Stage III resected colon cancer, ctDNA-guided adjuvant strategy — Australasian Gastro-Intestinal Trials Group (AGITG)
Visit Interactive Trial Page →















Top tweets by impressions — click to view on X
Lot of discussion to surely follow the DYNAMIC-III #ASCO25 oral. For rand trials of ctDNA-guided adj therapy in colon cancer to date:
➕trials
DYNAMIC, CALGB 80702 (post-hoc)
➖DYNAMIC III, ALTAIR,…
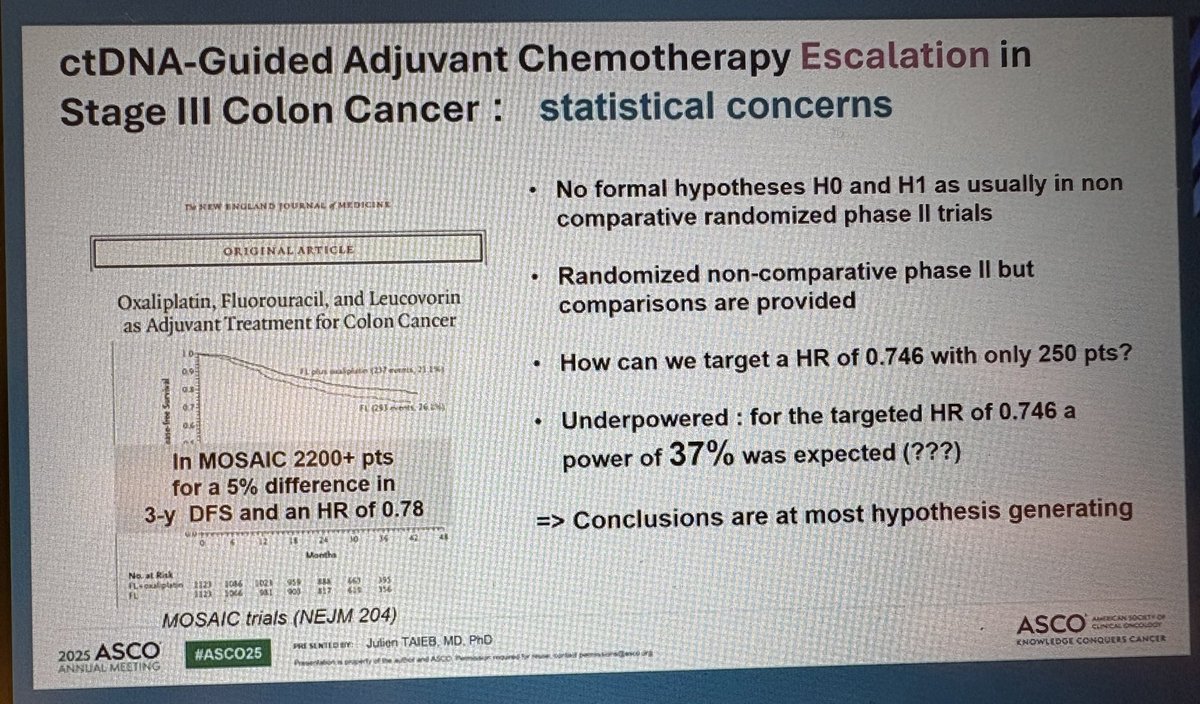
Dr. Taken discussant w/insight into DYNAMIC-III, underpowered for target HR 0.746 w/n=250 pts (MOSAIC needed >2200 pts for HR 0.78), heterogeneity in FOLFOXIRI duration. A power of 37% makes…
ctDNA-guided adj CTx escalation in stage III CRC
#ASCO25
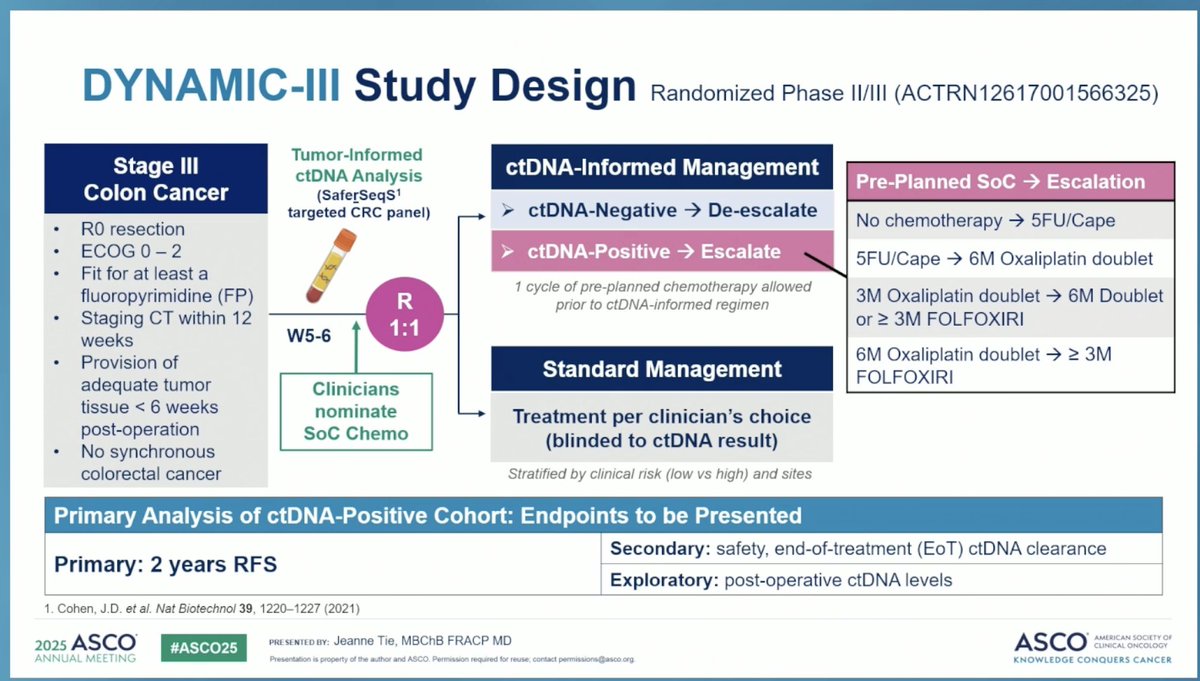
🔎Primary analysis of the ctDNA-positive cohort from the randomized AGITG DYNAMIC-III trial
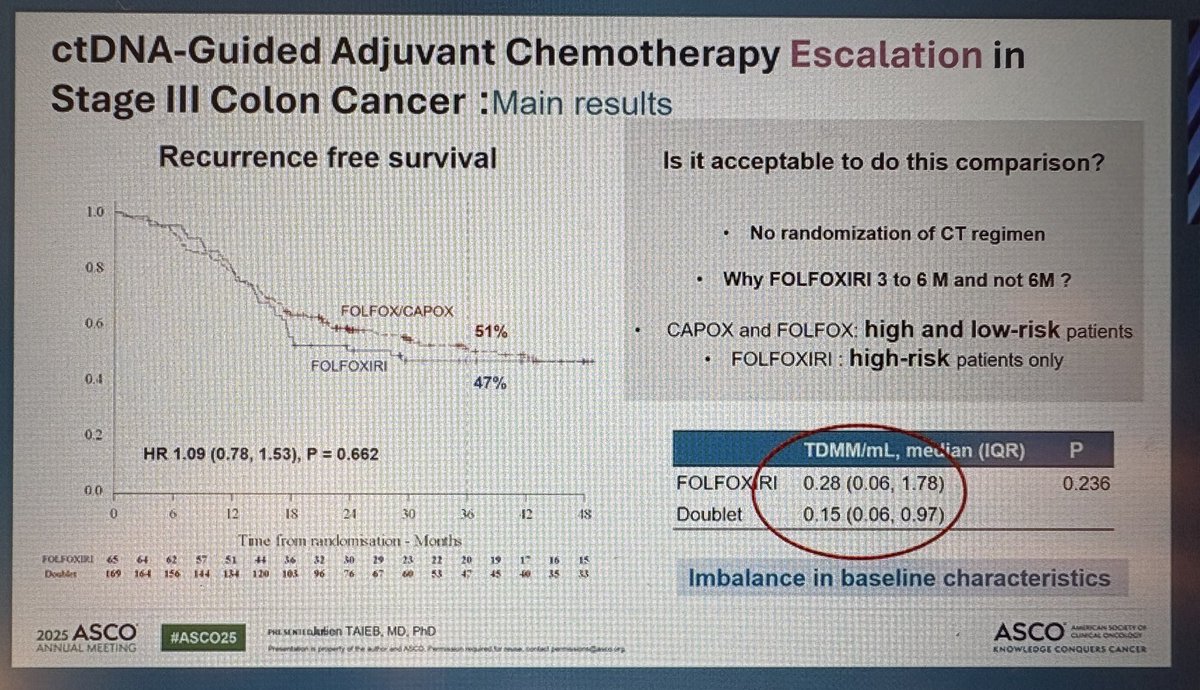
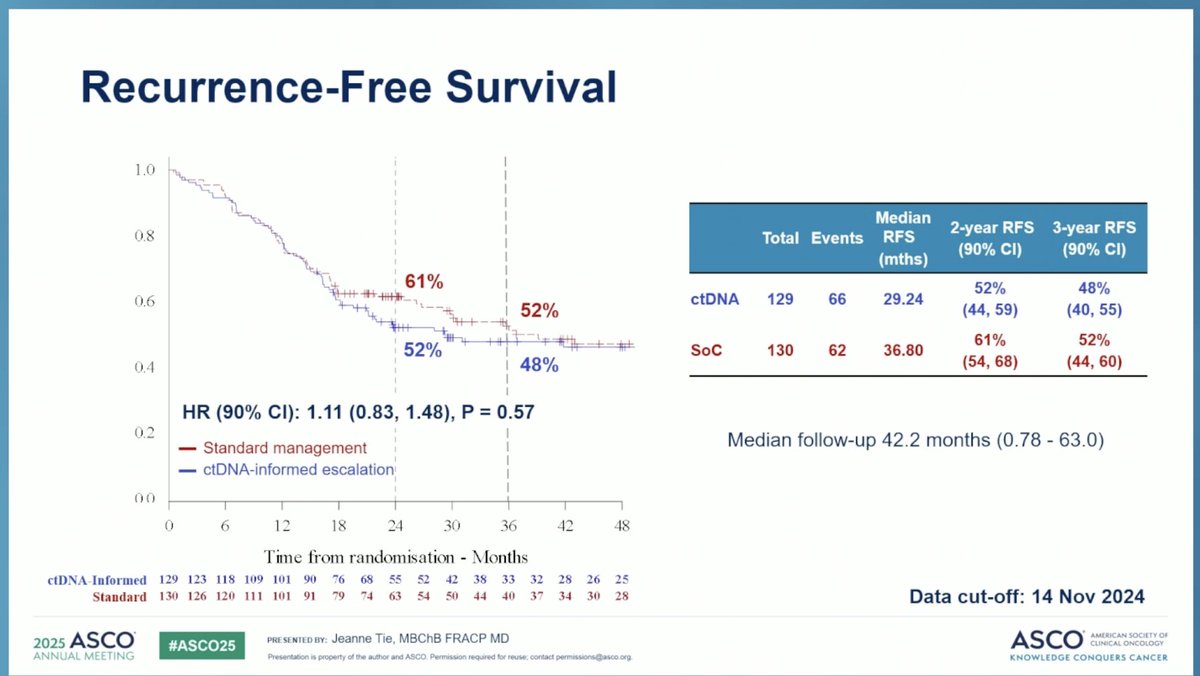
👉mRFS 29 vs 36 mo
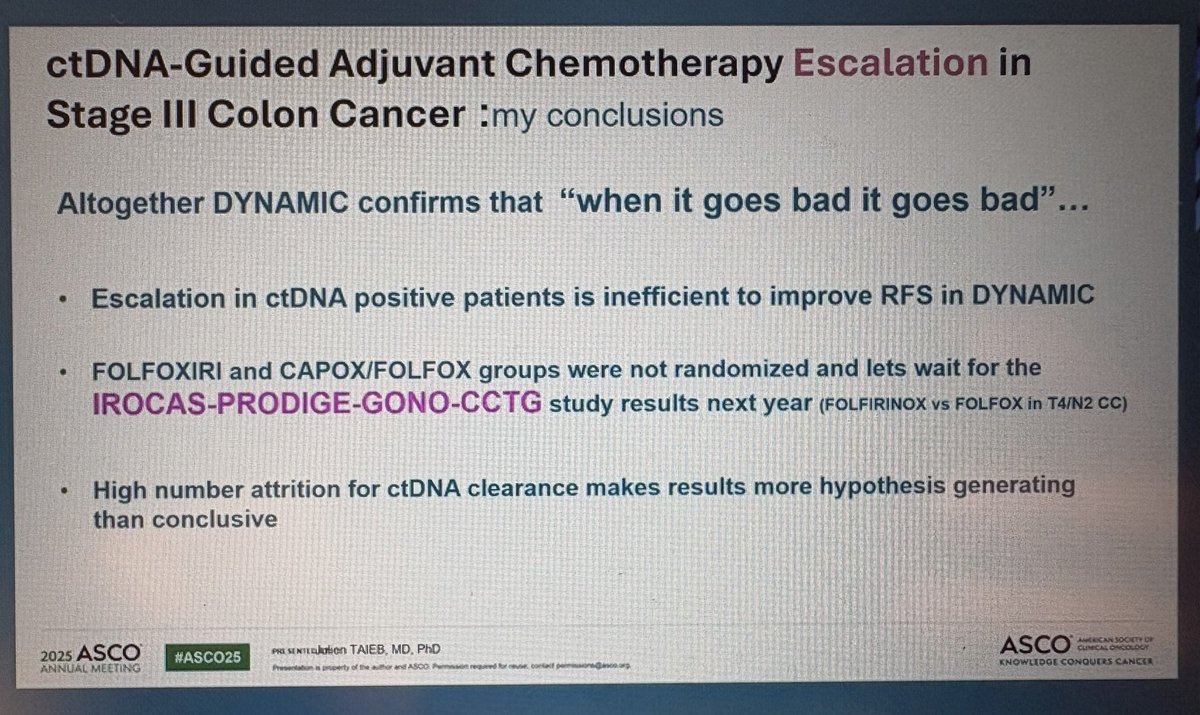
👉CTx escalation does not improve…
💎 #ESMO25 Presidential Session w/ @JeanneTie #ColorectalCancer – Phase III DYNAMIC-III: ctDNA-guided de-escalation after surgery in stage III colon cancer
In ctDNA⁻ patients:
☄️ 3-year RFS 85.3%…
DYNAMIC III: another study showing ctDNA prognostic, but not predictive.
At this point, the main scenario I see for ctDNA guiding treatment decision making in CRC is potentially selecting patients…
Very interesting data❗️
✳️Some sobering facts but few things important to note here:
👉ctDNA assays used in these studies matter. We have seen this in COBRA trial.
👉The study allowed optional…
📢 #ASCO25 GI – DYNAMIC-III Trial
🧬 Can escalation of chemo overcome ctDNA+ risk in stage III colon cancer?
🧪 Design:
961 pts randomized to:
➡️ ctDNA-informed ACT escalation
➡️ Standard ACT (SOC)
📈…

DYNAMIC-III study shows no benefit of giving more chemo for ctDNA+ stage 3 colon cancer.
I always say, ctDNA is amazing and cool, but it doesn't make FOLFOX (or irinotecan) more effective. #ASCO25…

❔ ctDNA detection is PROGNOSTIC for inferior outcomes following resection of stage III colon cancer, but is treating more aggressively better?
‼️ NO improvement in RFS by escalating treatment with a…

4. #DYNAMIC: ctDNA to escalate treatment in Stage III colon cancer.
- Post-surgery, ctDNA+ is high: 3 yrs recurrence risk RFS ~50%.
- FOLFOXIRI (escalation) didn’t reduce risk: 2-yr RFS 52% vs…
Overall non-inferiority not met, but trial supports ctDNA-informed personalization. De-escalation is feasible for ctDNA-negative low-risk patients. ctDNA-positive disease needs novel strategies beyond chemo intensification.
3-year RFS was 85.3% in the ctDNA-guided arm vs. 88.1% with standard care (difference -2.8%, 97.5% lower CI -8.0%). Non-inferiority margin of 7.5% was NOT met. Median RFS 29.24 vs. 36.8 mo (HR 1.11, 90% CI 0.83-1.48 (90% CI)).
OS data were not the primary focus of the analysis. ctDNA-guided de-escalation reduced oxaliplatin exposure and associated neuropathy, particularly in low-risk T1-3N1 disease.
De-escalation arm reduced oxaliplatin exposure and associated peripheral neuropathy. Specific Grade ≥3 AE rates were not detailed in the primary publication; the key safety signal is favorable toxicity reduction with de-escalation.
⚠️ Non-inferiority not met — but practice-informing for ctDNA-informed personalization. Overall non-inferiority not met, but trial supports ctDNA-informed personalization. De-escalation is feasible for ctDNA-negative low-risk patients. ctDNA-positive disease needs novel strategies beyond chemo intensification.