BRAF V600E-mutant metastatic colorectal cancer (1L) — Pfizer Inc. (via Array BioPharma) + Eli Lilly (cetuximab)
Visit Interactive Trial Page →











Top tweets by impressions — click to view on X
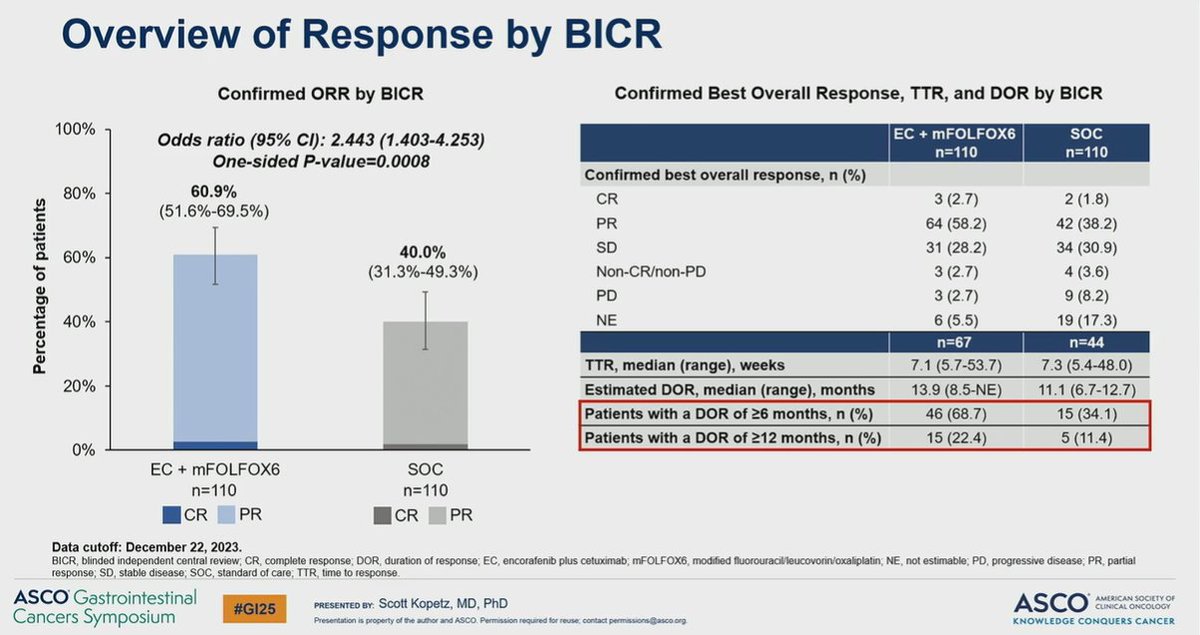
Results of Phase III BREAKWATER for BRAF V600E MT stage IV tx naive pts fulfilled primary endpoint for ORR (61% vs. 40%) and early trend for OS (add'l data to follow) defining a NEW standard of care.…
#ASCO2025
🚨 BREAKWATER OS data lands—and it must redefine 1L standard of care in BRAF V600E-mutant mCRC.
EC + mFOLFOX6 vs SOC (chemo ± bevacizumab):
📊 PFS: 12.8 vs 7.1 mo (HR 0.53, p < 0.0001)
🧬…
#ASCO25 @NEJM
BREAKWATER: Encorafenib + cetuximab + mFOLFOX6 vs standard care in 1L BRAF V600E mCRC
PFS➡️12.8 vs 7.1 mo✅️
OS➡️ 30.3 vs 15.1 mo✅️👏
💥For one of the hardest-to-treat mCRC subtypes,…
Day 1 #ASCO25 highlights:
1. Review on recent approvals
2. #BREAKWATER (update): BRAF+ mCRC
3. #CM8HW (update): MSI-H mCRC
4. #DYNAMIC: ctDNA in colon ca
5. #CAIRO6: periOP Rx in peritoneal…
Excellent slides to summarize top gi data from day 1 of #asco25 @ASCO @OncoAlert https://t.co/kedPg1SRtG

And the fun starts!
From @asco #asco25 press release
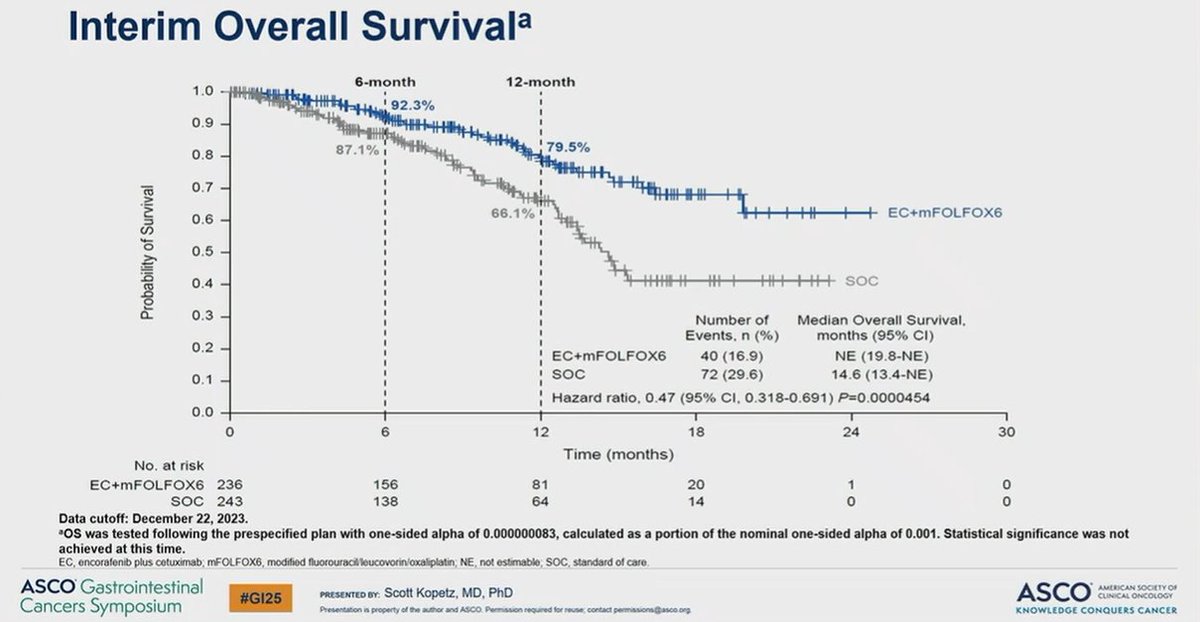
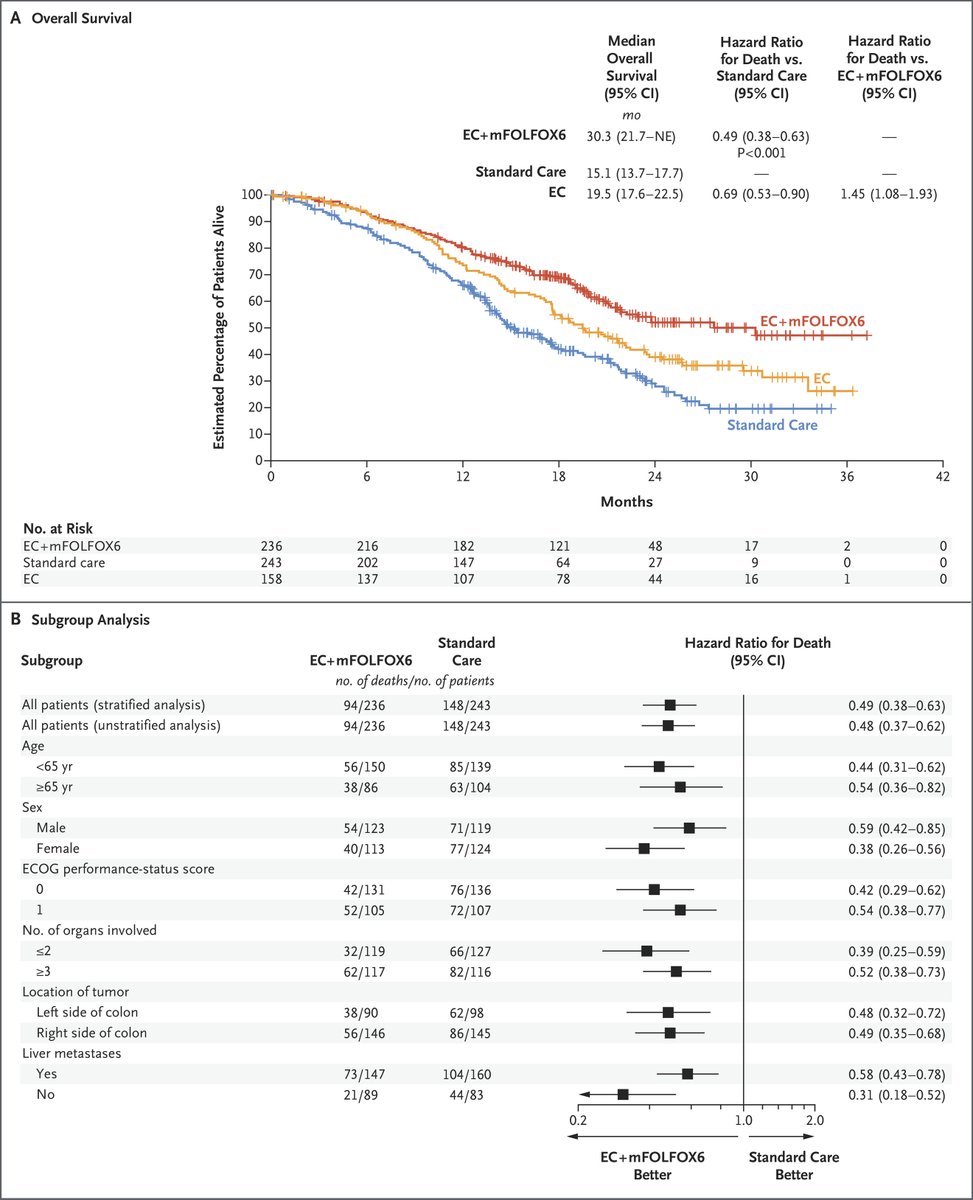
Overall survival was 30.3 months in the encorafenib/cetuximab with mFOLFOX6 arm, 19.5 months in the encorafenib/cetuximab alone arm, and 15.1…

You don't see survival curves like this often in colorectal cancer, let alone for BRAF mutated CRC.
And Median OS: 30.3 vs. 15.1 months. Wow.
What a win for our patients! #ASCO25…
🔥🔥🔥BREAKWATER🔥🔥🔥
BRAF V600E mut #CRC
SOC (FOLFOX) +/- encorafenib + cetuximab
EC + FOLFOX shows:
✅⬆️ORR
✅Strong suggestion of ⬆️OS
🚨EC + FOLFOX is a new SOC‼️
#GI25 @ASCO @OncoAlert…

#ASCO25 1st practice changing presentation, which has already been our practice since the initial readout for our patients with #BRAFV600E mutant colorectal cancer.
More options for our patients.👏🏽…
Along this same theme pls visit Board E10 #GI26 @asco Abs# 122 #Breakwater @PfizerOncMed #BRAFV600E post hoc analysis of EOCRC vs AOCRC:
- Better ORR
BUT
- Shorter OS
Indicating the unmet need…
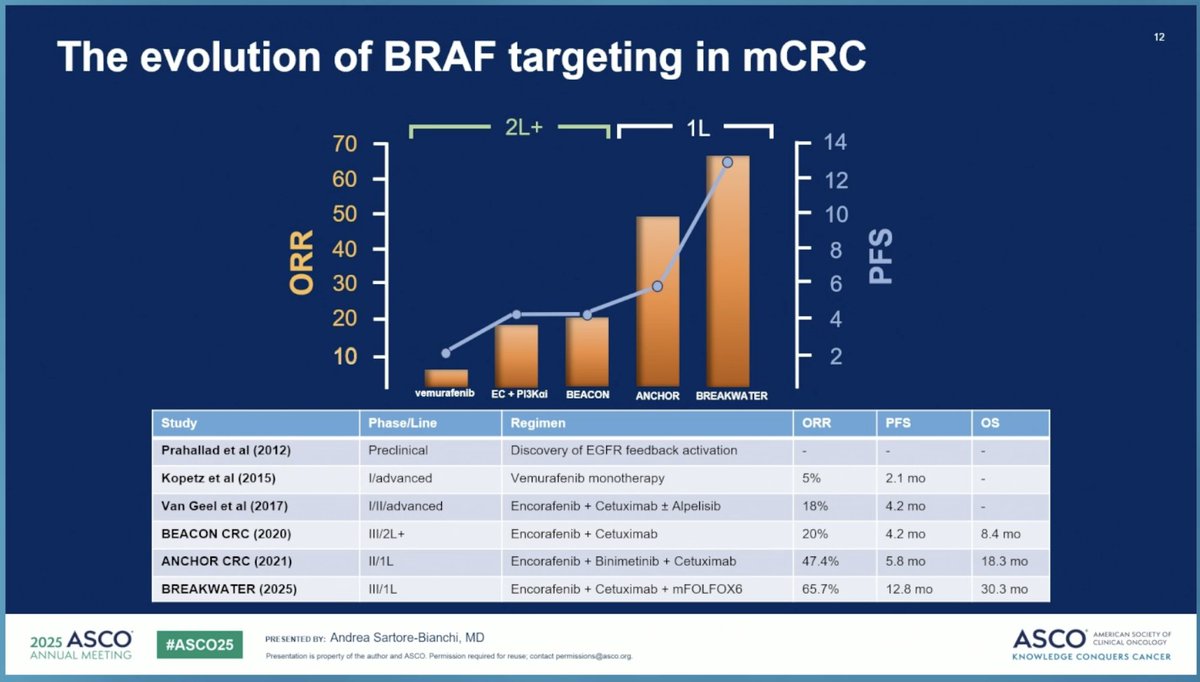
New 1L standard of care for BRAF V600E-mutant mCRC. Near-tripled OS (30.3 vs 15.1 mo, HR 0.49) in a historically aggressive subtype. Cohort 3 (FOLFIRI backbone) is extending evidence to patients with oxaliplatin contraindications.
Median PFS was 12.8 months with encorafenib+cetuximab+mFOLFOX6 vs. 7.1 months with standard chemotherapy (HR 0.53, 95% CI 0.41-0.68, P<0.0001). ORR was 61% vs. 40% (odds ratio 2.443).
Median OS was 30.3 months with EC+mFOLFOX6 vs. 15.1 months with SOC (HR 0.49, 95% CI 0.38-0.63, P<0.0001). Near-tripled median survival in this historically aggressive subtype.
Grade ≥3 all-cause AEs occurred in 74.0% with EC+mFOLFOX6 vs. 61.0% with SOC. Grade ≥3 treatment-related AEs: 69.7% vs. 53.9%. Safety consistent with individual component profiles; no unexpected signals. Cutaneous malignancy monitoring per BRAF inhibitor class effect.
✅ New 1L standard of care for BRAF V600E-mutant mCRC. New 1L standard of care for BRAF V600E-mutant mCRC. Near-tripled OS (30.3 vs 15.1 mo, HR 0.49) in a historically aggressive subtype. Cohort 3 (FOLFIRI backbone) is extending evidence to patients with oxaliplatin contraindications.