Phase 3 AcceleRET-Lung: first-line pralsetinib (GAVRETO) vs platinum-based standard-of-care chemotherapy (± IO) in RET fusion-positive advanced or metastatic NSCLC. Presented at ASCO 2026 (Abstract 8504) by Sanjay Popat, the trial delivered Phase 3 confirmation of selective RET inhibition in the 1L setting.
2026ASCO
ANNUAL MEETING
---
AcceleRET-Lung: Open-Label, Randomized, Phase 3 Trial
of Pralsetinib in 1L RET Fusion-Positive mNSCLC
Pralsetinib
Primary endpoint:
RET fusion-positive mNSCLC
PFS by investigator assessment according to
ECOG PS 0 or 1
RECIST v1.1
No prior systemic treatment
Patients with CNS metastases were
Optional crossover
Secondary endpoints:
R 1:1
upon PD
permitted if they were asymptomatic and
Overall response rate: CR or PR, duration of
on a stable dose of corticosteroids
response
Planned enrollment: N=226
Investigator's choice of
Overall survival, clinical benefit rate, disease
platinum-based chemotherapy
control rate, safety/tolerability
(SOC)ᵃ
Stratification factors
Statistical assumptions
History of brain metastasis (yes VS no)
133 PFS events targeted for 90% power to detect an HR of 0.57
ECOG PS (0 vs 1)
Intended use of pembrolizumab (yes VS no)
corresponding to target median PFS:
Pralsetinib: 12.3 months
SOC: 7.0 months
"In patients with non-squamous histology, SOC regimens could include carboplatin/cisplatin + pemetrexed * pembrolizumab. In patients with squamous histology, SOC regimens could include carboplatin/cisplatin
gemcitabine, or pembrolizumab + carboplatin + paclitaxel/nab-paclitaxel.
1L, first-line; CNS, central nervous system; CR, complete response; ECOG PS, Eastern Cooperative Oncology Group Performance Status; HR, hazard ratio; mNSCLC, metastatic non-small cell lung cancer; PD,
progressive disease; PFS, progression-free survival; PR, partial response; RECIST, Response Evaluation Criteria in Solid Tumors; SOC, standard of care.
2026 ASCO
#ASCO26
PRESENTED BY: Dr. Sanjay Popat
ASCO
AMERICAN SOCIETY or
CUNICAL ONCOLOGY
4
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
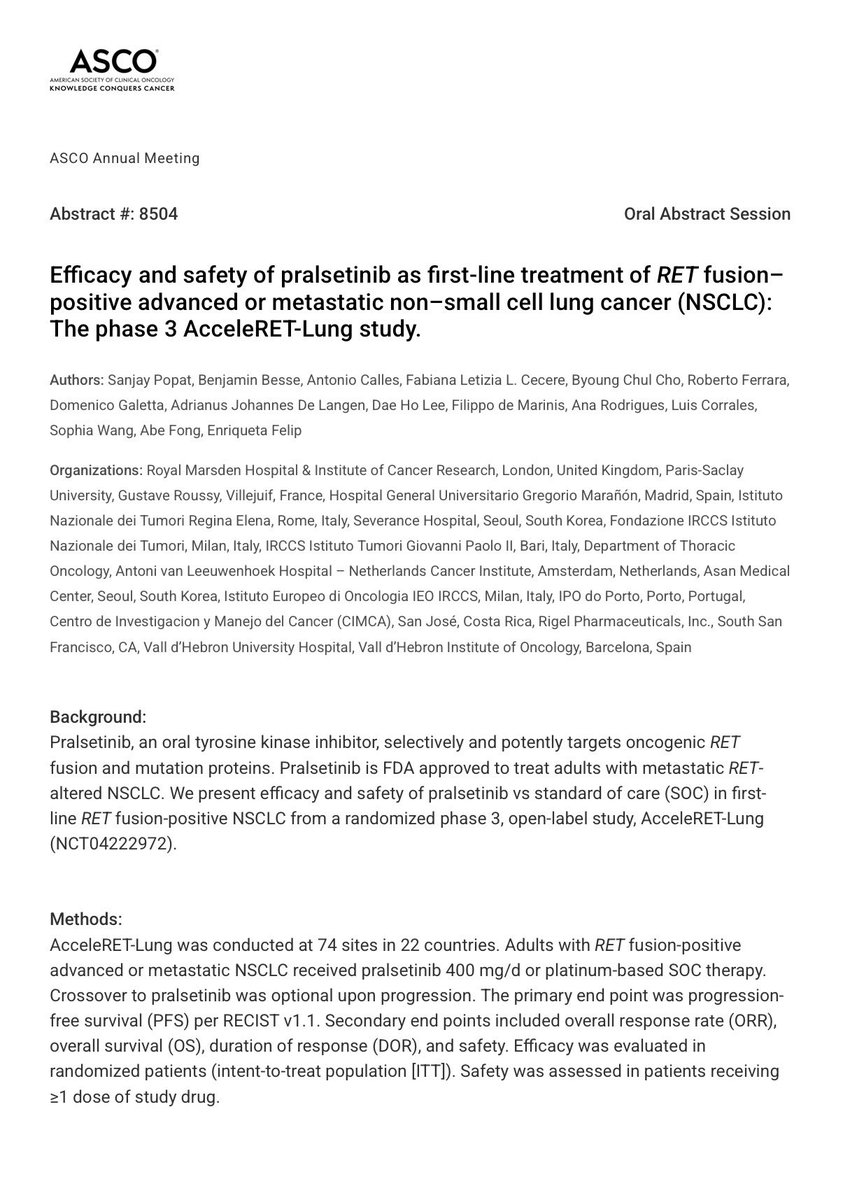
Pralsetinib Treatment Significantly Reduced the Risk
of Progression or Death vs SOC (Primary Endpoint)
100
Pralsetinib
SOC
Investigator assessment
90
(n=110)
(n=113)
18.7
9.0
80
Median PFS, months (95% CI)
(11.1, 25.2)
(7.1, 11.5)
Progression-Free Survival (%)
70
HR (95% CI)
0.59 (0.42, 0.84)
60
Log-rank P value
0.0027
Median duration of follow-up,
20.5
16.0
50
months (95% CI)
(17.5, 23.2)
(13.7, 20.9)
40
30
20
Pralsetinib
SOC
10
+
Censored
0
0
6
12
18
24
30
36
42
48
Number at risk
Time (Months)
Pralsetinib
110
75
51
36
22
16
7
1
SOC
113
64
31
18
8
4
1
Median PFS among intended use of pembrolizumab patients
Pralsetinib (n=73): 18.7 (8.6, 30.2) months SOC (n=74): 7.2 (5.1, 10.9) months (HR: 0.51)
HR, hazard ratio; PFS, progression-free survival; SOC, standard of care.
2026 ASCO
#ASCO26
PRE SENTED BY: Dr. Sanjay Popat
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
7
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
---
Pralsetinib Yielded Significantly Higher Response
Rates and More Durable Responses Than SOC
Overall Response Rate
100
Duration of Response
65.5%
90
Investigator
Pralsetinib
SOC
assessment
(95% Cl: 55.79, 74.26)
(n=72)
(n=47)
80
Median DOR,
20.6
9.7
41.6%
70
months (95% CI)
(17.2, 31.8)
(7.6, 15.9)
23.9
HR (95% CI)
0.48 (0.28, 0.80)
(95% Cl: 32.40, 51.24)
60
Log-rank P value
0.0043
50
40
30
20
Pralsetinib
10
SOC
Pralsetinib (n=110)
SOC (n=113)
Censored
0
Difference in ORR (95% CI)
23.9 (10.3, 37.5)
0
6
12
18
24
30
36
42
Odds ratio (95% CI)
2.81 (1.61, 4.93)
Number at risk
Time (Months)
Pralsetinib
72
54
40
25
14
9
4
1
P value (Cochran-Mantel-Haenszel)
0.0002
SOC
47
30
17
10
4
2
No significant difference in median (95% CI) OS between pralsetinib (NR [29.6 months, NR]) and SOC (39.8 months [39.8 months, NR])
- OS data was immature with >70% patients in each arm alive at end of study (HR [95% CI]: 1.09 [0.65, 1.85]; P=0.742)ᵃ
- 38 (34%) SOC patients crossed over to pralsetinib arm
"There were 33 (30%) deaths in the praisetinib arm and 27 (24%) deaths in the SOC arm.
DOR, duration of response; HR, hazard ratio; ORR, overall response rate; OS, overall survival; NR, not reached; SOC, standard of care.
2026 ASCO
#ASCO26
PRESENTED BY: Dr. Sanjay Popat
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
9
ANNUAL MEETING
Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco org.
KNOWLEDGE CONQUERS CANCER
ASCO 2026
ORAL ABSTRACT
AcceleRET-Lung
1L RET+ NSCLC
RET
Phase 3 study of pralsetinib VS platinum-
based standard of care (SOC)
@DrRishabhOnco)
Pralsetinib
Untreated
223
advanced or
Pralsetinib
SOC
patients
metastatic
400 mg/d
vs
randomized
RET fusion+
(n=113)
NSCLC
(n=110)
PRIMARY ENDPOINT: PFS
18.7
9.0
HR 0.59
VS
P=0.003
months
months
Pralsetinib
SOC
PFS DOUBLED
ORR
DOR
os
(overall response rate)
(duration of response)
(overall survival)
66%
VS
42%
20.6
VS
9.7
NR
vs
39.8
months
months
P<0.001
P=0.004
Not significant
HIGHER INFECTION RISK
Any infection
Infection-related
deaths
with pralsetinib
71% VS 52%
7.4% VS 0%
.
Pralsetinib doubled PFS in
RET+ NSCLC,
but infections require monitoring.
ASCO
AMERICAN SOCIETY OF CLINICAL ONCOLOGY
KNOWLEDGE CONQUERS CANCER
ASCO Annual Meeting
Abstract #: 8504
Oral Abstract Session
Efficacy and safety of pralsetinib as first-line treatment of RET fusion-
positive advanced or metastatic non-small cell lung cancer (NSCLC):
The phase 3 AcceleRET-Lung study.
Authors: Sanjay Popat, Benjamin Besse, Antonio Calles, Fabiana Letizia L. Cecere, Byoung Chul Cho, Roberto Ferrara,
Domenico Galetta, Adrianus Johannes De Langen, Dae Ho Lee, Filippo de Marinis, Ana Rodrigues, Luis Corrales,
Sophia Wang, Abe Fong, Enriqueta Felip
Organizations: Royal Marsden Hospital & Institute of Cancer Research, London, United Kingdom, Paris-Saclay
University, Gustave Roussy, Villejuif, France, Hospital General Universitario Gregorio Maranon, Madrid, Spain, Istituto
Nazionale dei Tumori Regina Elena, Rome, Italy, Severance Hospital, Seoul, South Korea, Fondazione IRCCS Istituto
Nazionale dei Tumori, Milan, Italy, IRCCS Istituto Tumori Giovanni Paolo II, Bari, Italy, Department of Thoracic
Oncology, Antoni van Leeuwenhoek Hospital - Netherlands Cancer Institute, Amsterdam, Netherlands, Asan Medical
Center, Seoul, South Korea, Istituto Europeo di Oncologia IEO IRCCS, Milan, Italy, IPO do Porto, Porto, Portugal,
Centro de Investigacion y Manejo del Cancer (CIMCA), San Jose, Costa Rica, Rigel Pharmaceuticals, Inc., South San
Francisco, CA, Vall d'Hebron University Hospital, Vall d'Hebron Institute of Oncology, Barcelona, Spain
Background:
Pralsetinib, an oral tyrosine kinase inhibitor, selectively and potently targets oncogenic RET
fusion and mutation proteins. Pralsetinib is FDA approved to treat adults with metastatic RET-
altered NSCLC. We present efficacy and safety of pralsetinib VS standard of care (SOC) in first-
line RET fusion-positive NSCLC from a randomized phase 3, open-label study, AcceleRET-Lung
(NCT04222972).
Methods:
AcceleRET-Lung was conducted at 74 sites in 22 countries. Adults with RET fusion-positive
advanced or metastatic NSCLC received pralsetinib 400 mg/d or platinum-based SOC therapy.
Crossover to pralsetinib was optional upon progression. The primary end point was progression-
free survival (PFS) per RECIST v1.1. Secondary end points included overall response rate (ORR),
overall survival (OS), duration of response (DOR), and safety. Efficacy was evaluated in
randomized patients (intent-to-treat population [ITT]). Safety was assessed in patients receiving
≥1 dose of study drug.
---
Results:
223 ITT patients were randomized to pralsetinib (n=110) or SOC (n=113). Pralsetinib and SOC
groups had similar baseline characteristics (median age: 62 and 63 y, respectively; female: 48%
and 57%; median lesions: both 4; brain metastases: 15% and 16%). The study was terminated
early per sponsor decision on January 27, 2025. ITT patients in the pralsetinib group had
significantly greater median PFS VS SOC (18.7 VS 9.0 mo; P=0.003), ORR (65.5% VS 41.6%;
P<0.001), and median DOR (20.6 VS 9.7 mo; P=0.004; Table). Safety was generally consistent
with the known pralsetinib profile except for a higher rate of infection in the pralsetinib group VS
SOC (71.3% VS 51.9%), including pneumonia (19.4% VS 5.8%), urinary tract infections (17.6% VS
7.7%), and opportunistic infections (9.3% VS 1.0%). There were 32 (30.0%) and 26 (25.0%) deaths
in the pralsetinib and SOC groups, respectively, with 8 (7.4%) and 0 due to infection. Common
grade ≥3 TRAEs in the pralsetinib VS SOC groups were hypertension (11.1% VS 0), neutropenia
(10.2% VS 8.7%), anemia (8.3% VS 10.6%), and decreased neutrophil count (7.4% VS 4.8%).
Conclusions:
In a Phase 3 study, pralsetinib met the primary PFS end point and had a significantly greater and
more durable ORR VS SOC, confirming the clinical utility of pralsetinib in RET fusion-positive
NSCLC. Monitoring for infections with pralsetinib is warranted.
Efficacy outcomes.
SOC
Pralsetinib (n=110)
Stratified hazard ratio/odds ratio (95% CI)
P Value
(n=113)
20.5
16.0
Duration of follow-up, mo, median (range)
(0,49.8)
(0,42.3)
18.7
9.0
0.59
PFS, mo, median (95% CI)
0.003
(11.1.25.2)
(7.1.11.5)
(0.42.0.84)
65.5
41.6
2.81
ORR, % (95% CI)
<0.001
(55.8,74.3)
(32.4,51.2)
(1.61,4.93)
39.8
1.09
os, mo, median (95% CI)
NR (29.6, NR)
0.742
(39.8, NR)
(0.65, 1.85)
20.6
9.7
0.48
DOR, mo, median (95% CI)
0.004
(17.2,31.8)
(7.6,15.9)
(0.28,0.80)
Research Funding:
Rigel Pharmaceuticals, Inc.
ASCO26
LUNG
CANCER
OncoAlert
360°
TOP TEN BY ONCOALERT
Oncology
For Collegues
By Colleagues
LBA4
HARMONI-6: IVONESCIMAB + CHEMO VS TISLELIZUMAB + CHEMO IN PREVIOUSLY UNTREATED
ADVANCED SQUAMOUS NSCLC - OS RESULTS (PHASE 3)
LBA3
LIBRETTO-432: ADJUVANT SELPERCATINIB IN STAGE IB-IIIA RET FUSION-POSITIVE NSCLC - EFS
PRIMARY RESULTS (PHASE 3)
8506
OPTITROP-LUNGO5: SACITUZUMAB TIRUMOTECAN + PEMBROLIZUMAB vs PEMBROLIZUMAB
AS 1L TREATMENT FOR PD-L1-POSITIVE ADVANCED NSCLC (RANDOMIZED PHASE 3)
8515
TRITON: TREMELIMUMAB + DURVALUMAB + CHEMO vs PEMBROLIZUMAB + CHEMO IN 1L NSQ
MNSCLC WITH STK11, KEAP1, AND/OR KRAS MUTATIONS (PHASE 2B INTERIM ANALYSIS)
LBA8500
WU-KONG28: SUNVOZERTINIB MONOTHERAPY vs PLATINUM-BASED CHEMO AS 1L TREATMENT
WWW.ONCOALERT360.COM
FOR ADVANCED NSCLC WITH EGFR EXON20INS (MULTINATIONAL PHASE 3)
8002
LORIN: NEOADJUVANT LORLATINIB IN STAGE III NSCLC HARBORING ALK FUSION (PHASE 2
MULTICENTER)
8502
CROWN: LORLATINIB vs CRIZOTINIB AS 1L TREATMENT FOR ADVANCED ALK+ NSCLC - 7-YEAR
UPDATE (PHASE 3)
8503
ALKOVE-1: NELADALKIB EFFICACY AND SAFETY IN PATIENTS WITH ADVANCED ALK+ NSCLC
LBA1510
LOW-DOSE PEMBROLIZUMAB WITH CHEMOTHERAPY IN ADVANCED NSCLC
8519
SILEVERTINIB (BDTX-1535) IN TREATMENT-NAİVE NSCLC WITH NON-CLASSICAL EGFR MUTATIONS
(PHASE 2)
ACCELERET-LUNG: PRALSETINIB AS 1L TREATMENT OF RET FUSION-POSITIVE ADVANCED/METASTATIC
8504
NSCLC (PHASE 3)
LBA8005
CONCURRENT THORACIC RADIOTHERAPY, PLATINUM/ETOPOSIDE CHEMOTHERAPY, AND DURVALUMAB
IMMUNOTHERAPY IN EXTENSIVE-STAGE SCLC (PHASE III)
Leads
Senior Faculty
Participating AF
Dr Horinouchi
Dr. özkerim
Dr Morgan
Dr. Liu
Dr Peters
Dr. Lovly
Dr. Lopes
Dr. Aggarwal
Dr. Reck
Dr. Mirallas
Med Onc
Med Onc
Clin Onc
Med Onc
Med Onc
Med Onc
Med Onc
Med Onc
Med Onc
Med Onc
ASCO
AMERICAN SOCIETY OF CLINICAL ONCOLOGY
KNOWLEDGE CONQUERS CANCER
Abstract #: 8504
Efficacy and safety of pralsetinib as first-line treatment of RET fusion-positive advanced or
metastatic non-small cell lung cancer (NSCLC): The phase 3 AcceleRET-Lung study.
Authors: Sanjay Popat, Benjamin Besse, Antonio Calles, Fabiana Letizia L. Cecere, Byoung Chul Cho,
Roberto Ferrara, Domenico Galetta, Adrianus Johannes De Langen, Dae Ho Lee, Filippo de Marinis, Ana
Rodrigues, Luis Corrales, Sophia Wang, Abe Fong, Enriqueta Felip
AcceleRET-Lung (NCT04222972) is the Phase 3 randomized trial that took pralsetinib (GAVRETO, Rigel Pharmaceuticals) — a selective oral RET kinase inhibitor — head-to-head against platinum-based standard-of-care chemotherapy (with optional IO) as first-line treatment of advanced or metastatic RET fusion-positive NSCLC. Presented at ASCO 2026 in an oral session (Abstract 8504, May 29, 2026) by Prof. Sanjay Popat of the Royal Marsden, AcceleRET-Lung met its primary PFS endpoint with a near-doubling of median progression-free survival (18.7 vs 9.0 months, p=0.003), a markedly higher response rate, and a more durable response — finally giving the field Phase 3 confirmation of a selective RET inhibitor in 1L RET+ NSCLC.
Population
Treatment-naïve adults with advanced or metastatic RET fusion-positive NSCLC (centrally confirmed). Asymptomatic CNS metastases allowed.
Intervention
Pralsetinib 400 mg PO once daily vs investigator's choice platinum-based chemotherapy ± pembrolizumab (non-squamous: pemetrexed; eligible squamous: gemcitabine), with optional crossover from SOC to pralsetinib at radiographic progression.
Primary Endpoint
Progression-free survival by blinded independent central review (BICR) per RECIST 1.1.
Key Secondary
Overall response rate (ORR), duration of response (DOR), overall survival (OS, immature), safety/tolerability, and intracranial activity in CNS-metastasis subgroup.
Efficacy & Safety
Reported Results
Progression-Free Survival (Primary Endpoint)
First-line pralsetinib produced a more than 2× improvement in median progression-free survival vs platinum-based SOC: mPFS 18.7 vs 9.0 months (p=0.003) in treatment-naïve RET fusion-positive advanced NSCLC. This is the first Phase 3 confirmation that selective RET inhibition outperforms chemotherapy in the 1L setting, validating earlier accelerated-approval data and establishing pralsetinib as a 1L option for this oncogene-defined subgroup.
Pralsetinib delivered a substantially higher and far more durable response than chemotherapy. ORR 65.5% vs 41.6% (pralsetinib vs SOC) and median DOR 20.6 vs 9.7 months. KOLs flagged the magnitude of DOR improvement — more than doubling — as the most clinically meaningful signal beyond the headline PFS result.
Pralsetinib was generally well-tolerated with a profile consistent with prior single-arm studies. KOLs highlighted a notable infection signal: 30 deaths (30.0%) in the pralsetinib arm vs 26 (25.0%) in SOC, with 8 (7.4%) due to infection on pralsetinib vs 0 on SOC. The Rigel presentation suggested increased monitoring is sufficient to manage severe infection risk in practice. Overall survival data remained immature at the data cutoff.
STATUSFDA Accelerated Approval (Sept 2020) · Phase 3 Confirmation Now Available
Pralsetinib (GAVRETO) received FDA accelerated approval in September 2020 for metastatic RET fusion-positive NSCLC based on the Phase 1/2 ARROW study. With AcceleRET-Lung now providing Phase 3 confirmation of efficacy versus platinum-based standard of care, the regulatory pathway to a full / regular approval in 1L RET+ NSCLC is now anticipated. Pralsetinib is currently marketed in the US by Rigel Pharmaceuticals, which reacquired the asset following Roche/Genentech's commercial wind-down in 2023.