Design — Phase 3; sacituzumab govitecan (Trodelvy, TROP2 ADC) vs docetaxel in 2L+ metastatic NSCLC post platinum + IO (NCT05089734). (ASCO 2024)
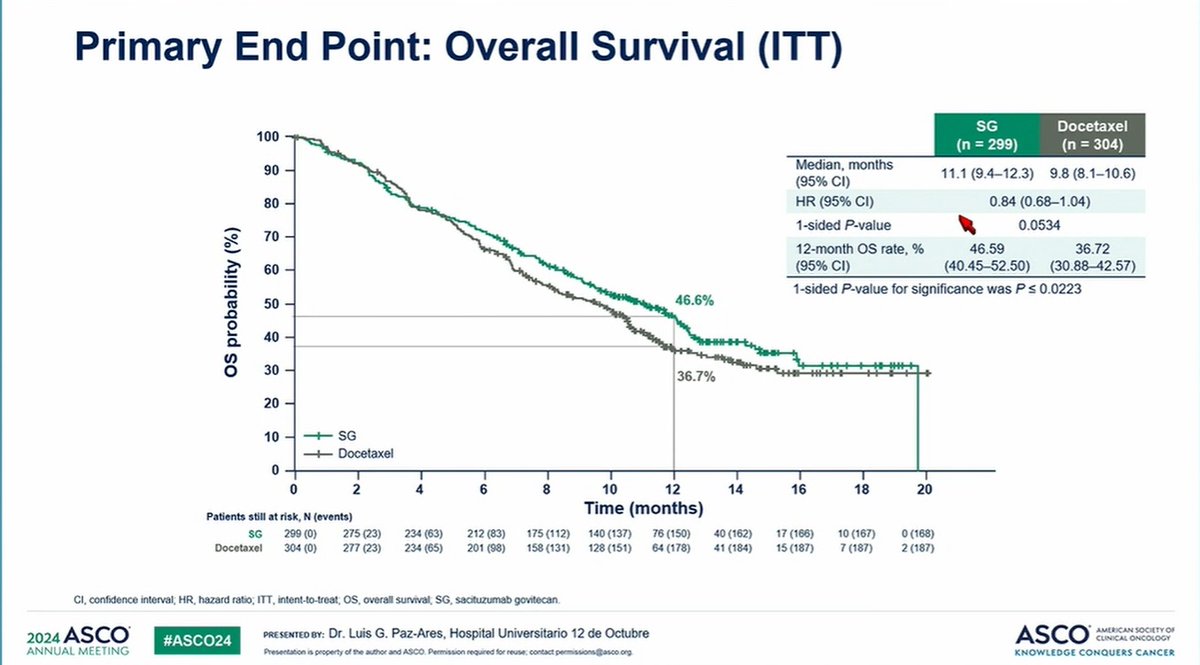
OS (primary — NOT met) — Median OS 11.1 vs 9.8 mo, HR 0.84 (95% CI 0.68-1.04; one-sided p=0.0534) — did not reach significance. (ASCO 2024, page data)
PFS — No significant PFS benefit: 4.1 vs 3.9 mo, HR 0.92 (not significant). (ASCO 2024)
Safety — Grade 3+ treatment-related AEs 66.6%; key toxicities neutropenia, diarrhea, fatigue. (page data)
Regulatory — NOT FDA approved in NSCLC. Trodelvy is approved in mTNBC, HR+/HER2- breast cancer, and urothelial cancer. (FDA.gov)
Sponsor / Drug — Gilead Sciences; sacituzumab govitecan (Trodelvy), a TROP2-directed antibody-drug conjugate. (Gilead)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 20, 2026.




















Top 10 by impressions - click to view on X
Such level of spin in the published conclusion!! @JCO_ASCO ❗️ We predicted it👇
Two new studies support the hypothesis that pts with EGFR mutated NSCLC are the best population for TROP-2 ADCs: EVOKE-01 (EGFR is in the ‘AGA’ subgroup in the forest plot) and ICARUS-LUNG....
$GILD's Trodelvy double whammy sees Evoke-01 underwhelm at #ASCO24 the day after Tropics-04 fails to confirm bladder cancer benefit. Via @ApexOnco...
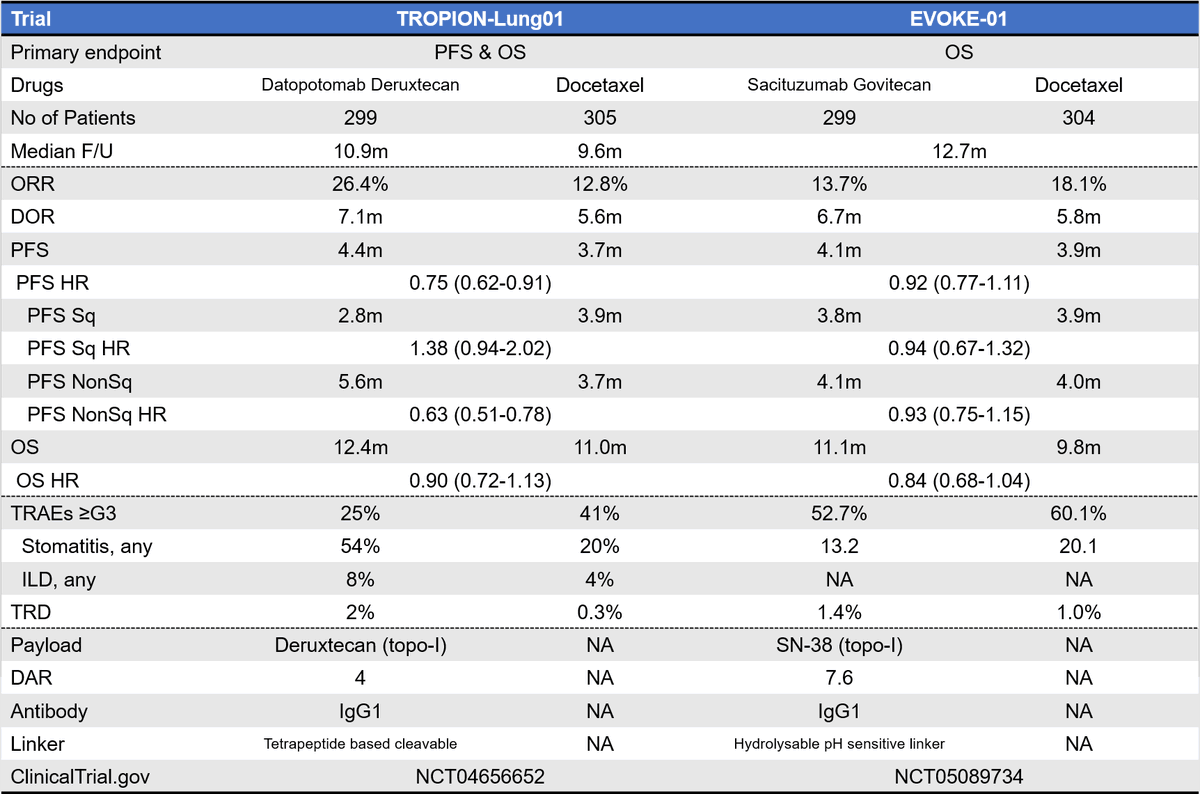
🔍Sport the difference🔎 🔥TROPION-Lung01 ✅PFS HR 0.75 (0.62-0.91)☀️ ✅OS HR 0.90 (0.72-1.13)🌧️ ✅"Clinically meaningful OS📈" 🔥EVOKE-01 ✅PFS HR 0.92 (0.77-1.11)🌧️ ✅OS HR 0.84...
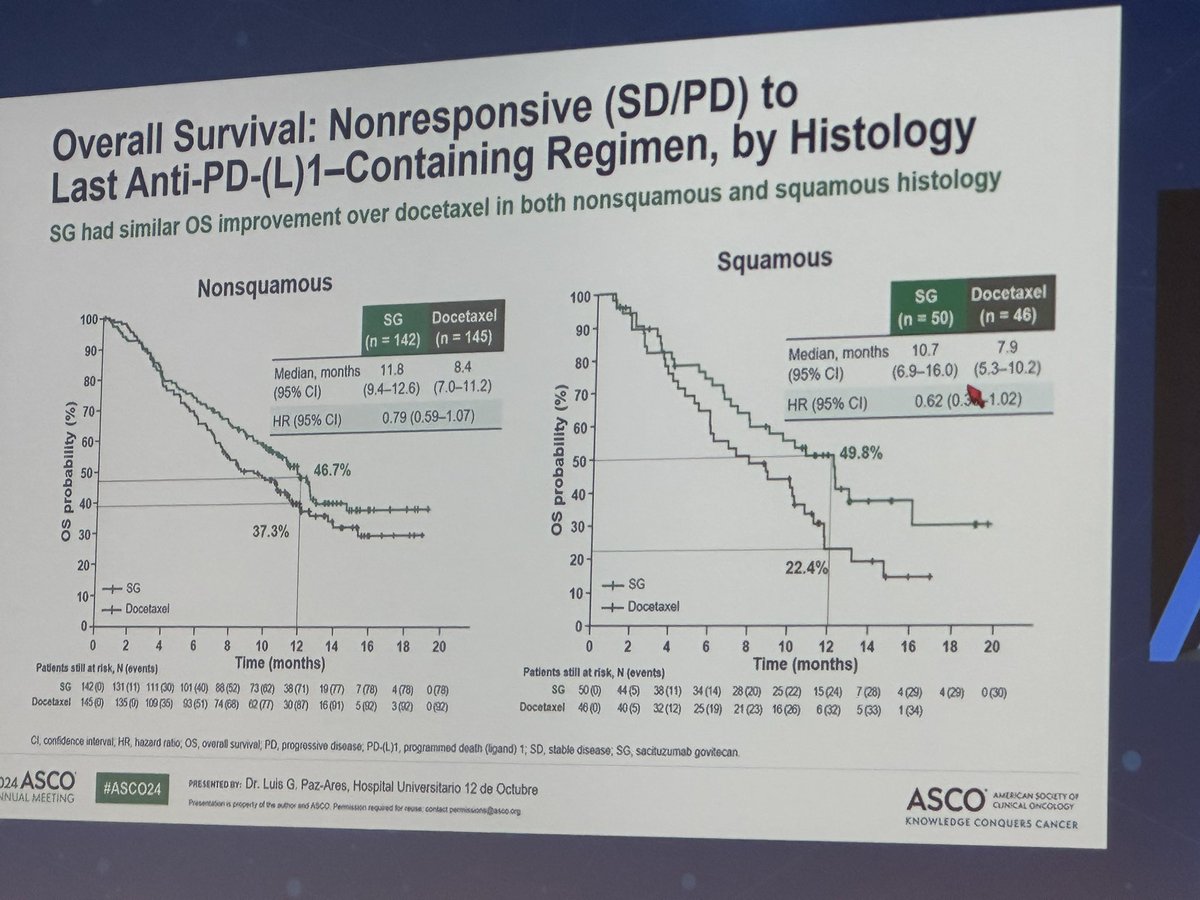
#ASCO24 EVOKE-01 on SG vs Docetaxel in 2L NSCLC ✔️Negative for primary endpoint of OS ✔️>3m OS benefit in pts non-responsive to prior ICI ✔️Similar benefit across...
EVOKE-01 sacituzumab govitecan vs Docet in 2L is ⛔️for OS.« Traffic light »🚦of ADCs in NSCLC is red. New biomarkers as targets for ADCs (current are prognostic), better safety of ADCs and explore mec...

#ASCO24 EVOKE-01 study: SG vs docetaxel mPFS➡️4.1 vs 3.9 mo (NS) mOS➡️11.1 vs 9.8 mo (NS) 💥SG was not superior to docetaxel in patients previously receiving platinum and...

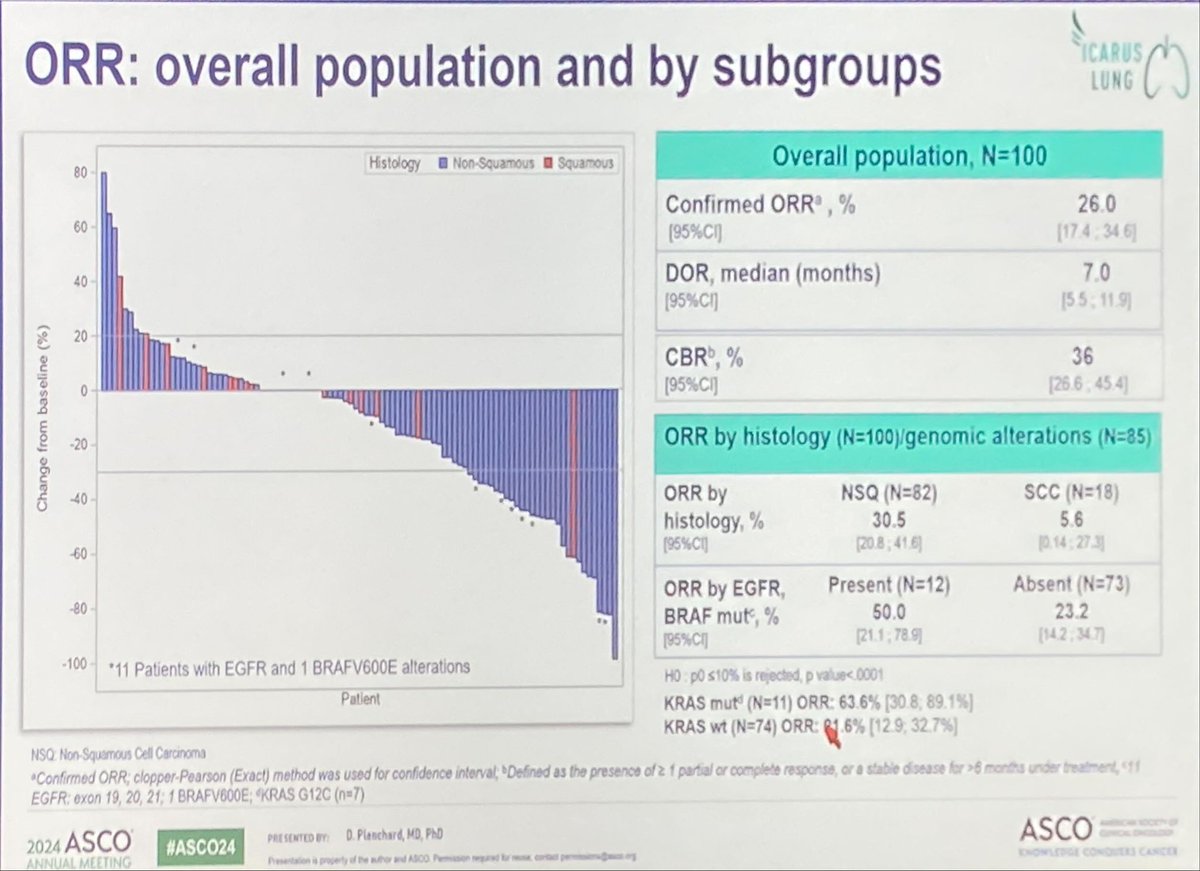
Happening NOW: mNSCLC Oral Abstracts Emerging Antibody-Drug Conjugates 🔹EVOKE-01: Phase 3 sacituzumab govitecan v docetaxel 🔸ICARUS-LUNG01: Phase 2 Dato-DXd 🔹OptiTROP-Lung01: Phase 2 1L sacituzumab...

⬇️ EVOKE-01: negative study overall but potential signal for TROP2 ADC SG in pts who had SD or PD as prior best response to IO. We need to understand dynamic + longitudinal nature of TROP2...

Dr. @LuisPaz_Ares presents EVOKE-01 results Sacituzumab govitecan vs docetaxel in 2L mNSCLC Sacituzumab does not meet primary end-point of statistically sig OS or PFS benefit, but mild...
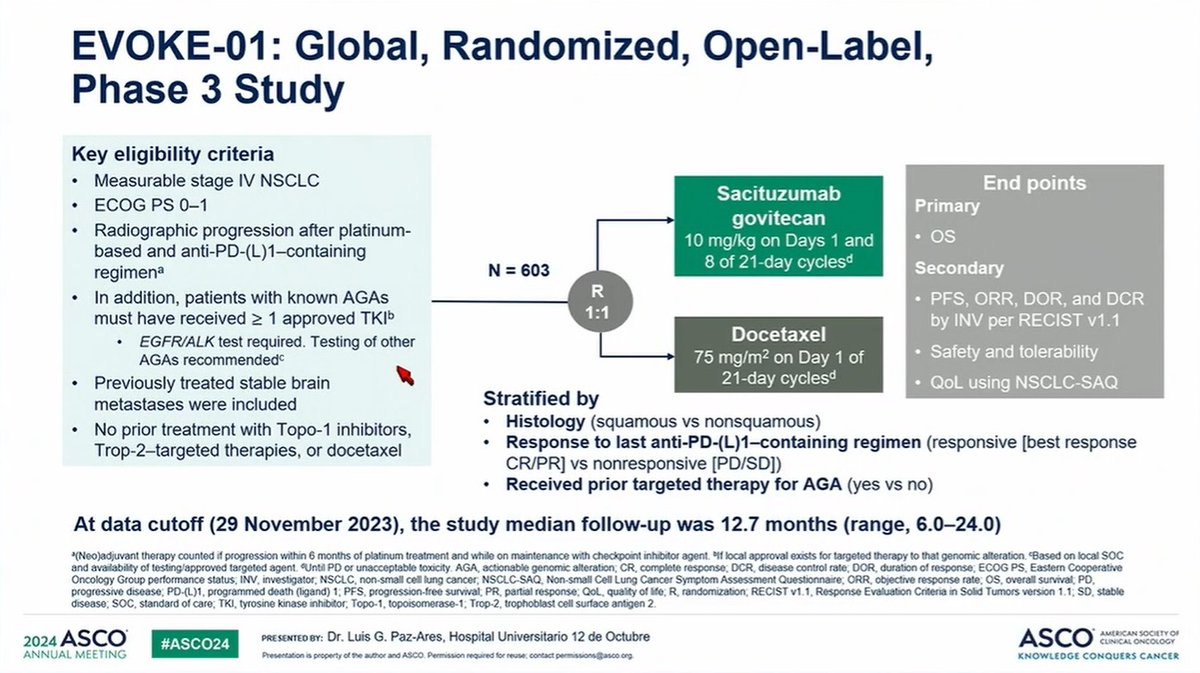
EVOKE-01 is a Phase III, global, multi-center, open-label trial that evaluated sacituzumab govitecan (Trodelvy) versus docetaxel in patients with previously treated advanced or metastatic NSCLC. The trial enrolled 603 patients randomized 1:1 whose cancer had progressed on or after platinum-based chemotherapy and checkpoint inhibitor therapy. EVOKE-01 did not meet its primary endpoint of overall survival, showing a numerical but not statistically significant improvement (HR 0.84; p=0.0534). Following discussions with regulators, Gilead formally discontinued development of sacituzumab govitecan in second-line-plus NSCLC.
Phase III, global, multi-center, open-label, 1:1 randomized trial comparing sacituzumab govitecan 10 mg/kg IV on days 1 and 8 of a 21-day cycle versus docetaxel IV on day 1 of a 21-day cycle. Treatment continued until disease progression or unacceptable toxicity. No companion diagnostic was required.
Adults aged 18+ with stage IV NSCLC (squamous or non-squamous) that had progressed after at least one platinum-containing chemotherapy and at least one anti-PD-(L)1 immunotherapy for advanced or metastatic disease. Patients with actionable genomic alterations must have also received approved targeted therapy. Enrolled 603 patients between November 2021 and May 2023.
Sacituzumab govitecan (Trodelvy) 10 mg/kg IV on days 1 and 8 of each 21-day cycle (n=299) versus docetaxel IV on day 1 of each 21-day cycle (n=304).
Primary endpoint: overall survival (OS). Key secondary endpoints: progression-free survival (PFS), objective response rate (ORR), duration of response (DOR), disease control rate (DCR), and safety. Patient-reported outcomes included time to first deterioration in shortness of breath (NSCLC-SAQ).
Sacituzumab govitecan did not demonstrate a statistically significant PFS benefit versus docetaxel. Median PFS was 4.1 months (95% CI: 3.0-4.4) versus 3.9 months (95% CI: 3.1-4.2), with an HR of 0.92 that was not statistically significant. Six-month PFS rates were 33.7% versus 31.4%. PFS results were consistent with the lack of meaningful separation between arms.
The primary OS endpoint was not met. Median OS was 11.1 months for sacituzumab govitecan versus 9.8 months for docetaxel (HR 0.84; 95% CI: 0.68-1.04; one-sided p=0.0534). Twelve-month OS rates were 46.6% versus 36.7%. A pre-specified (but not alpha-controlled) subgroup of patients non-responsive to prior anti-PD-(L)1 therapy showed median OS of 11.8 versus 8.3 months (HR 0.75; 95% CI: 0.58-0.97), but survival curves crossed multiple times and the confidence interval upper bound was close to 1.00. Gilead attempted to pursue regulatory filing based on this subgroup but the FDA declined to support it.
The safety profile was consistent with prior sacituzumab govitecan studies. Grade 3+ treatment-related AEs occurred in 66.6% of SG patients. Key toxicities: neutropenia 37.5% any grade (Grade 3+ 24.7%, vs 37% for docetaxel), diarrhea 52.7% any grade (Grade 3+ 10.5%, vs 4% docetaxel), fatigue 56.8% (Grade 3+ 12.5%), febrile neutropenia 7.8%. Treatment discontinuation due to AEs was lower with SG (9.8-10%) versus docetaxel (16.7-17%), though dose pauses were more frequent (58% vs 28%). Treatment-related deaths: 3.4% SG versus 4.5% docetaxel.
EVOKE-01 represents a high-profile failure for the TROP2-directed ADC class in NSCLC. Despite a numerical OS trend favoring sacituzumab govitecan, the trial missed statistical significance and the 1.3-month absolute benefit lacks clinical meaningfulness. Docetaxel actually outperformed on ORR (18.1% vs 13.7%). Gilead has discontinued further evaluation of Trodelvy in 2L+ NSCLC. The result contrasts with datopotamab deruxtecan (Tropion-Lung01), which showed PFS benefit in non-squamous histology. Gilead continues to pursue Trodelvy in 1L NSCLC combinations (EVOKE-02/EVOKE-03 with pembrolizumab).
EVOKE-01 is a Phase 3 trial of sacituzumab govitecan (Trodelvy), a TROP2-directed antibody-drug conjugate, versus docetaxel in adults with metastatic non-small cell lung cancer that progressed after platinum-based chemotherapy and immunotherapy (NCT05089734).
No. EVOKE-01 did not meet its primary overall survival endpoint. Median overall survival was 11.1 months with sacituzumab govitecan versus 9.8 months with docetaxel (HR 0.84; 95% CI 0.68-1.04; one-sided p=0.0534), which did not reach statistical significance.
No. Sacituzumab govitecan (Trodelvy) is not FDA approved for non-small cell lung cancer. It is FDA approved for metastatic triple-negative breast cancer, HR-positive/HER2-negative metastatic breast cancer, and locally advanced or metastatic urothelial cancer.
A pre-specified (but not alpha-controlled) subgroup of patients whose disease did not respond to prior immunotherapy showed a numerically larger overall survival difference. Because this was exploratory and the primary endpoint was not met, it is hypothesis-generating rather than practice-changing.
Sacituzumab govitecan (Trodelvy) is developed by Gilead Sciences.




















