triple negative breast cancer, TSST, time to second subsequent therapy
2026 ASCO
#ASCO26
PRE SENTED BY: Kevin Kalinsky, MD, MS, FASCO
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 2]
Participant Disposition and Subsequent Treatment
SG +
Chemo +
SG +
Chemo +
Participants who discontinued
Participant Disposition, n (%)
Pembro
Pembro
Pembro
Pembro
first-line treatment,* n (%)
(n = 221)
(n = 222)
(n = 125)
(n = 170)
Received second-line or later
Remaining on study treatment
95 (43)
52 (23)
69 (55)
119 (70)
therapy
Discontinued treatment
125 (57)
170 (77)
Received any subsequent ADC
13 (19)
97 (82)
Received any subsequent SG°
3 (4)
96 (81)
Progressive diseaseᵇ
84 (67)
138 (81)
Received third-line therapy
18 (14)
29 (17)
*Data are based on the primary analysis data-cut and follow-up is ongoing.
Almost twice as many participants in the SG + pembro group (43%) remained on study treatment
compared with the chemo + pembro group (23%) at the time of data cutoff
*In the SG pembro group, treatment discontinuation was also due to participant decision (n 20), adverse events (n = 11); death (n 6), investigator choice (n - 3), and non compliance with study drug (n - 1), in the chemo pembro group, treatment
discontinuation was due to adverse events (n 14), participant decision (n 13); non-compliance with study drug and death (n 2 each); and investigator choice (n 1). Percentages are calculated based on the number of participants who discontinued treatment
Percentages are calculated based on the number of participants who received second line or later therapy
ADC, antibody-drug conjugate; chemo, chemotherapy, pembro, pembrolizumab; SG, sacituzumab govitecan
2026 ASCO
#ASCO26
PRESENTED BY: Kevin Kalinsky, MD, MS, FASCO
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 3]
PFS After Next Line of Treatment (PFS2)
100
90
71.9% (95% CI, 64.5-78.0)
80
63.7% (95% CI, 51.1-73.9)
70
Event-Free Probability (%)
60
50
##
40
53.0% (95% CI, 44.5-60.8)
45.6% (95% CI, 35.6-55.1)
30
SG + Pembro
Chemo + Pembro
(n = 221)
(n = 222)
20
PFS2 events, n
55
83
10
Median PFS2," months (95% CI)
NR (NR-NR)
21.0 (16.0-NR)
Stratified HR (95% CI)
0.67 (0.48-0.95)
0
0
2
4
6
8
10
12
14
16
18
20
22
24
26
28
30
Time (months)
No. of Patients Still at Risk (Events)
SG + pembro
221 (0)
216 (5)
209 (12)
205 (16)
186 (25)
154 (33)
128 (41)
97 (48)
76 (52)
48 (52)
31 (54)
17 (54)
12 (55)
5 (55)
1 (55)
0 (55)
Chemo
pembro
222 (0)
218 (2)
213 (7)
208 (11)
186 (21)
154 (39)
129 (49)
101 (59)
70 (74)
46 (79)
32 (80)
16 (83)
10 (83)
5 (83)
0 (83)
PFS2 was longer in the SG + pembro group compared with the chemo + pembro group despite the high rate of
crossover in the chemo + pembro group, with a 33% reduction in risk of a PFS2 event with SG + pembro
*PFS2 IS defined as time from randomization to first documented progression on next-line therapy per investigator assessment, or death due to any cause, whichever occurred first
Chemo, chemotherapy; HR, hazard rabo, NR, not reached, pembro, pembrolizumab; PFS2, progression free survival 2; SG, sacituzumab govitecan
2026 ASCO
#ASCO26
PRE SENTED BY: Kevin Kalinsky, MD, MS, FASCO
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 4]
Key Takeaway Points:
ASCENT-04 PFS2 and Subsequent Therapies
In the ASCENT-04 study, PFS2 was longer in the SG + pembro group
compared with the chemo + pembro group, indicating sustained
long-term benefit beyond first progression
Despite the high rate of crossover from the control group to SG, time to first and
second subsequent therapies suggest that participants receiving 1L SG + pembro
experience longer initial disease control and delayed need for subsequent therapy
These results support SG + pembro as a new 1L standard of care
for patients with PD-L1+ mTNBC
1L, first line; chemo, chemotherapy, mTNBC, metastatic triple-negative breast cancer, PD-L1, programmed death ligand 1; pembro, pembrolizumab; PFS2, progression free survival 2; SG, sacituzumab govitecan
2026 ASCO
PRESENTED BY: Kevin Kalinsky, MD, MS, FASCO
ASCO
AMERICAN SOCIETY OF
#ASCO26
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
Patient-Reported Outcomes & Quality of LifeESMO 2025 · de Azambuja
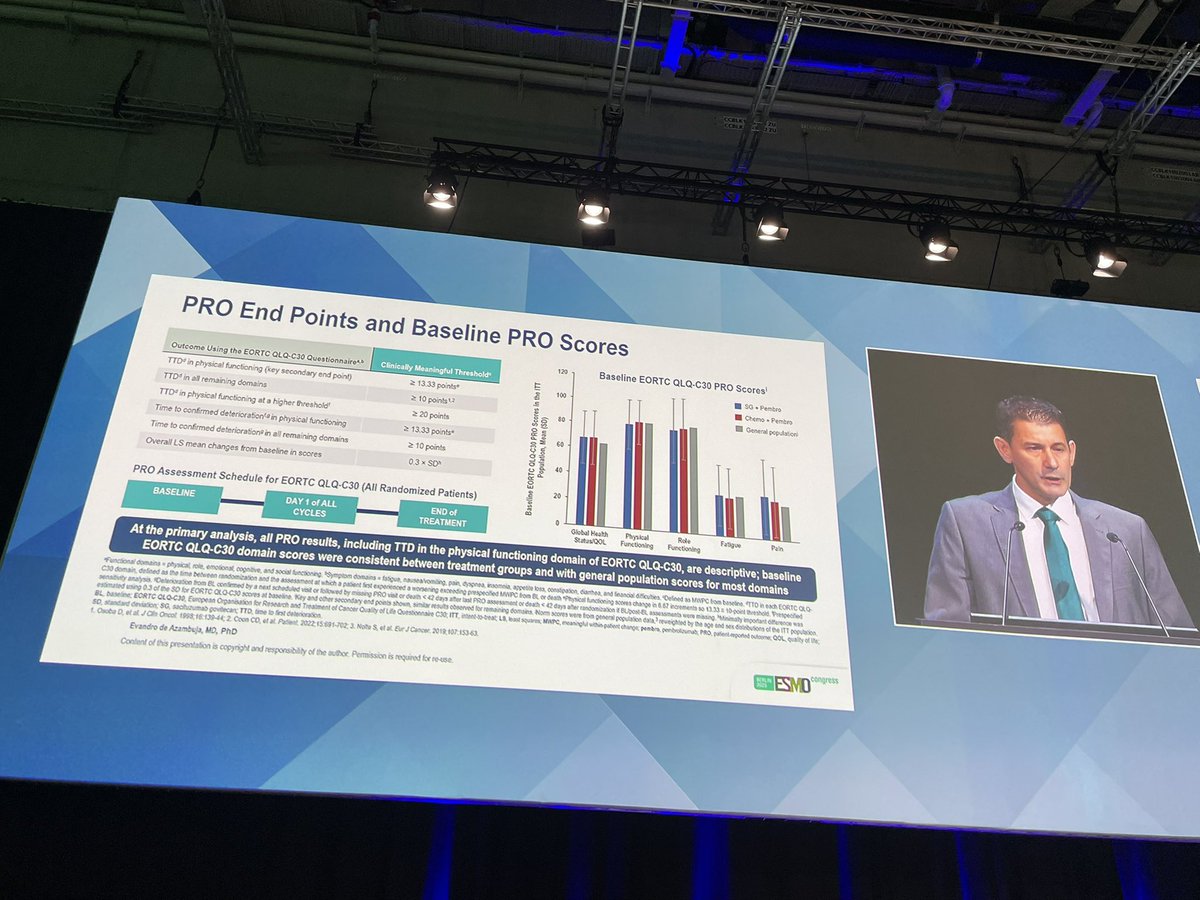
The ESMO 2025 PRO/QoL analysis (de Azambuja, Oct 20 2025): patient-reported outcomes on the EORTC QLQ-C30. Time-to-deterioration in physical functioning (key secondary) and the remaining domains, with baseline scores consistent between arms and with the general population.
[Slide 1]
ASCENT-04/KEYNOTE-D19: Study Design
Treatment was continued until BICR-verified
progression or unacceptable toxicity
End points
Previously untreated, locally
SG pembro
Primary
advanced unresectable, mTNBC:
(SG 10 mg/kg IV, days 1 and B of 21-day
PFS by BICR
cycles; pembro 200 mg, day 1 of 21-day cycles)
PD-L1+ (CPS 2 10)
n 221
R
Secondary
> 6 months since treatment in
1:1
OS
curative setting (prior anti-PD-
Chemo + pembro*,ᵇ
ORR, DOR by BICR
[L]1 use allowed)
(paclitaxel OR nab-paclitaxel
Safety
N 443
OR gemcitabine carboplatin)
QOL
Evandro de
n 222
- TTD in physical functioning
Azambuja
"Eligible patients who experienced BICR-verified disease
(key secondary)
progression were offered crossover to 21. SG monotherapy
- TTD in role functioning,
Patent reported outcomes (PROv) with recount govifecen (6G) .
Stratification factors
GHS/QOL, pain, and fatigue
(pembre) VII chemotherapy (chemo) . pembre in
De nove* vs recurrent mTNBC within 6 to 12 months
US/Canada/Western
Prior exposure to and-
(other secondary)
DECEPTS (ams) with previously undreaded POL metastate vom
from treatment completion in curstive setting vs recument > 12 months from
Europe vs the rest of
PD-(L)1 (yes is no)
1per the EORTC QLQ-C30
treatment completion in curative setting
the world
regative
breast
cancer
TNIC)
in
the
phase
12
ASCENT-GAINE
CiricalTrials gov dentiler NCT05382286 Data outsiff was March 3. 2025
up to 35% de novo mINSC Fembro was administered for # maximum of 35 cycles Administered per country specific prescribing information Per Response Evaluation Cellena n Sold Turnors version 11
21. second le BICR blinded independent central review, chemo, chemotherapy CPS combined positive score, DOR duration of response EORTC QLQ-C30 European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire
C30 GHS, global health status IV intravenously mTNBC metastatic Imple negative breast cancer ORR objective response - os overall survival PD-L1 programmed cell death-ligand 1, pembro perbrokzumab PFS progression-free survival,
PRO patient reported outcome, QOL quality of the R randomunation so sociturume govtecan, TTD time to first distenoration
Evandro de Azambuja, MD, PhD
Content of the presentation is copymght and responsibility of the author Permission is required for - use
ESMO
---
[Slide 2]
PRO End Points and Baseline PRO Scores
120
Baseline EORTC QLQ-C30 PRO Scores
Outcome Using the EORTC QLQ-C30 Questionnaire**
Clinically Meaningful Threshold
SG Pembro
TTD in physical functioning (key secondary end point)
2 13.33 points
100
Chemo Pembro
TTD in all remaining domains
2 10 points¹²
TTD in physical functioning at a higher threshold
> 20 points
Time to confirmed deterioration physical functioning
Baseline EORTC QLQ-C30 PRO Scores in the ITT
General population
80
2 13.33 points
Time to confirmed deterioration in all remaining domains
2 10 points
Population Mean (SD)
60
40
Overall LS mean changes from baseline in scores
0.3 SD
Evandro de
20
PRO Assessment Schedule for EORTC QLQ-C30 (All Randomized Patients)
Azambuja
BASELINE
DAY of ALL
END of
0
CYCLES
TREATMENT
Global Health
Physical
Role
Fatigue
Pain
Patient reported outcomes (PROs) with sacituzumab govitecan (SG) +
Status/QOL
Functioning
Functioning
pembrolizumab (pembro) vs chemotherapy (chemo) + pembro in
At the primary analysis, all PRO results, including TTD in the physical functioning domain of EORTC QLQ-C30, are descriptive; baseline
patients (ots) with previously untreated PD-L1 metastatic triple-
EORTC QLQ-C30 domain scores were consistent between treatment groups and with general population scores for most domains
negative breast cancer (mTNBC) in the phase III ASCENT-04/KE
Functional domains physical role emotional cognitive and social functioning Symptom domains fatigue, nausea/vomiting pain, dyspnea, insomnia appetite loss constipation, diarrhea, and financial difficulties Defined as MWPC from baseline TTD in each EORTC QLQ
C30 domain, defined as the time between randomization and the assessment at which a patient first experienced a worsening exceeding prespecified MWPC from BL or death Physical functioning scores change in 5.67 increments so 13.33 point threshold Prespecified
sensitivity analysis Reterioration from BL confirmed by next scheduled visit or followed by masing PRO vest or death 42 days after last PRO assessment or death days after randomization BL post BL assessments were missing Minimally important difference was
estimated using 0.3 of the SD for EORTC C30 scorts at baseline Key and other secondary end points shown similar results observed for remaining domains Nom scores wore from general population data reseighted by the age and sex distributions of the ITT population
BL baseline EORTC QLQ-C30 European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire C30; ITT. intent-to-beat LS least squares MWPC meaningful within patient change pembro pembrolizumab PRO patient reported outcome QOL quality of do:
SD. standard deviation SG sacituzumab govitecan, TTD time to first deterioration
1 Osoba D. of Cin Oncol 1998 16 139-44 2 Coon CD. et at Patient 2022,15 702 3 Note S et at Eur Cancer 15363
Evandro de Azambuja, MD, PhD
congress
Content of this presentation is copyright and responsibility of the author Permission is required for re-use
ESMO
---
[Slide 3]
Time to First Deterioration in Physical Functioning
100
13.33-Point MWPC Threshold
SG + Pembro
Chemo + Pembro
90
(m 221)
(n 222)
80
Median TTD* physical functioning
(95% CI), months
3.0(2.3-4.6)
3.5(2.9-4.2)
70
Stratified HR (95% CI)
0.95 (0.73-1.22)
Event-Free Probability (%)
60
so
40
30
20
10
0
0
2
4
6
8
10
12
14
16
18
20
22
24
26
No. of patients at risk (events)
Time (months)
SG permites
221(0)
105 (58)
66(98)
46(105)
27(111)
14(115)
11(115)
9(115)
5(118)
2(118)
2(118)
1(118)
1(118)
0 (118)
Chemo pembro
222(0)
111(59)
61(92)
34(129)
18(116)
10(118)
8(118)
4(118)
3(118)
2(118)
1(118)
1(118)
0(118)
TTD in physical functioning was maintained in the SG + pembro group and comparable between treatment groups
TTD defined as the time between randomization and the assessment at which a patient first experienced a worsening exceeding prespecified MWPC from BL or death
BL baseline chemo, chemotherapy CL confidence interval HR, hazand ratio, MWPC meaningful within patient change pembro, pembrolizumab SG, sacturumeb govitecan TTD time to first deterioration
Evandro de Azambuja, MD, PhD
Content of the presentation is copyright and responsibility of the author Permission is required for re-use
ESMO
congress
[Slide 1]
PRO End Points and Baseline PRO Scores
120
Baseline EORTC QLQ-C30 PRO Scores'
Outcome Using the EORTC QLQ-C30 Questionnaire**
Clinically Meaningful Threshold"
so Pembro
TTD in physical functioning (key secondary end point)
2 13.33 points*
100
Chemo Pembro
TTD in all remaining domains
2 10 points
TTD in physical functioning at a higher threshold
2 20 points
Time to confirmed detericration in physical functioning
2 13.33 points*
Time to confirmed deterioration in all remaining domains
2 10 points
Overall LS mean changes from baseline in scores
0.3 SD^
Baseline EORTC CLQ-C30 PRO Scores in the ITT
General population
80
Population, Mean (SD)
60
40
20
PRO Assessment Schedule for EORTC QLQ-C30 (All Randomized Patients)
BASELINE
DAY of ALL
END of
0
CYCLES
TREATMENT
Global Health
Physical
Role
Fatigue
Pain
Status/QOL
Functioning
Functioning
At the primary analysis, all PRO results, including TTD in the physical functioning domain of EORTC QLQ-C30, are descriptive; baseline
EORTC QLQ-C30 domain scores were consistent between treatment groups and with general population scores for most domains
Functional domains physical role, emotional copitive, and social functioning Symptom domains fingue, naissa/voming pain dyspnea, informa, appetite loss, constipation, diarthea, and feancial difficulties Defined as MAPC form basedes TTO in sich CORTC ao
C30 domain, defined as the time between informization and the assessment at which patient lirst experienced worsening exceeding prespecified MWPC from BL or death Physical functioning sooms change 6.62 increments 50 13.33 10-point threshold Prespecified
sensitivity analysis. Delerioration from BL confirmed by next scheduled visit or followed by maing PRO visit or death 42 days after last PRO assessment or death 42 days after randomization BUpost EL assessments were masing Minimally important difference ***
estimated using 0.3 of the so for EORTC OLO-C30 accres at baseline Key and other secondary end points shown, similar results observed for remaining domains Nom accres vere for general population data, reveighted by the age and sex distributions of the ITT population
BL baseline; ECRTC CLO-CIO, European Organisation for Research and Treatment of Cancer Quality of - Questionnaire C30 ITT, intent to DNK LB, least squares, MAPC, encaninglul within pabert change pembra PRO. patient reported but OOL quality of We
so, standard devision; so, sachuzumab povitecar; TTD. time to liest deterioration,
1. Osoba D, etal Ch Oncol 1993, 139-44;2 Coon CO, of at Patient 2022; 15.691-702; 3. Note 5, et at Evr Cancer 2019, 15363
Evandro de Azambuja, MD, PhD
Content of this presentation is copyright and responsibility of the author Permission is required for re-use.
congress
ESMO
---
[Slide 2]
Time to First Deterioration in Physical Functioning
100
13.33-Point MWPC Threshold
SG + Pembro
Chemo + Pembro
90
(n 221)
(n 222)
80
Median TTD* physical functioning
(95% CI), months
3.0(2.3-4.6)
3.5(294.2)
70
Stratified HR (95% CI)
0.95 (0.73-1.22)
Event-Free Probability (%)
60
50
40
30
20
10
0
0
2
4
6
8
10
12
14
16
18
20
22
24
26
No. of patients at risk (events)
Time (months)
SG pembro
221(0)
105(68)
66(98)
46(105)
27(111)
14(115)
11(115)
9(115)
5(118)
2(118)
2(118)
1(118)
1(118)
0(118)
Chemo pembro
222(0)
111(59)
61(92)
34(109)
18(116)
10(118)
$(118)
4(118)
3(118)
2(118)
1(118)
1(118)
0(118)
TTD in physical functioning was maintained in the SG + pembro group and comparable between treatment groups
TTD defined as the time between randomization and the assessment at which a patient first experienced a worsening exceeding prespecified MMPC from BL or death,
BL, baseline; chemo, chemotherapy, CI, confidence interval; HR, hazard ratio, MWPC, meaningful within-patient change; pembro, pembrolizumab; SG, sacituzumeb govitecan; TTD, time to first deterioration
Evandro de Azambuja, MD, PhD
Content of this presentation is copyright and responsibility of the author. Permission is required for re-use
ESMO
congress
---
[Slide 3]
Time to First Deterioration in EORTC QLQ-C30 Domains
Median (95% CI)
Median (95% CI)
TTD,* Months
TTD,* Months
ITT Population
SG + Pembro (n= 221)
Chemo + Pembro n - 222)
HR (95% City*
HR (95% CIP
Global health status/QOL
2.2(2.1-3.3)
35(2342)
0.98(0.75-1.27)
Physical functioning
3.0(2.34.6)
3.5(294.2)
0.95(073-1.22)
Role functioning
1.7.(1.1-2.2)
1.5(1,4-2.3)
1.01(0.79-1.29)
Emotional functioning
9.3 (5.9-NE)
49(3563)
Cognitive functioning
23(1.53.5)
29(223.5)
0.96(0.74-1.23)
Social functioning
1.9(1.5-2.2)
2.2(1.53.3)
1.02(0.80-1.31)
Fatigue
1.1(1.0-1.4)
1.0(0.9-1.4)
0.91(0.72-1.15)
Nausea/vomiting
1.5(1,0-2.2)
3.5(2,1-4.4)
1.38(1.07-1.77)
Pain
43(245.7)
3.2(2.24.2)
Dyspnea
4.7(3.1-6.7)
3.7(2.8-5.6)
0.88(0,67-1.16)
Insomnia
5.6(3.7-10.8)
3.5(2,8-4.4)
0.75(0.56-1.00)
Appetite loss
2.2(1.7-3.0)
4.2(2,9-5.6)
1,25 (0.96-1.64)
Constipation
28(21-3.5)
3.7(24-5.1)
1.07 (0.82-1.39)
Diarrhoa
1.4(1.0-1.8)
5.3(3,1-6.9)
1.92(1.48-2.43)
Financial difficultes
7.6(4.2-13.6)
9.3(5.7-NE)
1,16 (0.85-1.59)
05
1
pembro better
Chemo pembro better
QOL was generally maintained for a similar duration in both treatment groups; consistent results were observed in the analysis for TTCDc
TD in each EORTC QLQ-CJO domain defined as the time between randomization and the assessment at which patient first experienced worsening exceeding prespecified MAPC bon a or death MR Envors SG pembro Deterioration from
BL confirmed by next scheduled visit or followed by masing PRO visit or death 42 days after last PRO assessment or death 42 days after randomization BL post& assessments were missing
BL baseline; chemo, chemotherapy, CL confidence interval EORTC QLQ-C30, European Organisation for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30; HR Assed no, ITT, intent to beat, MAPC, meaninglul within
patient change, NE, not estimable pembro, pentrolaumab DOL, quality of the $0, sociluzumab government TTCD. time to confirmed deterioration TTO, time to first deterioration
Evandro de Atambuja, MO, PhD
Content of this presentation is copyright and responsibility of the author, Permission is required for N-050
ESMO
congress
---
[Slide 4]
Conclusions
Baseline QOL was generally maintained with SG + pembro, with benefits seen in several domains
TTD in physical functioning was comparable between the groups, with emotional functioning and pain favoring SG .
pembro VS chemo + pembro
The sensitivity analyses to evaluate substantial and sustained changes showed that SG . pembro may delay the onset of
decline in physical functioning, indicating a benefit in maintaining patients' ability to perform daily activities
Mean changes from baseline favored SG + pembro for physical, role, and emotional functioning, as well as pain and
insomnia
There was worsening of symptoms such as nausea/vomiting and diarrhea, which are consistent with the safety profile of
the SG + pembro group in the study, and can be managed by following established guidelines
SG + pembro maintained overall QOL, patients reported reduced symptom burden and improved functioning in multiple
domains; these data complement the clinically meaningful improvement in PFS and support this treatment regimen as a
potential new standard of care for patients with PD-L1+ mTNBC
Chemo, chemotherapy, pembro, PFS, progression free survive QOL quality of Me, so, sacitazumeb povitecary TTD, time as first deterioration
Evandro de Azambuja, MD, PhD
Content of his presentation is copyright and responsibility of the author Permission is required for re-use, -
ESMO
congress
Primary PFS ReadoutASCO 2025 · LBA109
The ASCO 2025 primary analysis (Tolaney, LBA109, May 31 2025; simultaneous NEJM publication): the registrational PFS, response, and safety data that established the first-line benefit in PD-L1+ mTNBC.
[Slide 1]
2025
ASCO
ANNUAL MEETING
Sacituzumab Govitecan Plus Pembrolizumab vs Chemotherapy
Plus Pembrolizumab in Patients With Previously Untreated,
PD-L1 Positive, Advanced or Metastatic Triple-Negative Breast
Cancer: Primary Results From the Randomized, Phase 3
ASCENT-04/KEYNOTE-D19 Study
Sara M Tolaney¹, Evandro de Azambuja², Kevin Kalinsky³, Sherene Loi4, Sung-Bae Kim⁵, Clinton Yam®,
Bernardo Rapoport7,8, Seock-Ah Im9, Barbara Pistilli¹⁰, Wassim McHayleh11, David W Cescon¹², Junichiro Watanabe¹³,
Manuel Alejandro Lara Banuelas14, Ruffo Freitas-Junior¹⁵, Javier Salvador Bofill¹⁶, Maryam Afshari17, Dianna Gary17, Lu
Wang¹⁷, Catherine Lai¹⁷, Peter Schmid¹⁸
Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA, USA; Institut Jules Bordet, Hôpital Universitaire de Bruxelles (H.U.B) and Université Libre de Bruxelles (ULB), Brussels,
Belgium; Winship Cancer Institute, Emory University, Atlanta, GA, USA: Peter MacCallum Cancer Centre, Melbourne, Australia; Asan Medical Center, University of Uisan College of Medicine,
Seoul, Republic of Korea: The University of Texas MD Anderson Cancer Center, Houston, TX, USA: The Medical Oncology Centre of Rosebank, Clinical and Translational Research Unit
(CTRU), Saxonwold, South Africa; Department of Immunology, Faculty of Health Sciences, University of Pretoria, Pretoria, South Africa: *Seoul National University Hospital, Cancer Research
Institute, Seoul National University College of Medicine, Seoul National University, Seoul, Republic of Korea; Department of Cancer Medicine, Gustave Roussy, Villejuif, France:
"AdventHealth Cancer Institute, Orlando, FL, USA; 12Princess Margaret Cancer Centre, UHN, Toronto, Canada; PJuntendo University Graduate School of Medicine, Tokyo, Japan; "Oncology
Center of Chihuahua, Chihuahua, Mexico: "CORA Advanced Center for Diagnosis of Breast Diseases, Federal University of Golás, Golânia, Brazil: "Medical Oncology Department, Hospital
Universitario Virgen del Rocio, Seville, Spain; "Gilead Sciences, Inc., Foster City, CA, USA; "Centre for Experimental Cancer Medicine, Barts Cancer Institute, Queen Mary University of
London, London, UK
RESENTED BY: Sara M Tolaney, MD, MPH
ASCO
AMERICAN
CUNICAL ONCOLOGY
2025 ASCO
#ASCO25
KNOWLEDGE CONQUERS CANCER
ANNUAL MEETING
Presentation property of the author and ASCO Permission required for - contact permissions@ass.org
---
[Slide 2]
ASCENT-04/KEYNOTE-D19 Study Design
Previously untreated, locally
SG + pembrod
End points
advanced unresectable, or
(SG 10 mg/kg IV, days 1 and 8 of 21-day
All treatment,
metastatic TNBCᵃ:
cycles; pembro 200 mg, day 1 of 21-day
Primary
cycles)
including SG
PFS by BICR®
PD-L1-positive (CPS ≥ 10 by
n = 221
or chemo, was
R
continued until
the 22C3 assayb)
1:1
BICR-verified
Secondary
≥ 6 months since treatment in
Chemo* + pembroᵈ
disease
OS
curative setting (prior anti-PD-
(paclitaxel 90 mg/m2 OR nab-paclitaxel
progression or
ORR, DOR by
[L]1 use allowed)
100 mg/m2 on days 1. 8, & 15 of 28-day cycles,
unacceptable
BICR
OR gemcitabine 1000 mg/m2 + carboplatin
toxicity
AUC 2 on days 1 & 8 of 21-day cycles; pembro
Safety
N = 443
200 mg on day 1 of 21-day cycles)
QoL
n = 222
Stratification factors:
De novo mTNBCc VS recurrent within 6 to 12 months from
*Eligible patients who experienced BICR-
completion of treatment in curative setting VS recurrent
verified disease progression were
> 12 months from completion of treatment in curative setting
offered to cross-over to
receive 2L SG monotherapy
US/Canada/Western Europe VS the rest of the world
Prior exposure to anti-PD-(L)1 (yes VS no)
ClinicalTrials gov identifier: NCT05382286.
TNBC status determined according to standard American Society of Clinical Oncology-College of American Pathologists criteria. Cako Againt Technologies. Up to 35% de novo mTNBC. Pembro was administered for a maximum of 35 cycles. *Per RECIST vt.1.
AUC. area under the curve; BICR, blinded independent central review, chemo, chemotherapy: CPS, combined positive score, DOR, duration of response, IV, intravenously, ORR, objective response rate, OS, overat survival, PD-L1, programmed cell death ligand 1: pembro,
pembrolizumab; PFS, progression-free survival; QoL, quality of tite; R, randomized; RECIST v1.1; Response Evaluation Criteria in Sold Tumors, version 1.1;SG, sackuzumab govitecan; TNBC, triple-negative breast cancer, TTR time-to-response
2025 ASCO
#ASCO25
PRESENTED BY: Sara M Tolaney, MD, MPH
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse; contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 3]
Progression-Free Survival by BICR
100
SG + Pembro
Chemo * Pembro
(n 221)
(л 222)
90
Number of PFS events
109
140
6 mo
80
Median PFS, mo (95% Ci)
11.2(9.3-16.7)
7.8(7,3-9.3)
Stratified HR (95% CI)
0.65(0.51-0.84)
Progression-Free Survival Probability (%)
70
P-value*
<0.001
12 mo
6-month PFS rate, % (95% CI)
72 (65-77)
63 (56-69)
60
12-month PFS rate, % (95% CI)
48 (41-56)
33 (26-40)
50
40
30
20
10
0
0
2
4
6
8
10
12
14
16
18
20
22
24
26
Time (months)
No. of Patients Still at Risk (Events)
SG Pembro
221 (0)
202 (11)
174 (33)
142 (59)
105 (75)
78 (89)
58 (96)
42 (98)
34 (99)
22 (103)
11 (106)
(109)
2
(109)
(109)
Chemo Pembro 222 (0)
191 (21)
159 (48)
123 (76)
88 (102)
59 (120)
40 (128)
29 (134)
21 (135)
13 (137)
7
(138)
4(138)
1 (139)
0(140)
SG + pembro demonstrated statistically significant and clinically meaningful improvement in PFS vs
chemo + pembro by BICR analysis, with a 35% reduction in risk of disease progression or death
Data cutoff date: March 3. 2025.
Two-sided P-value from stratified log rank test
BICR, binded independent central review, chemo, chemotherapy HR harard rate PFS, progression thee survival pentro, SG, sachuzumab govtecan
2025 ASCO
PRE SENTED BY: Sara M Tolaney, MD, MPH
ASCO
- SOCIETY or
CLINICAL CHECKED
#ASCO25
Presentation a property of the author and ASCO Permission required for - contact
KNOWLEDGE CONQUERS CANCER
ANNUAL MEETING
---
[Slide 4]
Conclusions
ASCENT-04/KEYNOTE-D19 is the first randomized, phase 3 study to evaluate the efficacy and safety
of an ADC/checkpoint inhibitor combination for first-line treatment of patients with PD-L1+ᵃ mTNBC
SG + pembro led to a statistically significant and clinically meaningful improvement in PFS VS chemo +
pembro (median 11.2 VS 7.8 months; HR, 0.65; 95% CI, 0.51-0.84; P < 0.001)
PFS benefit was observed across prespecified subgroups
OS data are immature, but an early trend in improvement was observed
ORR was higher (including an increased complete response rate), and responses were more durable
with SG + pembro VS chemo + pembro
The safety profile of SG + pembro was consistent with the established profiles of either agent; no
additive toxicity was observed
Results from ASCENT-04/KEYNOTE-D19 support the use of SG + pembro as a potential new standard of
care for patients with previously untreated, PD-L1+, locally advanced unresectable or metastatic TNBC
Data cutoff date: March 3, 2025
CPS 2 10 per HC 22C3 assay (Dako, Againt Technologies).
ADC, antibody drug conjugate; chemo, chemotherapy; CPS, combined positive score; DOR, duration of response; HR, hazard ratio, INC. immunohistochemstry; mTNBC; metastatic negative breast cancer; ORR, objective response rate: os, overall survivat, PD-L1,
programmed cell death ligand 1: pembro, pembrolizumab; PFS, progression-free survival; SG, sacituzumab govitecan; TNBC, triple-negative breast cancer
ASCO
AMERICAN SOCIETY OF
2025 ASCO
PRESENTED or: Sara M Tolaney, MD, MPH
CLINICAL ONCOLOGY
#ASCO25
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse: contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
[Slide 1]
ASCENT-04/KEYNOTE-D19 Study Design
Previously untreated locally
SG * pembro
End points
advanced unresectable, or
(SG 10 mg/kg IV, days 1 and * of 21-day
All treatment,
metastatic TNBC
cycles, pembro 200 mg, day 1 of 21-day
Primary
cycles)
including SG
Of chemo, was
PFS by BICR*
PD-L1-positive (CPS % 10 by
n 221
R
continued until
the 22C3 assay*)
1:1
BICR-verified
Secondary
2 6 months since treatment in
Chemo* * pembro
disease
OS
curative setting (prior anti-PD-
(pacitaxel 90 mg/m2 OR nab-pactitaxel
progression or
ORR, DOR by
[L]1 use allowed)
100 mg/m² on days 1,8, & 15 of 28-day cycles,
unacceptable
BICR*
OR gemcitabine 9000 mg/m3 + carboplatin
AUC 2 on days 14 a of 21-day cycles, pembro
toxicity
Safety
N 443
200 mg on day 1 of 21-day cycles)
QoL
Stratification factors:
15 = 222
De novo mTNBC VIII recurrent within G to 12 months from
"Eligible patients who experienced BICA-
completion of treatment n currative setting vs recurrent
verified disease progression were
12 months from completion of treatment in curative setting
offered to cross-over to
receive 2% SG monotherapy
US/Canda/Westentern Europe vsi the nest of the workd
Prior exposure to and-PD-(L)F (yes YTI no)
- -
- - - Increasive Code - - - - - - Technologies - - - - - - - . - the
mac - - - - - CPS - - - - - - - - - - - - - impress - - -
* I | I I I I . I I : I I I
2025 ASCO
#ASCO25
I I I = I
ASCO
ANNIVAL MEETING
-
I
|
KNOWLEDGE CONQUERS
---
[Slide 2]
Demographics and Baseline Characteristics
SG
Chemo +
SG
Chemo +
ITT Population
Pembro
Pembro
ITT Population
Pembro
Pembro
(n 221)
(n 222)
(n 221)
(n 222)
Female sex, n (%)
221 (100)
222 (100)
PD-L1 CPS > 10.d n (%)
221 (100)
222 (100)
Median age, (range) yr
54 (23-88)
55 (27-82)
Metastatic sites, n (%)
> 65 yr. n (%)
58 (26)
57 (26)
Lymph node
159 (72)
154 (69)
Race or ethnic group," n (%)
Lung
111 (50)
95 (43)
White
139 (63)
118 (53)
Bone
61 (28)
45 (20)
Asian
43 (19)
63 (28)
Liver
55 (25)
57 (26)
Black
13(6)
11 (5)
Brain
8 (4)
6 (3)
Other/not specified
26 (12)
30 (14)
Other
81 (37)
71 (32)
Geographic region, n (%)
US/Canada/Westen Europe
Chemo selected prior to randomization, n (%)
85 (38)
85 (38)
Taxane
Rest of the world
136 (62)
137 (62)
116 (52)
114 (51)
ECOG PS at baseline, n (%)
Gemcitabine/carboplatin
105 (48)
108 (49)
0
156 (71)
154 (69)
Prior anti-PD-(L)1 therapy, n (%)
9 (4)
11 (5)
1
65 (29)
67 (30)
Curative treatment-free interval, n (%)
De novo
75 (34)
75 (34)
Recurrent within 6-12 mo
40 (18)
40 (18)
Recurrent > 12 mo
106 (48)
107 (48)
Data cutoff date March 2025
*As reported by the patients "other" includes American indian or Alaska Native, other and not permitted Rest of the world includes Argentina, Australia Brank Case, Crech Republic Hang Kong Hungary israet Japan, Malaysia Mexico Poland Singapore, South Africa South
Korea Tateran and Turkey One patient the chemo pembro group had an ECOG PS 4PD-L status assessed using the PD-L INC 22C3 assay (Dako Agrent Technologies) at the time enrollment Other metastatic sides includes pleura, pleural effusion, skin, soft
Issue chest mat and muscle Actual chemo received was constitute with what was selected price to randomization however, two patients were randomined but as not receive treatment White 20 patients AGE included n the structified subgroup of prior exposure to anli-PD-
(LIT therapy (yes) per the IRT system only patients received prior treatment with anti-PD-(L)1 agents per the clinical database
Chemo chemotherapy CPS, combined positive score: ECOG PS, Eastern Cooperative Oncology Group performance status HC IRT. interactive response technology ITT. intent to-treat PARPI poly ADP-ribose polymerase inhibitor; PD-L1,
programmed cell death ligand pembro, pembrolizumab, SG, sachuzumab govitecan
2025 ASCO
#ASCO25
PRESENTED 3Y: Sara M Tolaney, MD. MPH
ASCO
AMERICA
CUNICAL ONCOLOGY
ANNUAL MEETING
Presentation property of - author and ASCO Permission name
KNOWLEDGE CONQUERS CANCER
---
[Slide 3]
Progression-Free Survival by BICR
100
SG + Pembro
Chemo + Pembro
(n 221)
(n 222)
90
Number of PFS events
109
6 mo
140
Median PFS, mo (95% CI)
11.2 (9.3-16.7)
7.8(7.3-9.3)
80
Stratified HR (95% CI)
0.65 (0.51-0.84)
Progression-Free Survival Probability (%)
70
P-value*
< 0.001
12 mo
6-month PFS rate, % (95% CI)
72 (65-77)
63 (56-69)
60
12-month PFS rate, % (95% CI)
48 (41-56)
33 (26-40)
50
40
30
20
10
0
0
2
4
6
8
10
12
14
16
18
20
22
24
26
Time (months)
No. of Patients Still at Risk (Events)
SG Pembro
221 (0)
202 (11)
174(33)
142(59)
105 (75)
78(89)
(96)
(98)
34 (99)
22 (103)
11 (106)
0 (109)
2 (109)
0 (109)
Chemo Pembro 222(0)
191 (21)
159 (48)
123(76)
88 (102)
59 (120)
40 (128)
(134)
21 (135)
13 (137)
7 (138)
4 (138)
1 (139)
0 (140)
SG + pembro demonstrated statistically significant and clinically meaningful improvement in PFS vs
chemo + pembro by BICR analysis, with a 35% reduction in risk of disease progression or death
Data cutoff sale March 3, 2025.
Two sided Please mom strated ing. name test
BICR blinded independent central review chemo, chemotherapy HR, harard - PFS progresson- mee survival periodo, SG, sachuzumab govitecan
2025 ASCO
#ASCO25
PRESENTED BY: Sara M Tolaney, MD, MPH
ASCO
AMERICAN socety or
CUNICAL ONCOLOGY
ANNUAL MEETING
Presentation property or - - - ABCO Perman - - - - perrissons@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 4]
Descriptive Overall Survival at Primary Analysis
100
90
80
70
Probability of Overall Survival (%)
60
50
40
SG + Pembro
Chemo + Pembro
30
(n 221)
(n . 222)
Number of os events
53
61
20
81% of patients who received any subsequent treatment
Median os, mo (95% CI)
NR (25.6-NR)
NR (NR-NR)
10
after discontinuation of chemo + pembro received SGª
HR (95% CI)
0.89 (0.62-1.29)
0
0
2
4
6
8
10
12
14
16
18
20
22
24
26
28
30
No. of Patients Still at Risk (Events)
Time (months)
SG Pembro
221(0)
216(5)
211(10)
206 (15)
190(23)
162 (28)
138(37)
111(41)
(46)
55(47)
36(50)
21(51)
14(52)
5(53)
1 (53)
0 (53)
Chemo Pembro 222(0)
218(2)
215(5)
210(10)
193(16)
166 (29)
142(34)
111(45)
87(53)
56(58)
38(60)
19(61)
11(61)
6(61)
0 (61)
OS data were immature (maturity rate, 26%), however,
a positive trend in improvement was observed for SG + pembro VS chemo + pembro
Date catelf date March 1. 2025 Median follow- was 14 months (range, 0 1-28.6)
FOR me 96 patients and received 80 monotherapy 35 subsequent annicancer merapy, 77 received . as part of the protocol specified crossover ofter meeting as crossover eligibility criteria, including BICR verification of disease progression the remaining 19 patients received
subsequent
-
monotherapy
-
commercial
supply
a. second line chemo, chemictherapy HR nazard rano, pembro, pembrolizumab NR not reached, os overall survival SG. sactuzumab goviecan
2025 ASCO
#ASCO25
PRESENTED BY: Sara M Tolaney, MD, MPH
ASCO
AMERICA or
CUNICAL ONCOLOGY
ANNUAL MEETING
Presentation property - author and ABCO Permission for
KNOWLEDGE CONQUERS CANCER
[Slide 1]
ASCENT-04/KEYNOTE-D19 Study Design
Previously untreated, locally
SG + pembrod
advanced unresectable, or
End points
metastatic TNBCᵃ:
(SG 10 mg/kg IV, days 1 and 8 of 21-day
cycles; pembro 200 mg, day 1 of 21-day
All treatment,
Primary
cycles)
including SG
PD-L1-positive (CPS ≥ 10 by
n = 221
or chemo, was
PFS by BICR®
R
the 22C3 assayb)
continued until
1:1
BICR-verified
Secondary
≥ 6 months since treatment in
Chemo* + pembroᵈ
disease
OS
curative setting (prior anti-PD-
(paclitaxel 90 mg/m2 OR nab-paclitaxel
progression or
[L]1 use allowed)
100 mg/m2 on days 1, 8, & 15 of 28-day cycles,
ORR, DOR by
unacceptable
BICR®
OR gemcitabine 1000 mg/m2 + carboplatin
AUC 2 on days 1 & 8 of 21-day cycles; pembro
toxicity
Safety
N = 443
200 mg on day 1 of 21-day cycles)
QoL
Stratification factors:
n = 222
De novo mTNBCc VS recurrent within 6 to 12 months from
*Eligible patients who experienced BICR-
completion of treatment in curative setting VS recurrent
verified disease progression were
> 12 months from completion of treatment in curative setting
offered to cross-over to
receive 2L SG monotherapy
US/Canada/Western Europe VS the rest of the world
Prior exposure to anti-PD-(L)1 (yes VS no)
ClinicalTrials gov identifier: NCT05382286
TNBC status determined according to standard American Society of Clinical Oncology-College of American Pathologists criteria. Cako Again Technologies. Up to 35% de novo mTNBC. Pembro was administered for a maximum of 35 cycles. *Per RECIST v1.1.
AUC, area under the curve; BICR, blinded independent central review; chemo, chemotherapy: CPS, combined positive score: DOR, duration of response: IV, intravenously, ORR, objective response rate; OS, overall survival; PD-L1, programmed cell death ligand 1; pembro,
pembrolizumab; PFS, progression-free survival; QoL., quality of life; R, randomized; RECIST v1.1; Response Evaluation Criteria in Sold Tumors version 1.1; SG, sacituzumab govitecan; TNBC, triple-negative breast cancer, TTR, time-to-response.
2025 ASCO
ASCO
AMERICAN SOCIETY OF
PRESENTED BY: Sara M Tolaney, MD, MPH
CLINICAL ONCOLOGY
#ASCO25
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse; contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 2]
Demographics and Baseline Characteristics
SG +
Chemo +
SG +
Chemo +
ITT Population
Pembro
Pembro
ITT Population
Pembro
Pembro
(n = 221)
(n = 222)
(n = 221)
(n = 222)
Female sex, n (%)
221 (100)
222 (100)
PD-L1 CPS ≥ 10,d n (%)
221 (100)
222 (100)
Median age, (range) yr
54 (23-88)
55 (27-82)
Metastatic sites, n (%)
≥ 65 yr, n (%)
58 (26)
57 (26)
Lymph node
159 (72)
154 (69)
Race or ethnic group,ᵃ n (%)
Lung
111 (50)
95 (43)
White
139 (63)
118 (53)
Bone
61 (28)
45 (20)
Asian
43 (19)
63 (28)
Liver
55 (25)
57 (26)
Black
13 (6)
11 (5)
Brain
8 (4)
6 (3)
Other/not specified
26 (12)
30 (14)
Other®
81 (37)
71 (32)
Geographic region, n (%)
Chemo selected prior to randomization, n (%)
US/Canada/Western Europe
85 (38)
85 (38)
Taxane
116 (52)
114 (51)
Rest of the worldb
136 (62)
137 (62)
Gemcitabine/carboplatin
105 (48)
108 (49)
ECOG PS at baseline,ᶜ n (%)
0
156 (71)
154 (69)
Prior anti-PD-(L)1 therapy,º n (%)
9 (4)
11 (5)
1
65 (29)
67 (30)
Curative treatment-free interval, n (%)
De novo
75 (34)
75 (34)
Recurrent within 6-12 mo
40 (18)
40 (18)
Recurrent > 12 mo
106 (48)
107 (48)
Data cutoff date: March 3, 2025. "other" includes American Indian or Alaska Native, other, and not permitted. Rest of the world includes Argentina, Australia, Brazil, Chile, Czech Republic, Hong Kong, Hungary, Israel, Japan, Malaysia, Mexico, includes Poland, Singapore, effusion, South skin, Afric
*As reported by the patients; One patient in the chemo pembro group had an ECOG PS ≥ 2. PD-L1 status assessed using the PD-L1 IHC 22C3 assay (Dako, Agailent Technologies) at the time of enrollment. *Other metastatic in the sites stratified pleura, of pleural exposure to an
Korea, chest Taiwan, wall, and and Turkey. muscle. Actual chemo received was consistent with what was selected prior to randomization; however, two patients were randomized but did not receive treatment. While 20 patients were included subgroup prior
(L)1 Chemo, tissue, therapy chemotherapy: (yes) per the CPS, IRT combined system, only positive 6 patients score; received ECOG PS, prior Eastern treatment Cooperative with anti-PD-(L)1 Oncology agents Group per performance the clinical database. status; IHC. mmunohistochemistry; IRT, interactive response technology. ITT, intent-to-treat PARPI, poly ADP-ribose polymerase inhibitor, PD-L1,
programmed cell death ligand 1; pembro, pembrolizumab; SG, sacituzumab govitecan.
PRESENTED BY: Sara M Tolaney, MD, MPH
ASCO
2025 ASCO
#ASCO25
KNOWLEDGE CC
Presentation is property of the author and ASCO. Permission required for reuse; contact permissions@asco.org
ANNUAL MEETING
---
[Slide 3]
Progression-Free Survival by BICR
100
SG + Pembro
Chemo + Pembro
90
(n 221)
(n = 222)
6 mo
Number of PFS events
109
140
80
Median PFS, mo (95% CI)
11.2 (9.3-16.7)
7.8 (7.3-9.3)
Progression-Free Survival Probability (%)
Stratified HR (95% CI)
0.65 (0.51-0.84)
70
P-value*
< 0.001
60
12 mo
6-month PFS rate, % (95% CI)
72 (65-77)
63 (56-69)
12-month PFS rate, % (95% CI)
48 (41-56)
33 (26-40)
50
40
30
20
10
0
0
2
4
6
8
10
12
14
16
18
20
22
24
26
Time (months)
No. of Patients Still at Risk (Events)
SG + Pembro
221 (0)
202 (11)
174 (33)
142 (59)
105 (75)
78 (89)
58 (96)
42 (98)
34 (99)
22 (103)
11 (106)
6 (109)
2 (109)
0 (109)
Chemo + Pembro 222 (0)
191 (21)
159 (48)
123 (76)
88 (102)
59 (120)
40 (128)
29 (134)
21 (135)
13 (137)
7 (138)
4 (138)
1 (139)
0 (140)
SG + pembro demonstrated statistically significant and clinically meaningful improvement in PFS vs
chemo + pembro by BICR analysis, with a 35% reduction in risk of disease progression or death
Data cutoff date: March 3, 2025.
*Two-sided P-value from stratified log-rank test.
BICR, blinded independent central review; chemo, chemotherapy; HR, hazard ratio; PFS, progression-free survival; pembro, pembrolizumab; SG, sacituzumab govitecan.
PRESENTED BY: Sara M Tolaney, MD, MPH
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
2025 ASCO
#ASCO25
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for rouse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
[Slide 4]
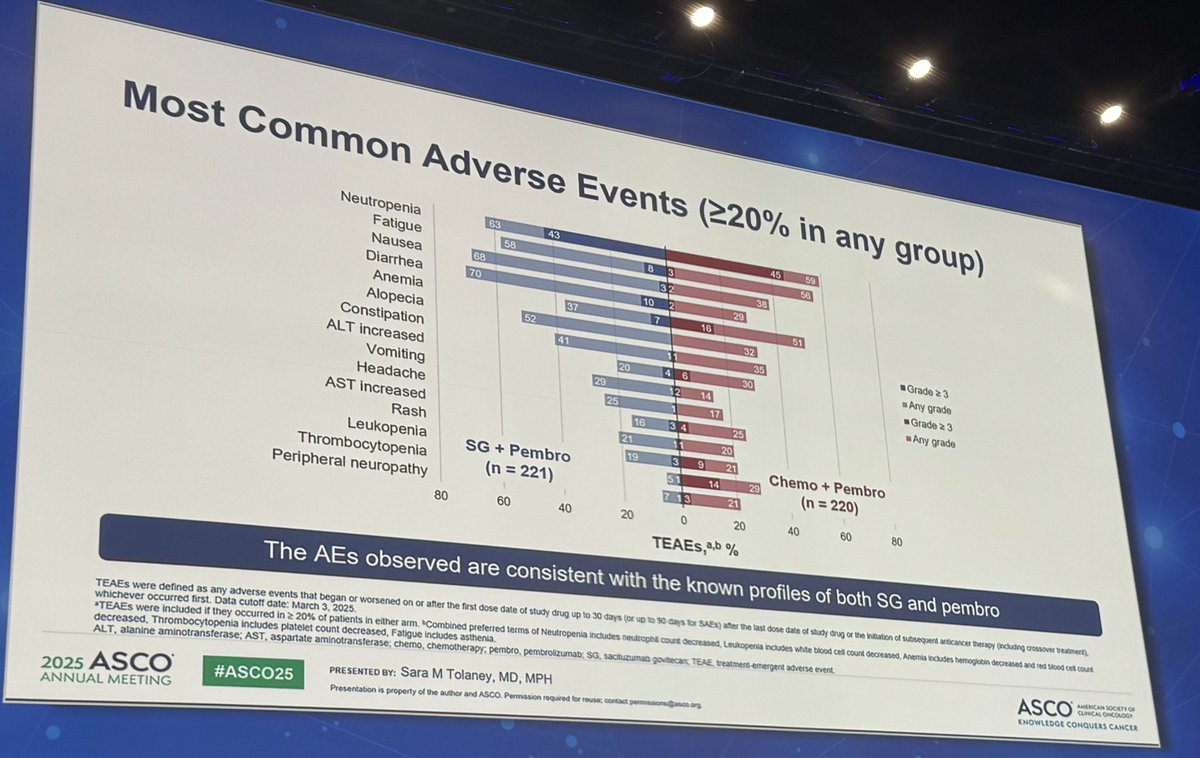
Most Common Adverse Events (≥20% in any group)
Neutropenia
63
43
45
59
Fatigue
58
8
3
56
Nausea
68
3
38
Diarrhea
70
10
2
29
Anemia
37
7
16
51
Alopecia
52
32
Constipation
41
35
Grade ≥ 3
ALT increased
20
4
6
30
Any grade
Vomiting
29
12
14
Grade 2 3
Headache
25
1
17
Any grade
AST increased
16
3
4
25
Rash
21
20
Leukopenia
19
3
9
21
SG + Pembro
Chemo + Pembro
Thrombocytopenia
51
14
29
(n = 221)
(n = 220)
Peripheral neuropathy
/
13
21
80
60
40
20
0
20
40
60
80
TEAEs, %
The AEs observed are consistent with the known profiles of both SG and pembro
TEAEs were defined as any adverse events that began or worsened on or after the first dose date of study drug up to 30 days (or up to 90 days for SAEs) after the last dose date of study drug or the initiation of subsequent anticancer therapy (including crossover treatment).
whichever occurred first. Data cutoff date: March 3, 2025.
TEAEs were included if they occurred in 2 20% of patients in either arm. Combined preferred terms of Neutropenia includes neutrophi count decreased, Leukopenia includes white blood cell count decreased, Anemia includes hemoglobin decreased and red blood cell count
decreased, Thrombocytopenia includes platelet count decreased, Fatigue includes asthenia.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; chemo, chemotherapy; pembro, pembrolizumab: SG, sacituzumao govtecan; TEAE, treatment emergent adverse event
2025 ASCO
#ASCO25
PRESENTED BY: Sara M Tolaney, MD, MPH
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@ason.org
KNOWLEDGE CONQUERS CANCER
ASCENT-04 / KEYNOTE-D19 (NCT05382286) is a Phase 3, international, open-label, randomized trial of the Trop-2 antibody-drug conjugate sacituzumab govitecan (SG; Trodelvy) plus pembrolizumab (Keytruda) versus investigator-choice chemotherapy (paclitaxel, nab-paclitaxel, or gemcitabine + carboplatin) plus pembrolizumab in patients with previously untreated, PD-L1-positive (CPS ≥ 10) locally advanced unresectable or metastatic triple-negative breast cancer. This PD-L1-positive group is the population for which chemo + pembrolizumab (KEYNOTE-355) has been the first-line standard of care. 443 patients were randomized 1:1 (221 SG + pembro vs 222 chemo + pembro); patients who progressed on the control arm could cross over to SG. The primary endpoint is progression-free survival by blinded independent central review (BICR). Primary PFS was presented at ASCO 2025 (LBA109, Sara Tolaney) with simultaneous publication in the New England Journal of Medicine; a biomarker-subgroup analysis (Abstract 1013) and a PFS2 / subsequent-therapy readout were presented at #ASCO26, and patient-reported outcomes were presented at ESMO 2025.
Study Design
Phase 3, international, open-label, randomized 1:1 (221 SG + pembro vs 222 chemo + pembro). SG 10 mg/kg IV days 1 & 8 of 21-day cycles + pembrolizumab 200 mg day 1; control = investigator-choice chemo + pembrolizumab (max 35 cycles). Crossover to 2L SG allowed after BICR-verified progression. Sponsors: Gilead Sciences / Merck.
Population
N=443 with previously untreated locally advanced or metastatic TNBC, PD-L1-positive (CPS ≥ 10) by 22C3. Up to 35% de novo mTNBC; prior anti-PD-(L)1 in the curative setting allowed if ≥ 6 months earlier.
First-line SG + pembrolizumab produced a statistically significant and clinically meaningful improvement in PFS by BICR: median 11.2 months vs 7.8 months with chemo + pembrolizumab, HR 0.65 (95% CI 0.51-0.84), P < 0.001 — a 35% reduction in the risk of progression or death. The 12-month PFS rate was 48% vs 33%. Responses were both more frequent and more durable with SG + pembro: ORR 60% vs 53% (complete response 13% vs 8%), with median DOR 16.5 vs 9.2 months.
At the primary analysis, overall survival was immature (~26% maturity) and not yet reported as a formal comparison, with interpretation confounded by extensive crossover — 96 of the 222 control-arm patients (81% of those who went on to subsequent therapy) crossed over to receive SG (ASCENT-04 PFS2, ASCO 2026 Abstract 1001). On safety, grade ≥ 3 treatment-related adverse events were comparable between arms (71% vs 70%), and fatal treatment-emergent events were equal (3% vs 3%). The toxicity profiles differed by regimen: SG + pembro carried more grade 3 neutropenia (43%) and diarrhea (10%), while chemo + pembro carried more neutropenia (45%), anemia (16%), and thrombocytopenia (14%). Critically, treatment discontinuation due to adverse events was markedly lower with SG + pembro (12% vs 31%), as were dose reductions (35% vs 44%).
The ASCO 2026 biomarker analysis (Tolaney, Abstract 1013) showed the PFS benefit of SG + pembrolizumab was maintained across every prespecified subgroup. By Trop-2 H-score quartile, median PFS favored SG + pembro in all four quartiles (Q1 HR 0.81, Q2 0.73, Q3 0.46, Q4 0.57; ITT 11.2 vs 7.8 mo, HR 0.65). The benefit held regardless of tumor BRCA status (tBRCA wild-type HR 0.67; mutant 0.88) and HER2-IHC0 vs HER2-low status — supporting the regimen without further biomarker selection. A separate PFS2 readout (Kalinsky) found median PFS2 was not reached with SG + pembro vs 21.0 months with chemo + pembro (stratified HR 0.67, 95% CI 0.48-0.95), with the benefit persisting despite the high control-arm crossover to SG and longer time to first and second subsequent therapies.
ASCENT-04 establishes first-line SG + pembrolizumab as an effective new option for PD-L1-positive mTNBC, the setting where chemo + pembrolizumab (KEYNOTE-355) has been standard. The improvement in PFS (11.2 vs 7.8 mo), the higher and more durable response rates (DOR 16.5 vs 9.2 mo), and the consistent benefit across Trop-2, tBRCA, and HER2 subgroups argue for moving SG into the first line for this population, while the lower discontinuation rate (12% vs 31%) points to a more manageable regimen. Open questions KOLs are watching: overall survival remains immature and is confounded by extensive control-arm crossover to SG (81% of those subsequently treated) — so PFS2 (NR vs 21.0 mo) is being used as a durable-benefit surrogate; the 1L indication is now FDA approved (June 24, 2026); and how this regimen sits alongside the PD-(L)1-ineligible ASCENT-03 monotherapy data and the other 1L Trop-2 ADC datopotamab deruxtecan.
ASCENT-04/KEYNOTE-D19 is a Phase 3 randomized trial comparing sacituzumab govitecan (Trodelvy) plus pembrolizumab (Keytruda) with pembrolizumab plus chemotherapy in first-line PD-L1-positive metastatic triple-negative breast cancer.
What were the ASCENT-04 results?
The combination improved median progression-free survival to 11.2 versus 7.8 months, an approximately 35% reduction in the risk of progression or death; results were published in the New England Journal of Medicine.
Is the Trodelvy plus Keytruda combination FDA approved?
Yes. In June 24, 2026 the FDA approved sacituzumab govitecan (Trodelvy) plus pembrolizumab (Keytruda) for first-line PD-L1-positive (CPS>=10) metastatic triple-negative breast cancer, based on ASCENT-04.
What is the approved regimen?
Sacituzumab govitecan (Trodelvy, Gilead), a Trop-2 antibody-drug conjugate, combined with pembrolizumab (Keytruda, Merck), an anti-PD-1 antibody.
Who sponsored ASCENT-04 and what is its identifier?
ASCENT-04/KEYNOTE-D19 was sponsored by Gilead Sciences in collaboration with Merck; its ClinicalTrials.gov identifier is NCT05382286.