First-line locally advanced or metastatic urothelial carcinoma — Merck Sharp & Dohme
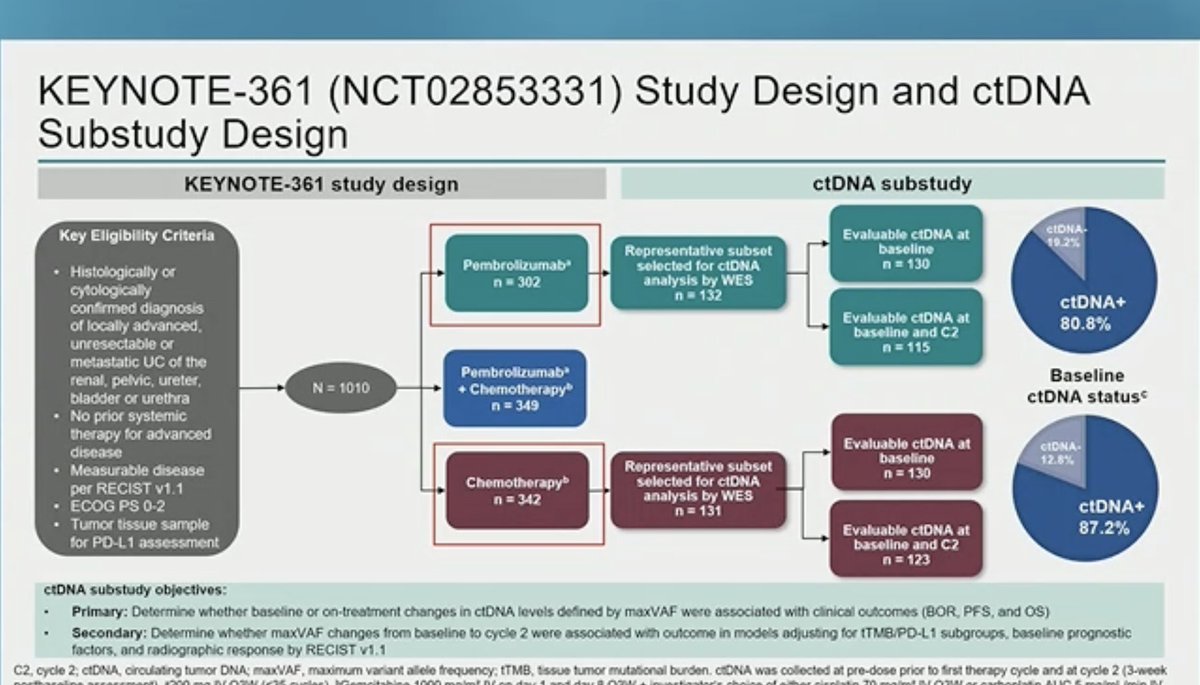
Discover KOL Sentiment on KEYNOTE-361 →Design - Phase 3 first-line pembrolizumab +/- platinum chemotherapy vs chemotherapy alone, locally advanced/metastatic urothelial carcinoma (NCT02853305); dual primary PFS + OS.
PFS (dual primary) - NOT met - median 8.3 vs 7.1 mo, HR 0.78 (95% CI 0.65-0.93), P=0.0033 (did not cross the significance boundary).
OS (dual primary) - NOT met - median 17.0 vs 14.3 mo, HR 0.86 (95% CI 0.72-1.02), P=0.0407.
Safety - Grade >=3 treatment-related AEs 75% (pembro+chemo) vs 17% (pembro monotherapy) vs 72% (chemo); common events anemia, diarrhea, fatigue.
Regulatory - Investigational / negative - no FDA approval from this trial; 1L standard of care has moved to enfortumab vedotin + pembrolizumab (EV-302).
Sponsor / drug - Merck (MSD); pembrolizumab (Keytruda).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.






















Top tweets by impressions — click to view on X
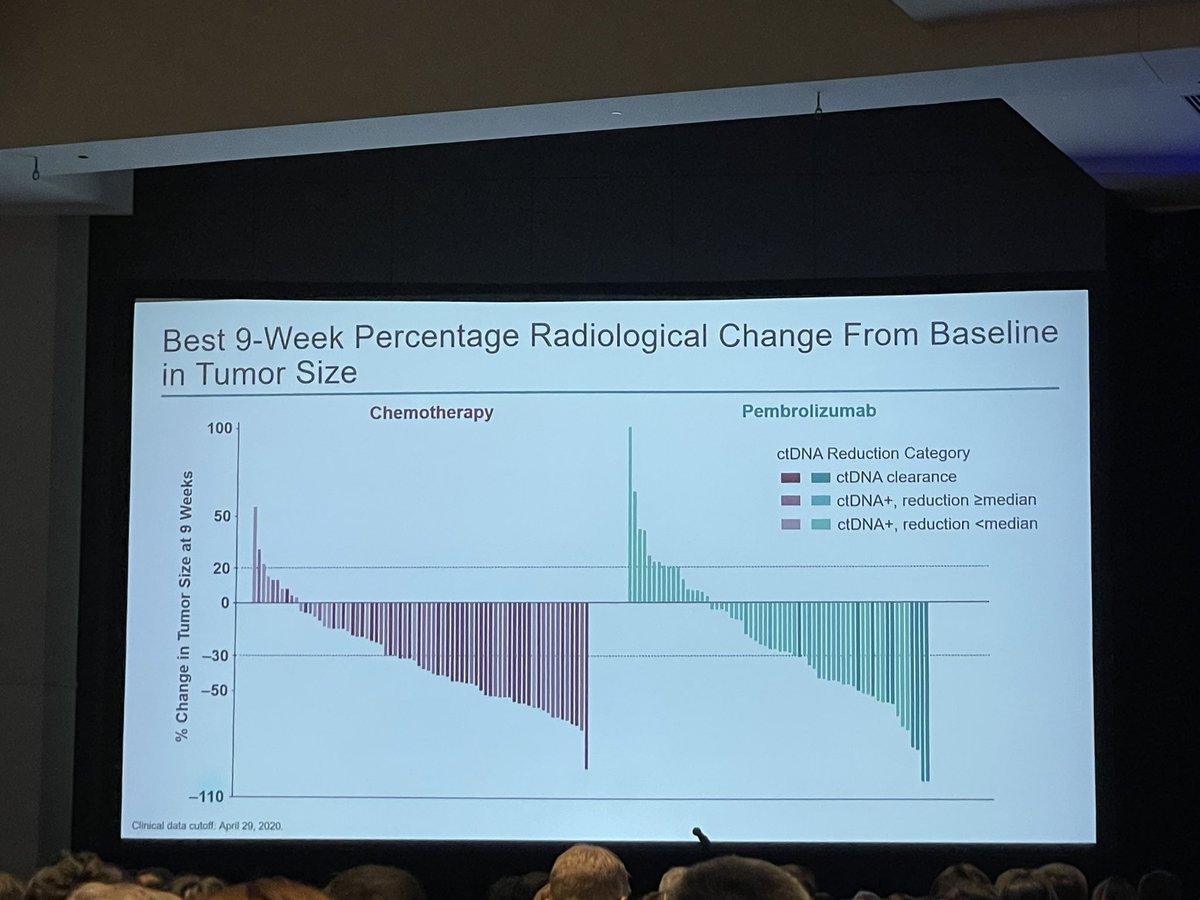
Out in @NatureMedicine today. Treatment is associated with dynamic changes to ctDNA in advanced bladder cancer #ASCO24 . These changes are associated with outcome especially with pembro.…
Excellent talk by @tompowles1 #ASCO24 @ASCO 👉ctDNA data by clinical outcomes with pembro monoRx vs chemo in pts with advanced mUC #bladdercancer from the phase 3 KEYNOTE-361👉 ctDNA levels at…
Now at #ASCO24: In an exploratory analysis of the Keynote-361 phase 3 trial that tested immunotherapy and chemotherapy in advanced urothelial carcinoma, ctDNA levels were associated with response to…
The one and only @tompowles1 presenting data from the #KeyNote361 trial
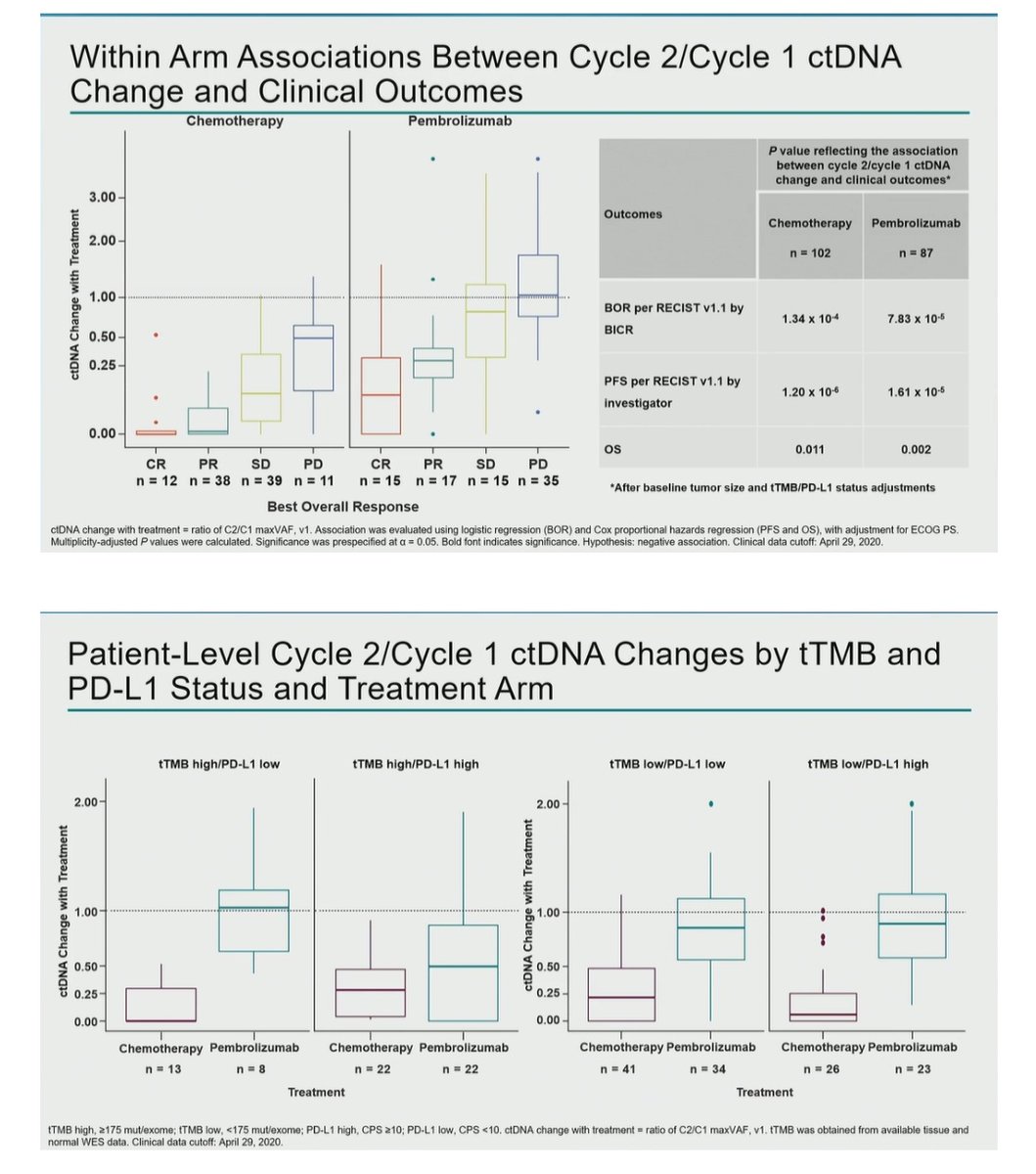
🚨#ctDNA reductions were associated with improved ORR, PFS (P< 0.001), and OS (P< 0.01) in pts with previously untreated…
@tompowles1 with very nice @GuardantHealth ctDNA analysis from #Keynote361 — more ctDNA clearance in chemo treated pts. Would be interesting to see for EV-pembro treated patients! @ASCO #ASCO24…
🧬In the KEYNOTE-361 trial, lower baseline ctDNA levels predicted better outcomes with pembrolizumab in advanced urothelial carcinoma.
🧬ctDNA reductions during treatment correlated with improved…

💫🌟🔥🔝4518: 5Quantitative circulating tumor DNA (ctDNA) assessment in patients (pts) with advanced urothelial carcinoma (UC) treated with pembrolizumab (pembro) or platinum-based chemotherapy (chemo)…
Quantitative ctDNA assessment in patients with advanced #UrothelialCarcinoma treated with pembrolizumab or platinum-based chemotherapy from the phase 3 #KEYNOTE-361 trial. Presented by @tompowles1…

CtDNA in the KEYNOTE 361 study presented by @tompowles1 - higher clearance with chemo but more predictive of response to pembrolizumab. Likely will be an important biomarker in advanced UC…

A review from the FDA was published in #JITC last year to outline regulatory implications of ctDNA in IO for solid tumors. Watch the video abstract here: https://t.co/TDiRp9k5z6. Then make your way…
KEYNOTE-361 failed to show statistically significant PFS or OS benefit for pembrolizumab + platinum-based chemotherapy vs. chemotherapy alone in 1L mUC. The monotherapy arm was not formally tested. Results contributed to the FDA revising the mUC accelerated approval for pembrolizumab monotherapy to the cisplatin-ineligible / platinum-ineligible setting only. Field has since been transformed by EV-302 (enfortumab vedotin + pembrolizumab), which established ADC + IO as the new 1L SOC. KEYNOTE-361 remains a cautionary tale about IO + chemo combinations in urothelial cancer.
Median: 8.3 months (pembrolizumab + chemo, 95% CI 7.5-8.5) vs. 7.1 months (chemotherapy alone, 95% CI 6.4-7.9). HR 0.78 (95% CI 0.65-0.93), P=0.0033 Neither primary endpoint met pre-specified statistical significance boundary. PFS: median 8.3 vs. 7.1 months, HR 0.78 (95% CI 0.65-0.93, P=0.0033) — did NOT meet P=0.0019 significance boundary. OS: median 17.0 vs. 14.3 months, HR 0.86 (95% CI 0.72-1.02, P=0.0407) — did NOT meet P=0.0142 boundary. Pembrolizumab monotherapy arm not formally tested per hierarchical statistical plan. Exploratory monotherapy OS: 15.6 vs. 14.3 months, HR 0.92 (95% CI 0.77-1.11). Median follow-up 31.7 months.
Median: 17.0 months (pembrolizumab + chemo, 95% CI 14.5-19.5) vs. 14.3 months (chemotherapy alone, 95% CI 12.3-16.7). HR 0.86 (95% CI 0.72-1.02), P=0.0407 OS was a dual primary endpoint (see above); not met.
Grade ≥3 adverse events: 75% (pembro_chemo) vs. 17% (pembro_mono) vs. 72% (chemo). Key AEs: anemia (30% pembro+chemo; 33% chemo), pneumonitis (1% pembro mono), diarrhea, fatigue, hyponatremia (1% pembro mono). Treatment-related Grade ≥3 AEs: 75% (pembro+chemo), 17% (pembro monotherapy), 72% (chemo). Treatment-related serious AEs: 31% / 16% / 18%. Discontinuation of any component: 31% / 16% / 18%. Safety profile consistent with prior studies; no new safety signals.
❌ Historical negative trial; 1L urothelial SOC has since moved to EV-302 (enfortumab + pembrolizumab). KEYNOTE-361 failed to show statistically significant PFS or OS benefit for pembrolizumab + platinum-based chemotherapy vs. chemotherapy alone in 1L mUC. The monotherapy arm was not formally tested. Results contributed to the FDA revising the mUC accelerated approval for pembrolizumab monotherapy to the cisplatin-ineligible / platinum-ineligible setting only. Field has since been transformed by EV-302 (enfortumab vedotin + pembrolizumab), which established ADC + IO as the new 1L SOC. KEYNOTE-361 remains a cautionary tale about IO + chemo combinations in urothelial cancer.
KEYNOTE-361 is a Phase 3 randomized trial (NCT02853305) of first-line pembrolizumab (Keytruda) with or without platinum-based chemotherapy versus chemotherapy alone in patients with locally advanced or metastatic urothelial carcinoma. Progression-free survival and overall survival were dual primary endpoints.
No. KEYNOTE-361 was a negative trial. Neither dual primary endpoint crossed the pre-specified statistical significance boundary: progression-free survival was 8.3 versus 7.1 months (HR 0.78; 95% CI 0.65-0.93; P=0.0033) and overall survival was 17.0 versus 14.3 months (HR 0.86; 95% CI 0.72-1.02; P=0.0407) for pembrolizumab plus chemotherapy versus chemotherapy alone.
No. Because both primary endpoints failed to reach statistical significance, KEYNOTE-361 did not result in an FDA approval for first-line pembrolizumab plus chemotherapy in urothelial carcinoma. Pembrolizumab (Keytruda) remains FDA approved in many other cancer settings, but this specific first-line combination was not established by this trial.
First-line standard of care has since moved to enfortumab vedotin plus pembrolizumab (based on EV-302), which showed a substantial overall survival benefit regardless of cisplatin eligibility. KEYNOTE-361 is now regarded as a historical negative trial that did not change practice.
Grade 3 or higher treatment-related adverse events occurred in about 75% of the pembrolizumab-plus-chemotherapy arm, 17% of the pembrolizumab-monotherapy arm, and 72% of the chemotherapy arm. Common events included anemia, diarrhea, and fatigue, with pneumonitis and hyponatremia seen in a small percentage of the monotherapy arm - consistent with the known profiles of chemotherapy and checkpoint inhibition.