First-line recurrent or metastatic non-squamous NSCLC (NSQ-NSCLC) — Shanghai Junshi Biosciences
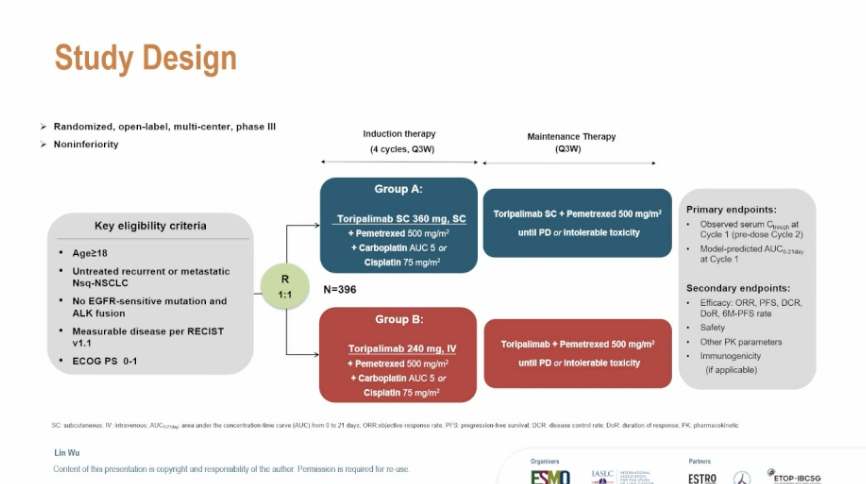
Discover KOL Sentiment on JS001sc →Design - Phase 3 open-label randomized study of subcutaneous toripalimab (JS001sc) + chemotherapy vs intravenous toripalimab + chemotherapy, 1L recurrent/metastatic non-squamous NSCLC (NCT06505837; Junshi; PI Prof. Lin Wu).
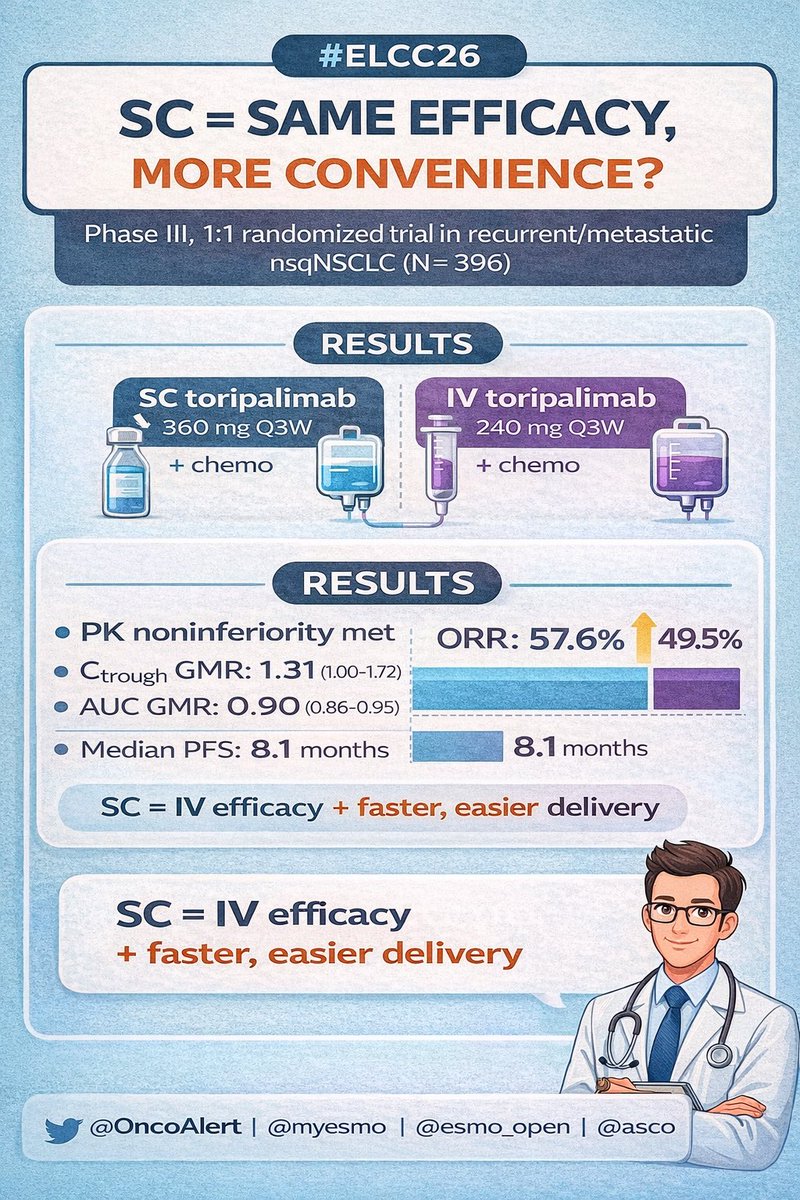
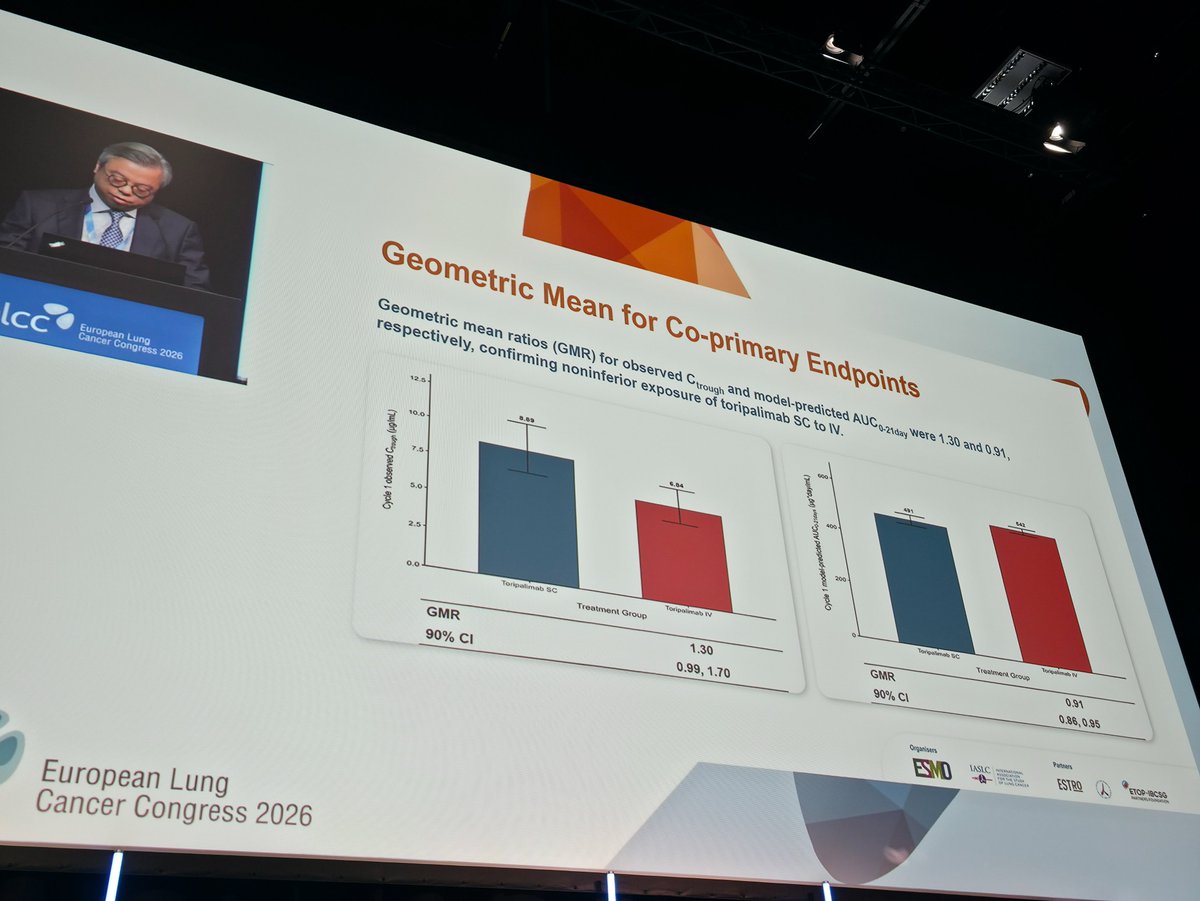
Primary endpoint (PK non-inferiority) - Met (reported November 2025): subcutaneous JS001sc + chemotherapy achieved non-inferior drug exposure versus intravenous toripalimab + chemotherapy.
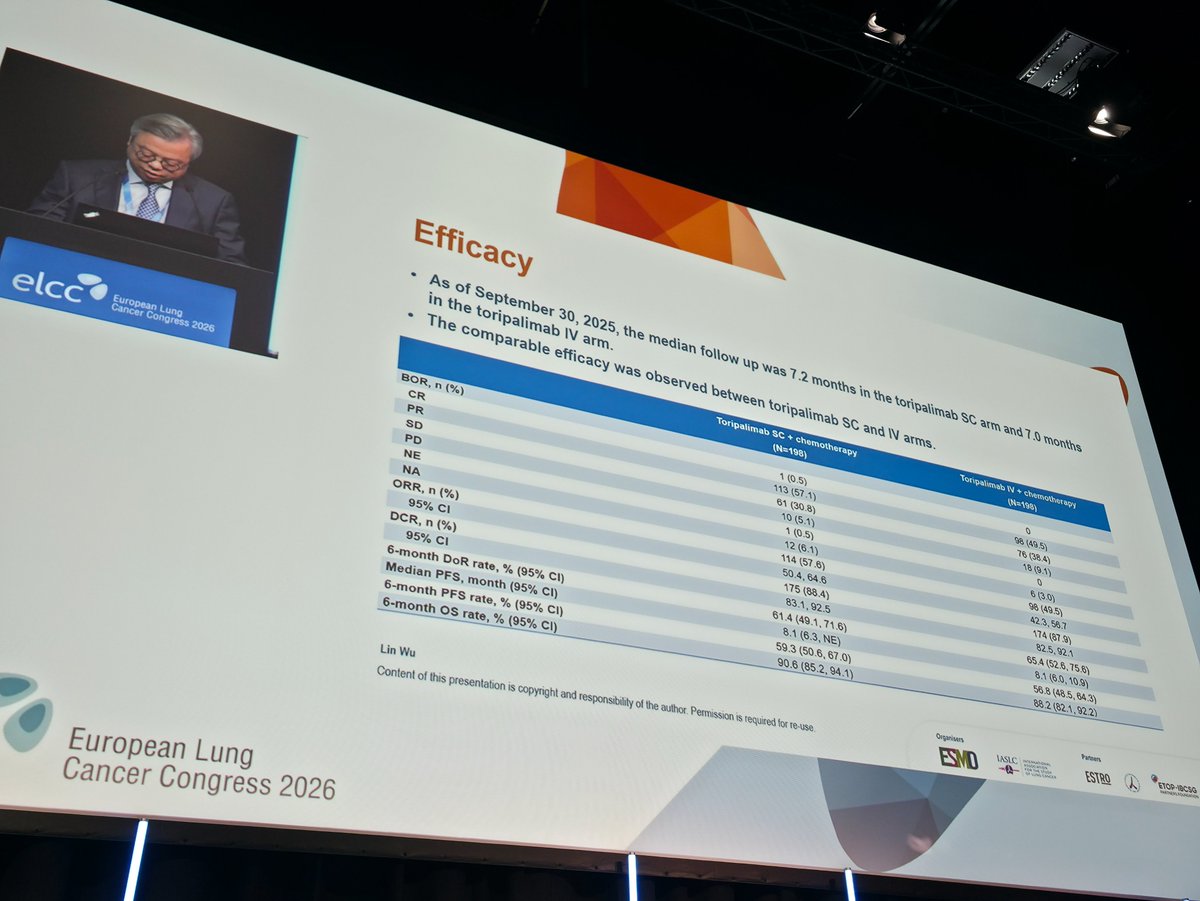
Efficacy / safety - OS, ORR and PFS not yet disclosed - reported by the sponsor as comparable, with detailed results to follow at an upcoming conference; safety described as comparable to intravenous toripalimab.
Regulatory - China NMPA New Drug Application accepted March 9, 2026 (across 12 indications per sponsor); not FDA approved.
Context - First China-developed subcutaneous anti-PD-1 formulation to reach Phase 3 and NDA filing; intravenous toripalimab (Loqtorzi in the US) is separately approved for nasopharyngeal carcinoma.
Sponsor / drug - Shanghai Junshi Biosciences; subcutaneous toripalimab (JS001sc).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.





Top tweets by impressions — click to view on X
🆙 #ELCC26 @myESMO @IASLC 🇩🇰
🔥Mini Oral session 2
☑️Tripalimab: Subcutaneous vs. IV
🎯Noninferiority of exposure of SC to IV tripalimab
🎙️Dr. Lin Wu
🎙️Chair: Dr. Kersti Oselin…
🔥 SC vs IV toripalimab in 1L nsqNSCLC - practice changing convenience? #ELCC26
Phase III data comparing subcutaneous vs intravenous toripalimab + chemo 👇
🧬 Study population
•Recurrent/metastatic…
Bioequivalence and pharmacodynamics of Toripalimab at #ELCC2026 @OncoAlert https://t.co/DOhUFW2cZw
@MARIANOPROVENCI chairman of @gecp_org discuss trial dealing with Toripalimab subcutaneous or intravenous formulation combined with chemotherapy in the treatment of advanced NSCLC at #ELCC2026…
JS001sc is the first China-developed subcutaneous anti-PD-1 monoclonal antibody to reach Phase 3 and NDA filing. Toripalimab was the first domestic Chinese PD-1 approved (originally for melanoma 2018, expanded to 12 indications including 1L NSCLC, NPC, esophageal). The Phase 3 JS001sc-002-III-NSCLC trial demonstrated non-inferior PK exposure vs. IV toripalimab plus comparable efficacy and safety. NMPA accepted NDAs across all 12 approved indications (March 2026). Parallels global SC IO trend (nivolumab SC FDA-approved 2024 via CheckMate 67T). Offers convenience, reduced infusion chair time, potential home administration.
Median: non-inferior exposure (JS001sc + chemo) vs. reference (JS001 IV + chemo). Phase 3 multi-center open-label randomized study (JS001sc-002-III-NSCLC), NCT06505837. Principal investigator Professor Lin WU (Hunan Cancer Hospital). Population: first-line recurrent or metastatic non-squamous NSCLC. Arms: JS001sc (toripalimab SC) + chemo vs JS001 (IV toripalimab) + chemo. Primary endpoints: drug exposure (non-inferiority), efficacy, safety. RESULTS: JS001sc exposure NON-INFERIOR to JS001, with comparable efficacy and safety profiles — primary endpoints MET. First Phase 3 of a domestic China anti-PD-1 SC formulation. Specific HR, ORR, PFS, OS numerical values not disclosed in press release; data to be presented at international academic conference.
OS, ORR, PFS data not yet disclosed — comparable per sponsor; detailed results at upcoming conference. Non-inferiority PK design with efficacy/safety as co-objectives.
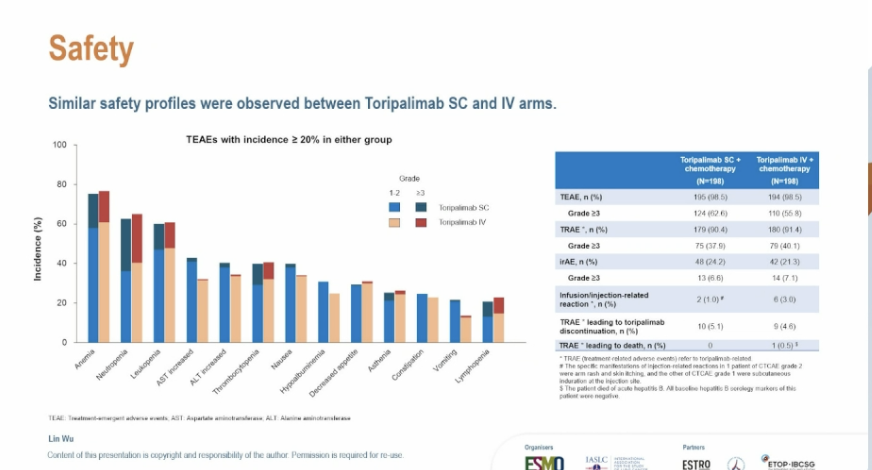
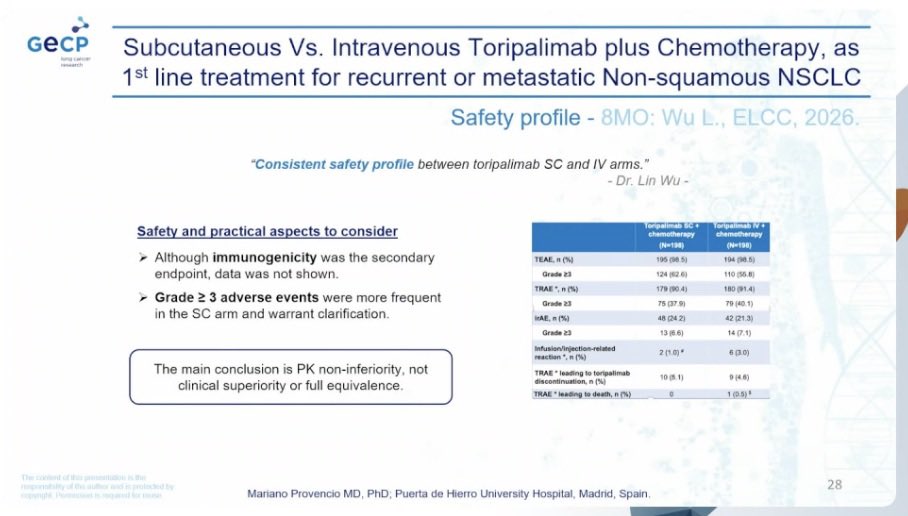
Comparable safety to IV toripalimab per sponsor press release. No specific G≥3 TRAE rates disclosed.
✅ China NDA filed (March 2026): First domestic SC anti-PD-1 formulation across 12 indications. JS001sc is the first China-developed subcutaneous anti-PD-1 monoclonal antibody to reach Phase 3 and NDA filing. Toripalimab was the first domestic Chinese PD-1 approved (originally for melanoma 2018, expanded to 12 indications including 1L NSCLC, NPC, esophageal). The Phase 3 JS001sc-002-III-NSCLC trial demonstrated non-inferior PK exposure vs. IV toripalimab plus comparable efficacy and safety. NMPA accepted NDAs across all 12 approved indications (March 2026). Parallels global SC IO trend (nivolumab SC FDA-approved 2024 via CheckMate 67T). Offers convenience, reduced infusion chair time, potential home administration.
JS001sc-002-III-NSCLC (NCT06505837) is a Phase 3, multicenter, open-label, randomized study by Shanghai Junshi Biosciences comparing a subcutaneous formulation of toripalimab (JS001sc) plus chemotherapy against intravenous toripalimab plus chemotherapy as first-line treatment of recurrent or metastatic non-squamous non-small cell lung cancer. The principal investigator is Professor Lin Wu.
The trial's primary endpoint - non-inferior pharmacokinetic (drug exposure) of the subcutaneous formulation versus intravenous toripalimab plus chemotherapy - was met, as reported by the sponsor in November 2025. Overall survival, objective response rate and progression-free survival had not been publicly disclosed at the time the page was compiled, with the sponsor describing them as comparable and detailed results expected at an upcoming conference.
No. JS001sc is investigational and not FDA approved. A China NMPA New Drug Application for the subcutaneous formulation was accepted on March 9, 2026. The intravenous form of toripalimab is approved in the US as Loqtorzi for nasopharyngeal carcinoma, but that is a different (intravenous) product and indication.
A subcutaneous anti-PD-1 formulation can shorten administration time and reduce infusion-chair and resource burden compared with intravenous dosing, potentially improving convenience for patients and clinics. JS001sc is described as the first China-developed subcutaneous anti-PD-1 antibody to reach Phase 3 and regulatory filing.
The sponsor reported that the safety of subcutaneous JS001sc plus chemotherapy was comparable to intravenous toripalimab plus chemotherapy, without disclosing specific grade 3 or higher treatment-related adverse event rates at the time of the press release. Full safety data are expected with the detailed efficacy readout.