













Top 10 by impressions - click to view on X
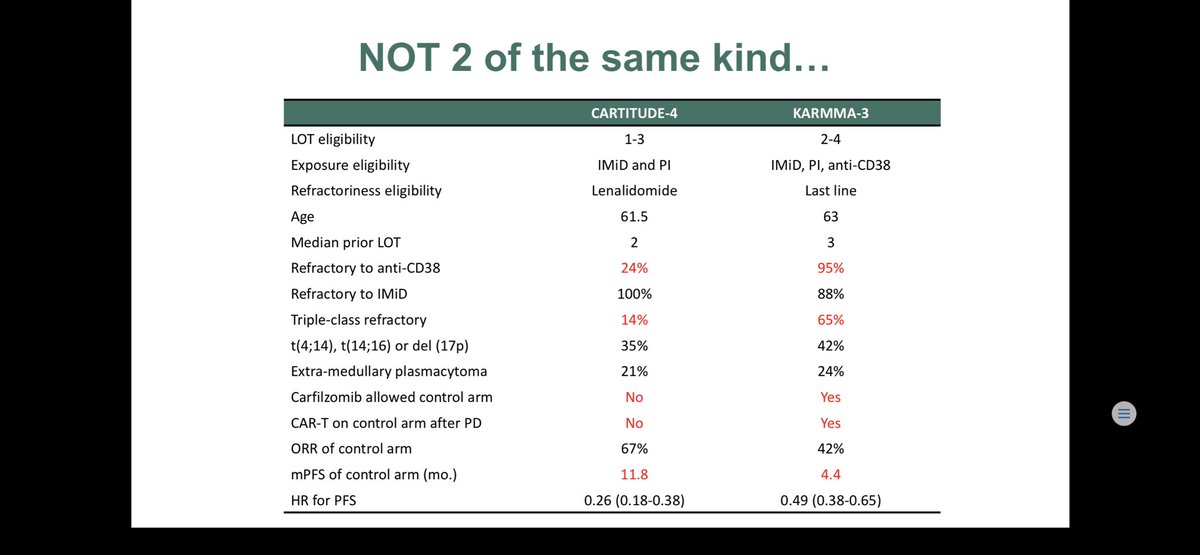
We had the privilege to contribute to both Cartitude-4 and KarMMa-3. Crucial differences between these important studies often overlooked #myeloma 1/X
More good news for patients. We used to dream about all these options!! #abecma #bcma #rrmm #mmsm will you offer...
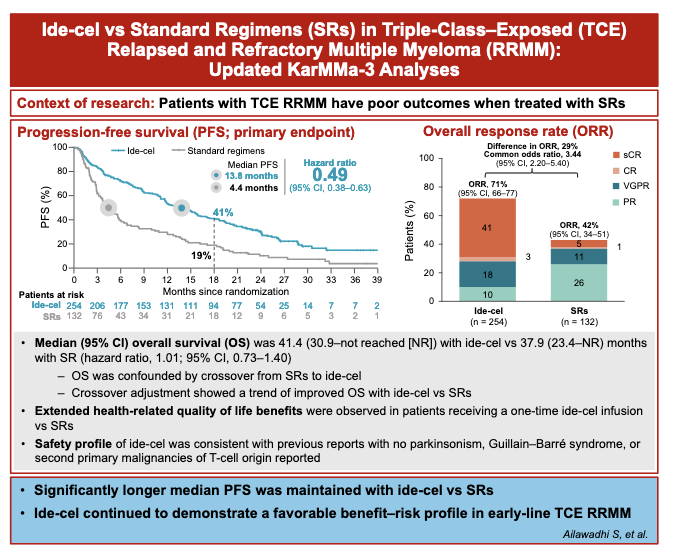
#Myeloma Paper of the Day: Updated KarMMa-3 analyses shows Ide-cel improved median PFS vs. standard regimens (13.8 vs. 4.4 months; HR 0.49; 95% CI 0.38-0.63) and ORR (71% vs. 42%;...
We are all tempted to compare to cilta-cel. The CARTITUDE-4 trial is positive on a press-release, but please remember, the patient population in that trial will be less heavily pre-treated (1-3...
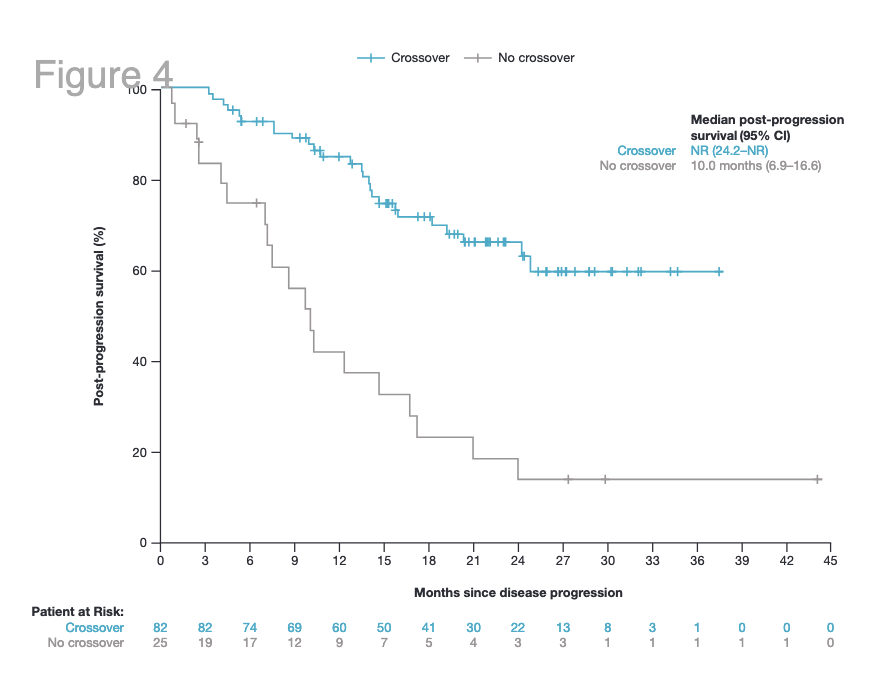
It is sad that a very efficient drug, ide-cel, is likely being removed from the German market. What factored into this decision is the lack of a clear OS benefit. KarMMa-3 allowed cross-over after...

Reflects all the issues with PRO data in most RCTs. We wouldn't tolerate this with PFS or OS data, hence, PRO should be held to similar standard as well IMO. I highlighted some...

@ManniMD1 Manni we have to be precise in comparing apples to apples here. There are significant differences in trial designs , post protocol therapy, bridging to name a few that I suspect...

@JanakiramMurali I agree that Ide-cel should be available (it is already) and has utility for myeloma, but the point of crossover in an RCT is to show whether sequencing matters, so if the...
Looking forward to this #ASH24 #MMsm oral by @KarenSweiss @EagleMyeloma @HealthTree! I will say that this is one of the key benefits of...

@Bethfaiman @khouri_jack @FaizAnwerMD1 Earlier CAR-T will be a part of the future undoubtedly. Sponsors for #idecel to be congratulated for allowing...
KarMMa-3 is an international, randomized, open-label Phase III trial that evaluated idecabtagene vicleucel (ide-cel, Abecma) versus standard regimens in adults with relapsed and refractory multiple myeloma who had received 2 to 4 prior lines of therapy including an immunomodulatory agent, a proteasome inhibitor, and daratumumab. The trial randomized 386 patients 2:1 to ide-cel or investigator's choice of five standard regimens. KarMMa-3 is the first Phase III trial to demonstrate superiority of a CAR-T cell therapy over standard of care in earlier-line RRMM, leading to the first FDA approval of CAR-T in this setting.
Phase III, international, open-label, 2:1 randomized trial comparing a single infusion of ide-cel (150-450 x 10^6 CAR+ T cells) to investigator's choice of five standard regimens (DPd, DVd, IRd, Kd, or EPd). Patients in the ide-cel arm underwent leukapheresis, optional bridging therapy (1 cycle), lymphodepleting chemotherapy (fludarabine + cyclophosphamide x 3 days), then a single ide-cel infusion. Crossover from standard regimens to ide-cel was permitted upon confirmed progressive disease.
Adults with RRMM who had received 2 to 4 prior regimens including an IMiD, a proteasome inhibitor, and daratumumab, and who were refractory to their last regimen. 66% had triple-class-refractory disease and 95% had daratumumab-refractory disease. ECOG PS 0-1 required. Stratified by age (<65 vs >=65), prior regimens (2 vs 3-4), and cytogenetics (high-risk vs absence/unknown).
Ide-cel arm: single infusion of ide-cel at target dose 150-450 x 10^6 CAR+ T cells after lymphodepleting chemotherapy. Standard regimen arm: continuous therapy with investigator's choice of DPd, DVd, IRd, Kd, or EPd until progression or unacceptable toxicity.
Primary endpoint: progression-free survival (PFS) assessed by blinded independent review committee (IRC) per IMWG criteria. Key secondary endpoints: overall response rate (ORR, partial response or better) and overall survival (OS). Additional secondary endpoints: complete response rate (CRR), duration of response (DOR), MRD negativity, time to response, PFS2, health-related quality of life, and safety.
At median follow-up of 18.6 months (primary analysis), median PFS was 13.3 months with ide-cel vs 4.4 months with standard regimens (HR 0.49; 95% CI 0.38-0.65; P<0.001). At the final PFS analysis (median follow-up 30.9 months), the benefit was maintained with median PFS of 13.8 vs 4.4 months (HR 0.49; 95% CI 0.38-0.63). PFS rate at 18 months was 41% with ide-cel vs 19% with standard regimens.
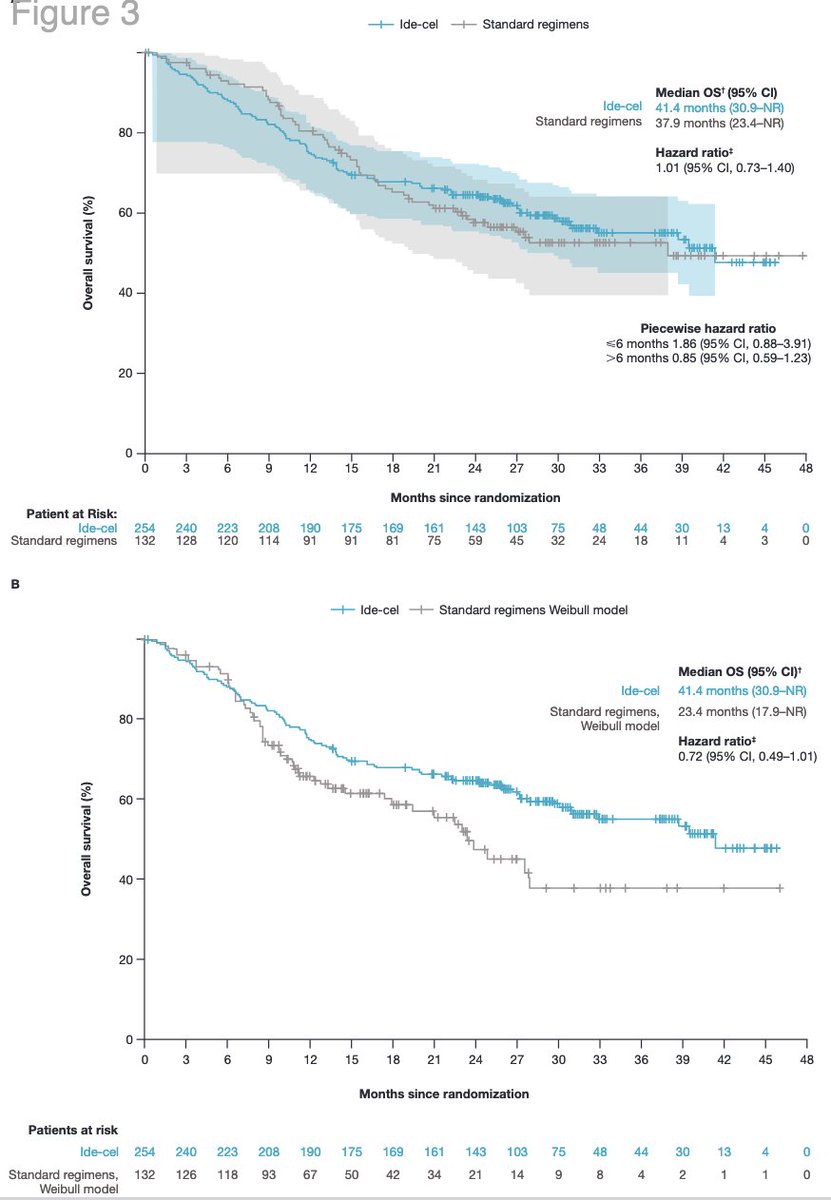
Overall survival data were immature at primary analysis. The first and second interim OS analyses demonstrated an OS detriment in the ide-cel arm for approximately the first 15 months after randomization, attributed to manufacturing delays and early treatment-related deaths. However, crossover-adjusted analyses trended toward ide-cel benefit. The FDA ODAC voted 8-3 that the benefit-risk profile was favorable despite early mortality concerns.
Grade 3/4 adverse events occurred in 93% of ide-cel patients vs 75% with standard regimens. Among 225 ide-cel-treated patients: CRS occurred in 88-91% (Grade >=3 in 4-5%), investigator-identified neurotoxicity in 15% (Grade >=3 in 3%), and broader FDA-defined neurotoxicity in 46% (Grade >=3 in 5-11%). Grade 3/4 cytopenias were frequent: neutropenia 76-79%, anemia 45-51%, thrombocytopenia 42%. Prolonged Grade 3/4 cytopenias beyond Day 30: neutropenia 39%, thrombocytopenia 37%. Infections occurred in 56-58% (Grade 3/4 in 20-24%). Treatment-related Grade 5 events occurred in 3% of ide-cel patients (most commonly sepsis).
KarMMa-3 established ide-cel as the first FDA-approved CAR-T cell therapy for triple-class exposed RRMM after 2+ prior lines of therapy. The approval shifted CAR-T from a last-resort option to an earlier treatment choice in the RRMM journey. Key clinical debates include the early OS detriment driven by manufacturing delays and CAR-T toxicity, competition with Carvykti (cilta-cel, CARTITUDE-4) approved for an overlapping indication, optimal patient selection and timing of CAR-T versus bispecific antibodies, and strategies to reduce manufacturing turnaround time.








