FDA Approved · Apr 4, 2024Triple-class-exposed R/R MyelomaPhase 3 · NCT03651128BMS / 2seventy bio
KarMMa-3 is a Phase 3 trial of idecabtagene vicleucel (ide-cel, Abecma; BMS / 2seventy bio) versus standard regimens in triple-class-exposed relapsed/refractory multiple myeloma (2-4 prior lines). It significantly improved progression-free survival (13.3 mo primary / 13.8 mo updated vs 4.4; HR 0.49) and response (ORR 71% vs 42%); overall survival was confounded by 56% crossover (ITT HR 1.01). FDA approved April 4, 2024.
FDA APPROVED April 4, 2024 - relapsed/refractory multiple myeloma (≥2 prior lines)
The FDA approved idecabtagene vicleucel (ide-cel, Abecma; Bristol Myers Squibb / 2seventy bio) for triple-class-exposed relapsed/refractory multiple myeloma after two or more prior lines, based on KarMMa-3. The trial met its PFS primary endpoint; overall survival interpretation is confounded by extensive crossover.
Design: ide-cel vs standard regimens (investigator's choice of 5), triple-class-exposed R/R MM, 2-4 prior lines (N=386).
PFS: 13.3 mo (NEJM primary) / 13.8 mo (ASH 2023 update) vs 4.4 mo - HR 0.49, P<0.0001 (51% risk reduction).
Response: ORR 71% vs 42%; CR 44% vs 5%; MRD-negative CR 35% vs 2% (ASH 2023).
Overall survival: ITT 41.4 vs 37.9 mo, HR 1.01 - confounded by 56% crossover; crossover-adjusted HR 0.72. No clear unadjusted OS benefit (actively debated).
Regulatory: FDA approved April 4, 2024 (≥2 prior lines, triple-class exposed).
[Slide 1] Significant benefit with ide-cel at final PFS analysis (ITT population). Median PFS: ide-cel 13.8 months vs standard regimens 4.4 months. Hazard ratio 0.49 (95% CI 0.38-0.63). 18-month PFS rate 41% vs 19%. Patients at risk: ide-cel 254, standard regimens 132. Rodriguez-Otero P, et al. ASH 2023 [Abstract 1028].
[Slide 2] Deep and durable responses with ide-cel. Difference in ORR 29%, OR 3.36 (95% CI 2.17-5.22). ORR 71% (95% CI 66-77) vs 42% (95% CI 34-51). CR rate 44% (38-50) vs 5% (2-9). MRD-negative CR rate 57/163 (35%) vs 1/54 (2%). Median DOR 16.6 months (12.1-19.6) vs 9.7 (5.5-16.1). Median PFS2 23.5 vs 16.7 months, HR 0.79 (0.60-1.04).
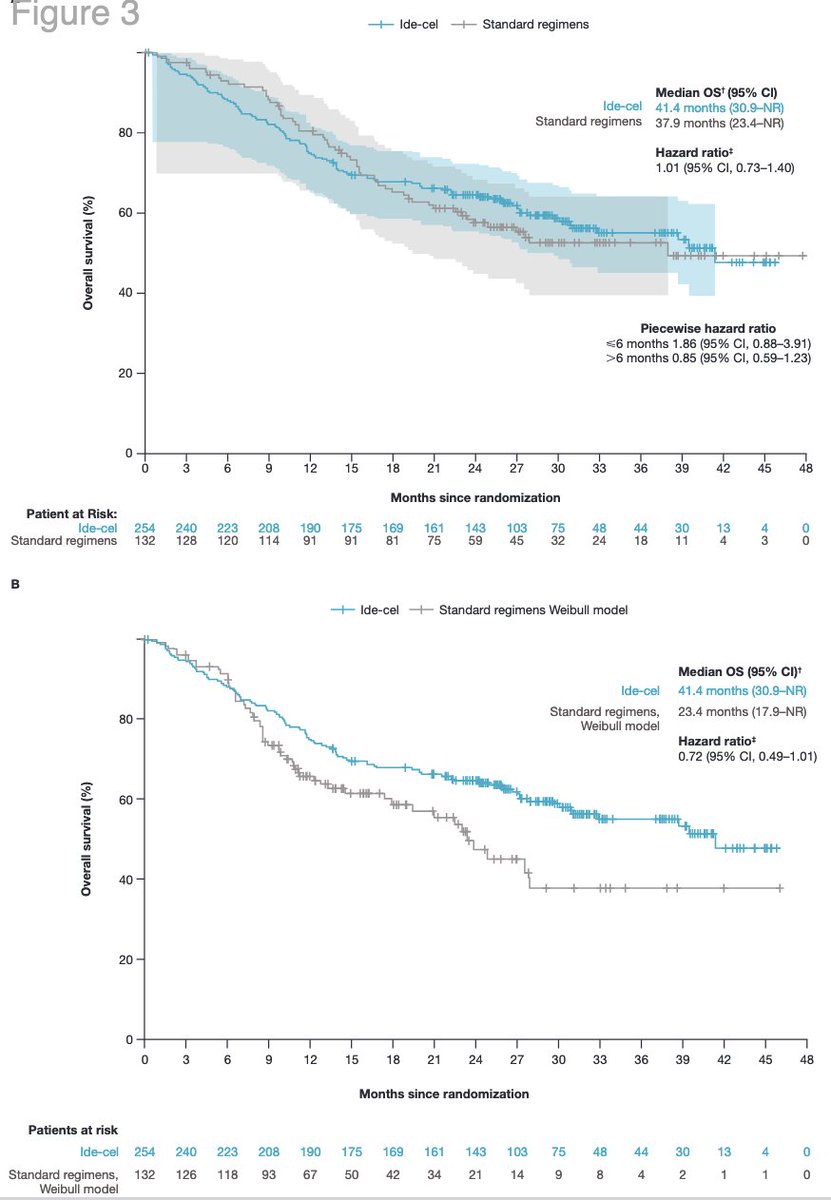
[Slide 3] OS analysis confounded by substantial crossover. ITT population: median OS 41.4 (30.9-NR) vs 37.9 (23.4-NR) months, HR 1.01 (95% CI 0.73-1.40). Sensitivity analysis adjusted for crossover (two-stage Weibull): 41.4 vs 23.4 (17.9-NR) months, HR 0.72 (95% CI 0.49-1.01). Information fraction 74% (164/222 events).
[Slide 4] Patients who never received ide-cel drive imbalance in early OS events. Patients who died <=6 months from randomization: ide-cel 30 (12%) vs standard 9 (7%). Of ide-cel early deaths, 17 (7%) did NOT receive study treatment vs 0 in the standard arm. Primary cause of death: AEs 8 (3%) vs 3 (2%); myeloma progression 18 (7%) vs 6 (5%). Early-death subgroup enriched for R-ISS III, high-risk cytogenetics, EMP, and high tumor burden.
[Slide 1] Figure 2. Progression-free survival. Median PFS ide-cel 13.8 vs standard regimens 4.4 months, HR 0.49 (0.38-0.63); 18-month PFS 41% vs 19%. By prior lines (ide-cel): 2 prior lines 16.2 months (13.3-20.9), 3 lines 13.6 (10.2-17.7), 4 lines 11.2 (7.4-15.2); standard regimens 4.8 / 3.4 / 4.8 months.
[Slide 2] Figure 3. Overall survival. ITT median OS 41.4 vs 37.9 months, HR 1.01 (0.73-1.40). Piecewise HR <=6 months 1.86 (0.88-3.91); >6 months 0.85 (0.59-1.23). Crossover-adjusted Weibull model: 41.4 vs 23.4 months, HR 0.72 (0.49-1.01).
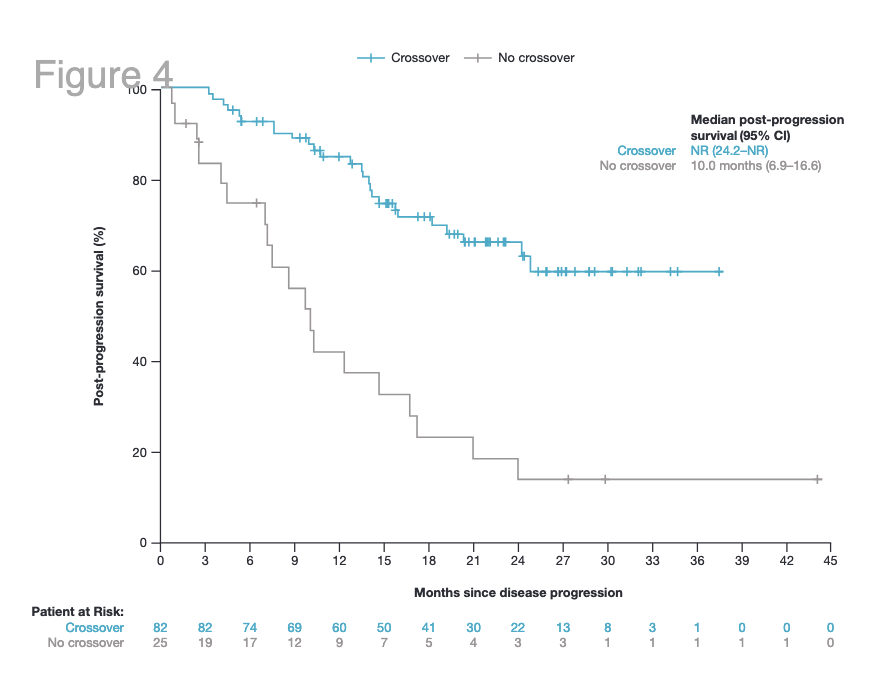
[Slide 3] Figure 4. Post-progression survival. Crossover NR (24.2-NR) vs no crossover 10.0 months (6.9-16.6).
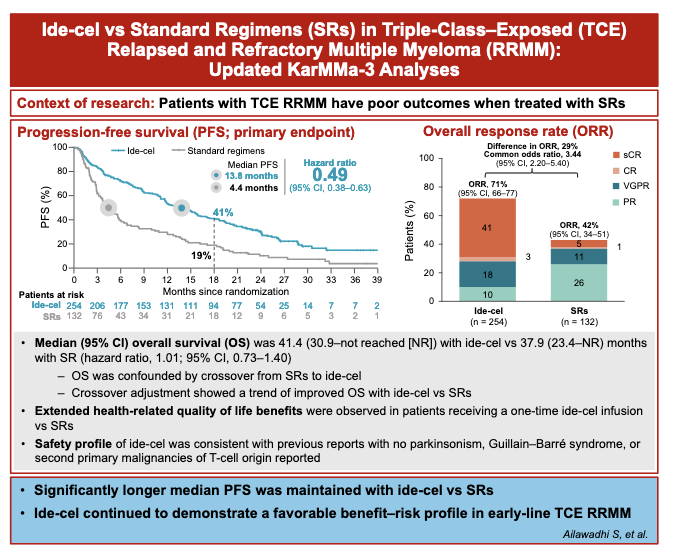
[Slide 4] Visual abstract (Ailawadhi S, et al.): Ide-cel vs Standard Regimens in Triple-Class-Exposed RRMM - Updated KarMMa-3 Analyses. PFS 13.8 vs 4.4 months, HR 0.49. ORR 71% vs 42%, common OR 3.44. Median OS 41.4 vs 37.9 months, HR 1.01 - confounded by crossover from standard regimens to ide-cel; crossover adjustment showed a trend of improved OS. Extended HRQoL benefits with a one-time ide-cel infusion. Safety consistent with prior reports - no parkinsonism, Guillain-Barre syndrome, or second primary malignancies of T-cell origin.
[Slide 1] Clinical implications and insights from patient-reported outcome (PRO) data in KarMMa-3 (Lancet Haematology, March 2024; commentary by Rajshekhar Chakraborty on Delforge et al). Although KarMMa-3 met its primary endpoint (PFS), there was no overall survival benefit at median follow-up of ~31 months given crossover. PRO data significantly and meaningfully improved across prespecified EORTC QLQ-C30 domains (global QoL, physical functioning, fatigue, pain). Ide-cel led to earlier time to improvement and delayed time to deterioration. PROs measured at day 1 of infusion, month 1, then each QoL-assessment phase.
[Slide 2] (continued) A systematic review showed that just five (3%) of 149 oncology clinical trials assessed quality of life until death. In a heavily pretreated population with median overall survival of ~3 years, comprehensive PRO reporting provides insight into patient experience and treatment decision-making. Rajshekhar Chakraborty, Columbia University Irving Medical Center, New York.
[Slide 1] Progression-free survival. Median PFS ide-cel 13.8 vs 4.4 months, HR 0.49 (0.38-0.63); 18-month PFS rate 41% vs 19%.
[Slide 2] Baseline characteristics. Median age 63 years (both arms). Previous autologous HSCT 84% vs 86%. R-ISS stage III 12% vs 11%. High tumor burden 28% vs 26%. High-risk cytogenetics 65% vs 62% (del(17p) 26% vs 32%; t(4;14) 17% vs 14%; 1q gain/amplification 49% vs 39%). Ultra-high-risk cytogenetics 26% vs 22%. Daratumumab-refractory 95% vs 93%. Triple-class-refractory 65% vs 67%.
[Slide 1] Changes in overall HRQoL from baseline (EORTC QLQ-C30 GHS/QoL and EQ-5D-5L VAS). Ide-cel showed significant and meaningful improvements vs standard regimens. Delforge M, et al. ASH 2023 [Abstract #96].
[Slide 2] Change in fatigue and pain from baseline (EORTC QLQ-C30). Ide-cel showed significant and meaningful improvements in fatigue and pain vs standard regimens.
[Slide 3] Between-group differences in all PRO domains from baseline to month 25. Overall LSM changes favored ide-cel for 18 of 21 domains, effect size (Hedges' g) 0.3 to 0.8; differences exceeded prespecified MID thresholds in 13 domains. GHS/QoL difference 7.49 (g 0.58); fatigue -7.60 (g -0.51); pain -6.64 (g -0.39).
[Slide 4] Time to confirmed deterioration, ide-cel vs standard regimens, all PRO domains. Significantly longer with ide-cel for EORTC QLQ-C30 emotional, cognitive, and social functioning, dyspnea, and constipation, and QLQ-MY20 side effects. In general, more domains favored ide-cel for time to improvement.
KarMMa-3 is a global, randomized, open-label Phase 3 trial of idecabtagene vicleucel (ide-cel, Abecma) versus standard regimens in patients with triple-class-exposed relapsed/refractory multiple myeloma after 2-4 prior lines. The primary endpoint, progression-free survival, was met (13.3 months NEJM primary / 13.8 months ASH 2023 update vs 4.4 months; HR 0.49), with higher response rates (ORR 71% vs 42%). Because the design permitted crossover (56% of standard-regimen patients received ide-cel on progression), overall survival is confounded: the ITT hazard ratio was 1.01 while a prespecified crossover-adjusted analysis showed a trend (HR 0.72). The therapy is FDA approved (April 4, 2024).
Median PFS was 13.3 months in the NEJM primary analysis and 13.8 months in the ASH 2023 updated analysis, versus 4.4 months with standard regimens (HR 0.49, P<0.0001) - a 51% reduction in the risk of progression or death. 18-month PFS rate 41% vs 19%.
Median PFS 13.3 (primary) / 13.8 (updated) vs 4.4 months · HR 0.49
Objective response rate was 71% with ide-cel versus 42% with standard regimens (OR 3.36). Complete response 44% vs 5%; MRD-negative CR 35% vs 2%; median duration of response 16.6 vs 9.7 months (ASH 2023).
In the ITT population, median OS was 41.4 vs 37.9 months with a hazard ratio of 1.01 (95% CI 0.73-1.40) - no unadjusted benefit. This is confounded: 56% of standard-regimen patients crossed over to ide-cel on progression. A prespecified crossover-adjusted (two-stage Weibull) analysis estimated 41.4 vs 23.4 months, HR 0.72 (0.49-1.01). A piecewise analysis showed early excess hazard (≤6 months HR 1.86) reversing after 6 months (HR 0.85). The early-death imbalance was driven largely by patients who never received the ide-cel infusion (17 of 30 early deaths). This is the central point of KOL debate.
Ide-cel carries CAR T-specific risks (cytokine release syndrome, neurotoxicity); the updated safety profile reported no parkinsonism, Guillain-Barre syndrome, or T-cell-origin second primary malignancies. Patient-reported outcomes (EORTC QLQ-C30, EQ-5D-5L) favored ide-cel in 18 of 21 domains, including global health status/QoL, fatigue, and pain (Delforge et al., ASH 2023). The OS confounding and early grade-5 events remain the basis for ongoing expert debate.
KarMMa-3 is a Phase 3 randomized trial comparing ide-cel (Abecma) against standard regimens in triple-class-exposed relapsed/refractory multiple myeloma after 2-4 prior lines.
What were the KarMMa-3 PFS results?
Median PFS was 13.3 months (NEJM primary) / 13.8 months (ASH 2023 update) versus 4.4 months (HR 0.49; P<0.0001); ORR was 71% versus 42%.
Did KarMMa-3 show an overall survival benefit?
No clear unadjusted benefit: ITT OS was 41.4 vs 37.9 months (HR 1.01), confounded by 56% crossover. A crossover-adjusted analysis showed a trend (HR 0.72). It remains actively debated.
Is ide-cel (Abecma) FDA approved based on KarMMa-3?
Yes. On April 4, 2024 the FDA approved ide-cel for R/R multiple myeloma after ≥2 prior lines including an IMiD, a proteasome inhibitor, and an anti-CD38 antibody.
Why is KarMMa-3 debated?
The clear PFS benefit contrasts with the lack of a clear unadjusted OS benefit (ITT HR 1.01, crossover-confounded) and an early excess of deaths in the ide-cel arm, largely among patients who never received the infusion.