Locally advanced or metastatic NSCLC without actionable genomic alterations, post-platinum chemo + anti-PD-(L)1 — AstraZeneca
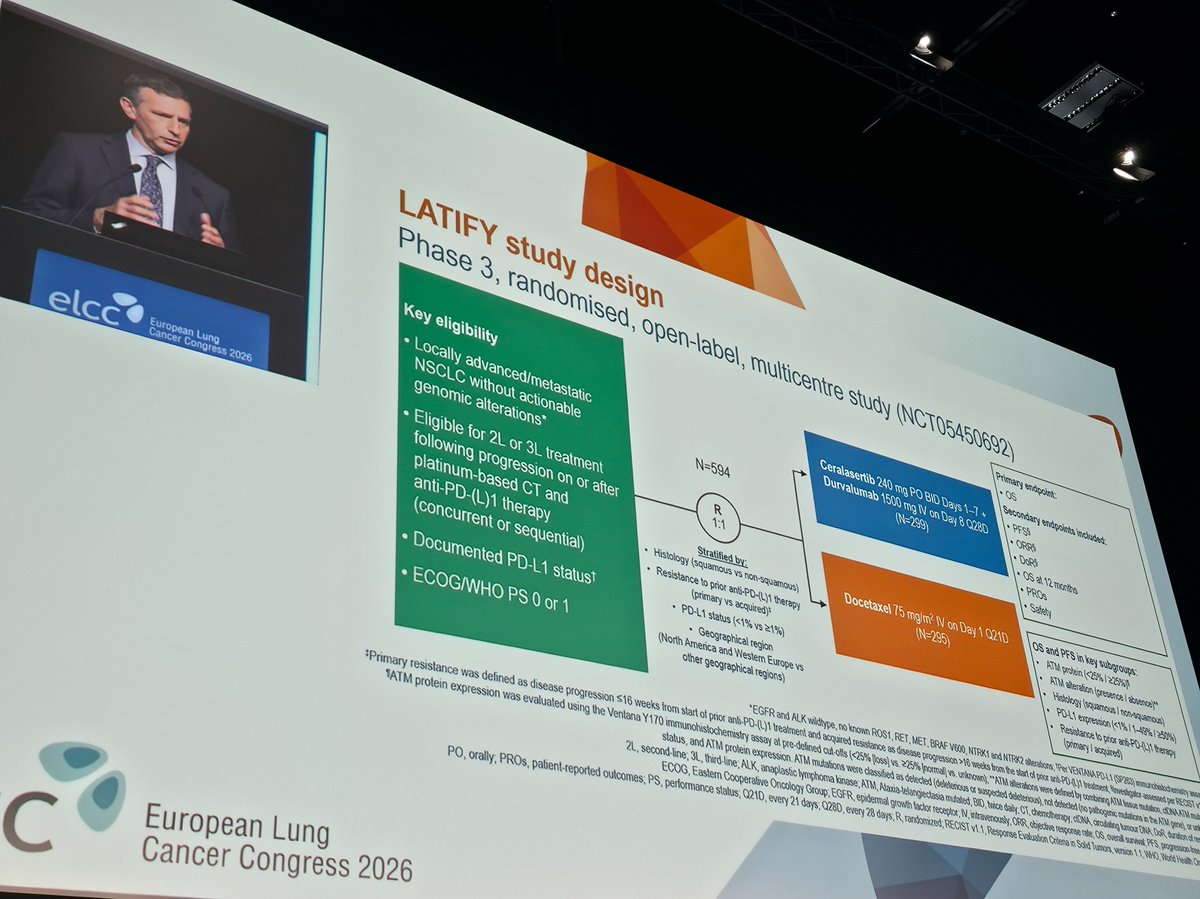
Discover KOL Sentiment on LATIFY →Design - Phase 3 open-label randomized global trial (~594 patients, 1:1) of ceralasertib (investigational ATR inhibitor, 240 mg BID x7 days) + durvalumab (Imfinzi, 1500 mg Q4W) vs docetaxel in post-IO + platinum advanced NSCLC without actionable alterations (NCT05450692; AstraZeneca).
Overall survival (primary, NOT MET) - The trial FAILED its primary overall-survival endpoint; ceralasertib + durvalumab did not improve OS versus docetaxel (AstraZeneca press release, December 22, 2025).
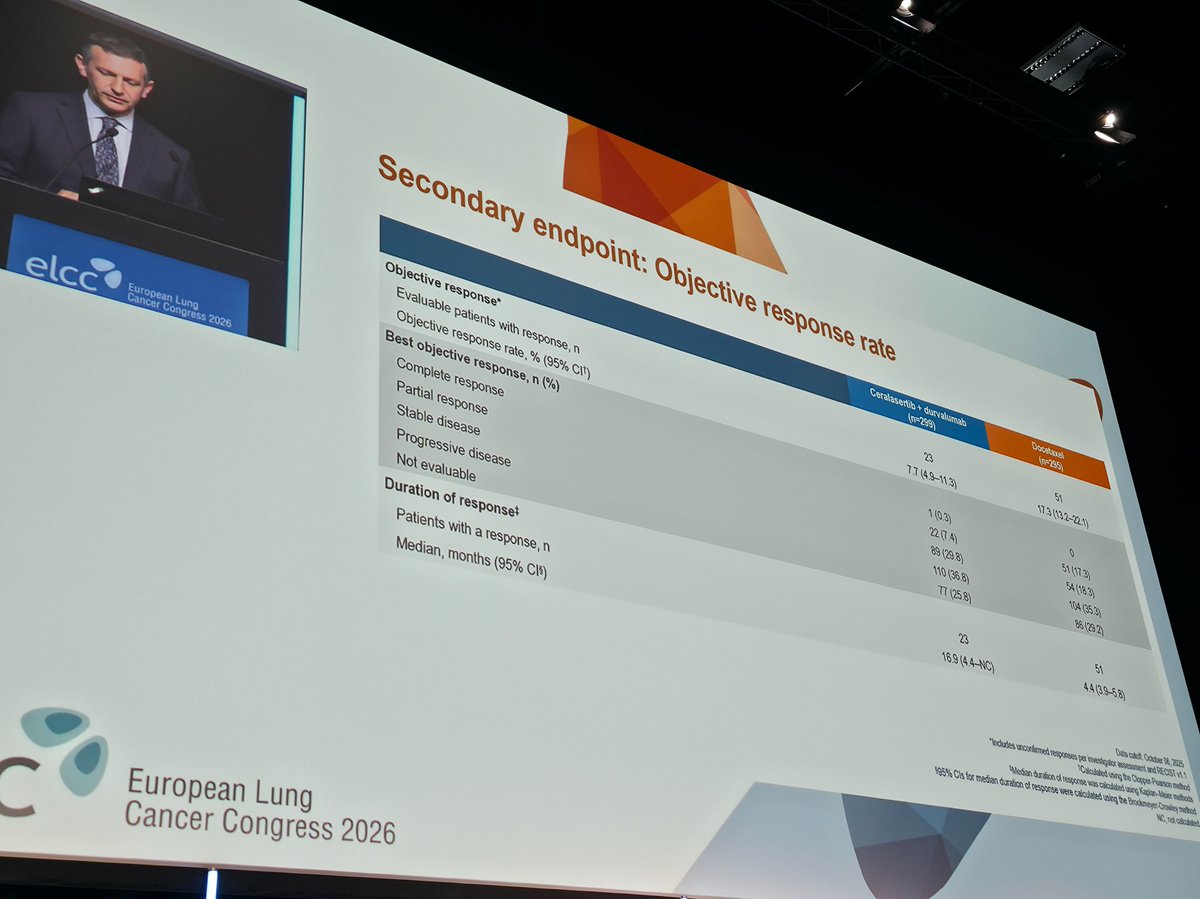
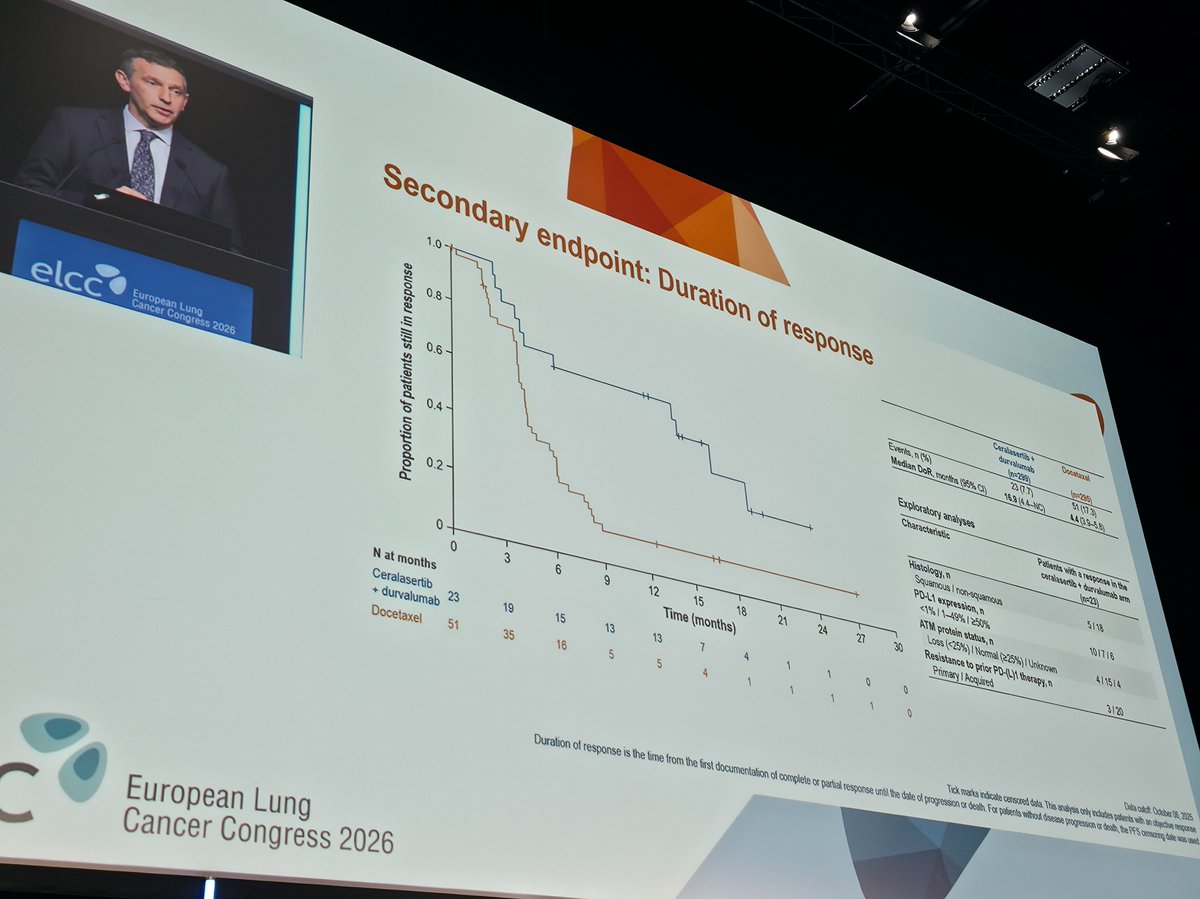
Secondary endpoints - Detailed PFS, ORR, DoR and other secondary results are pending presentation at a medical meeting.
Safety - The combination was generally well tolerated with a safety profile consistent with the known profiles of durvalumab and ceralasertib; no new safety signals were identified.
Regulatory / sponsor - Investigational and negative; ceralasertib is not FDA approved. Sponsor AstraZeneca.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.











Top tweets by impressions — click to view on X
🔜 #ELCC26 @myESMO 🇩🇰
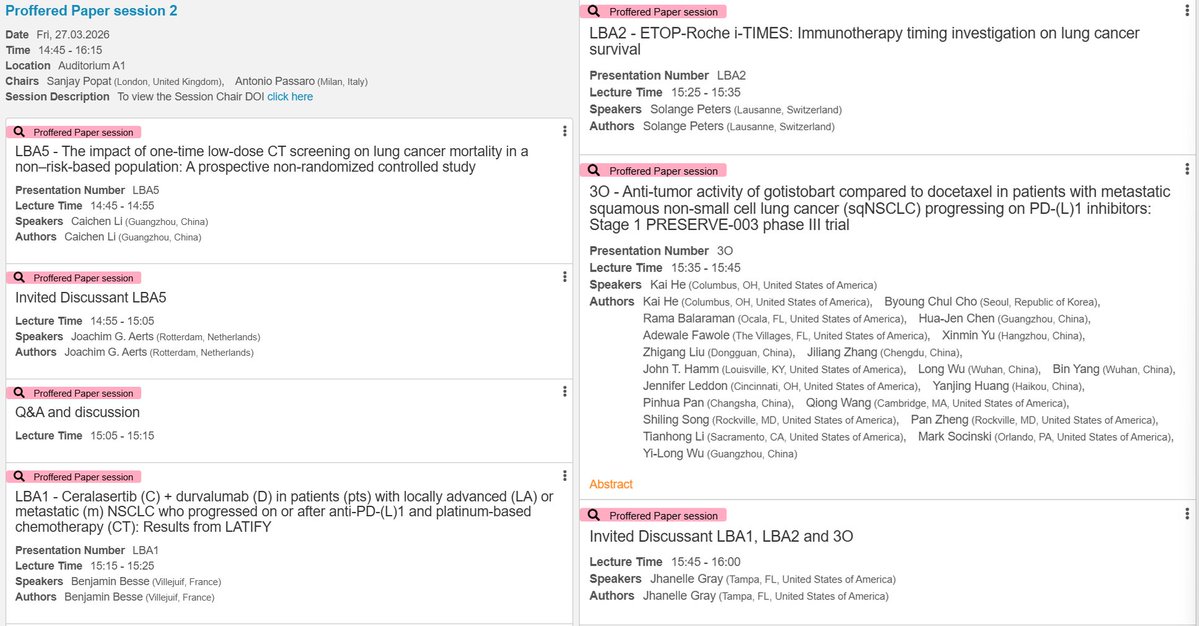
🔥Proffered Paper session 2
☑️CT screening in non-risk-based population
☑️LATIFY: ceralasertib + durvalumab
☑️ETOP-Roche i-TIMES: immunotherapy timing
☑️PRESERVE-003: gotistobart…
Post-#ELCC26 clarity in one place 😉
🔗 https://t.co/BkY68N7Kjp
From KRAS G12D degraders to ADC final OS, plus negative trials that matter (LATIFY) and practice-changing questions (i-TIMES, NorthStar)…
Superb presentation by @BenjaminBesseMD on the results of the Phase III LATIFY study. Unfortunately, the trial was negative, despite a potential benefit in 7% of patients who require molecular…
🆙 #ELCC26 @myESMO 🇩🇰
🔥Proffered Paper session 2
☑️LATIFY: ceralasertib + durvalumab
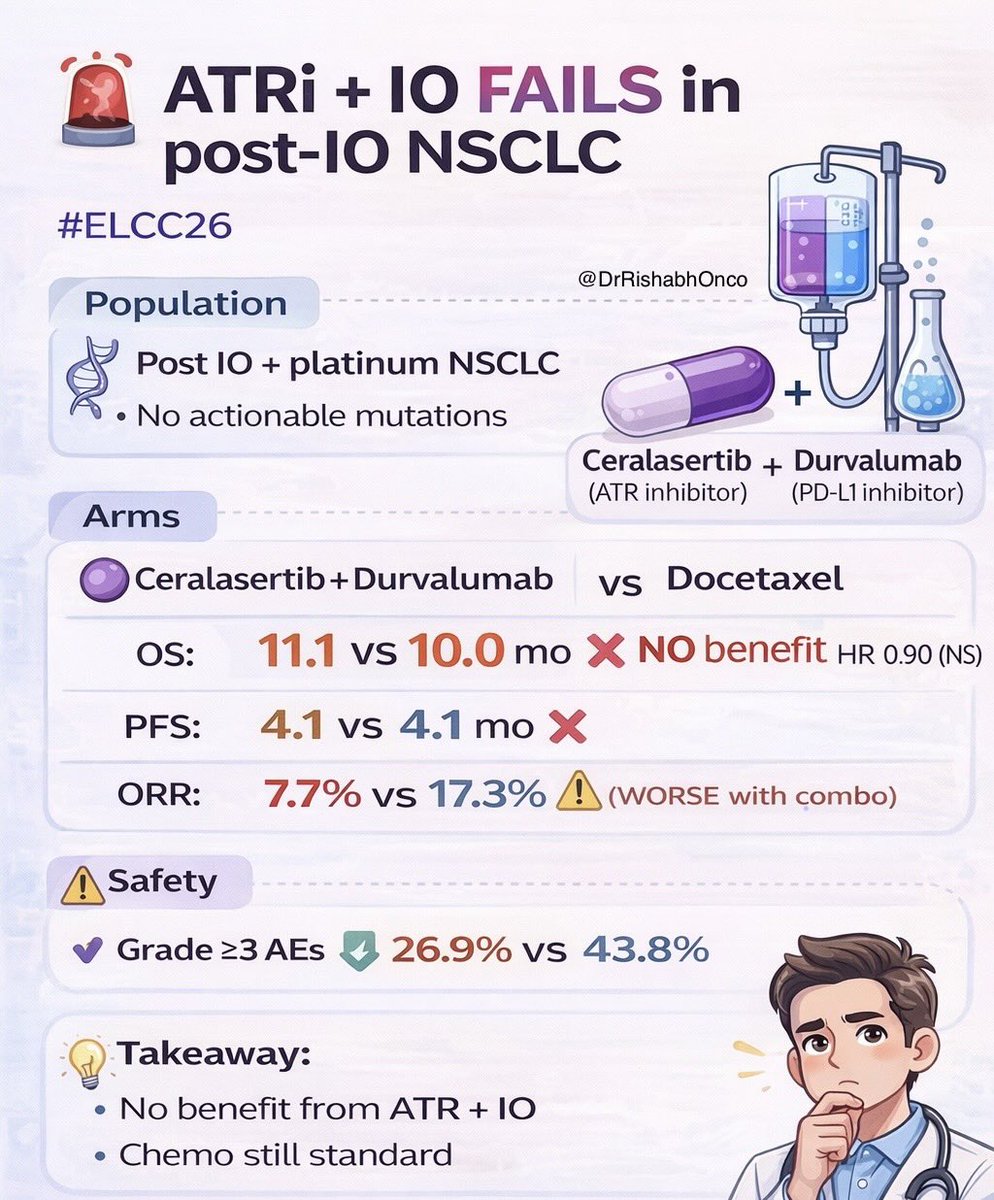
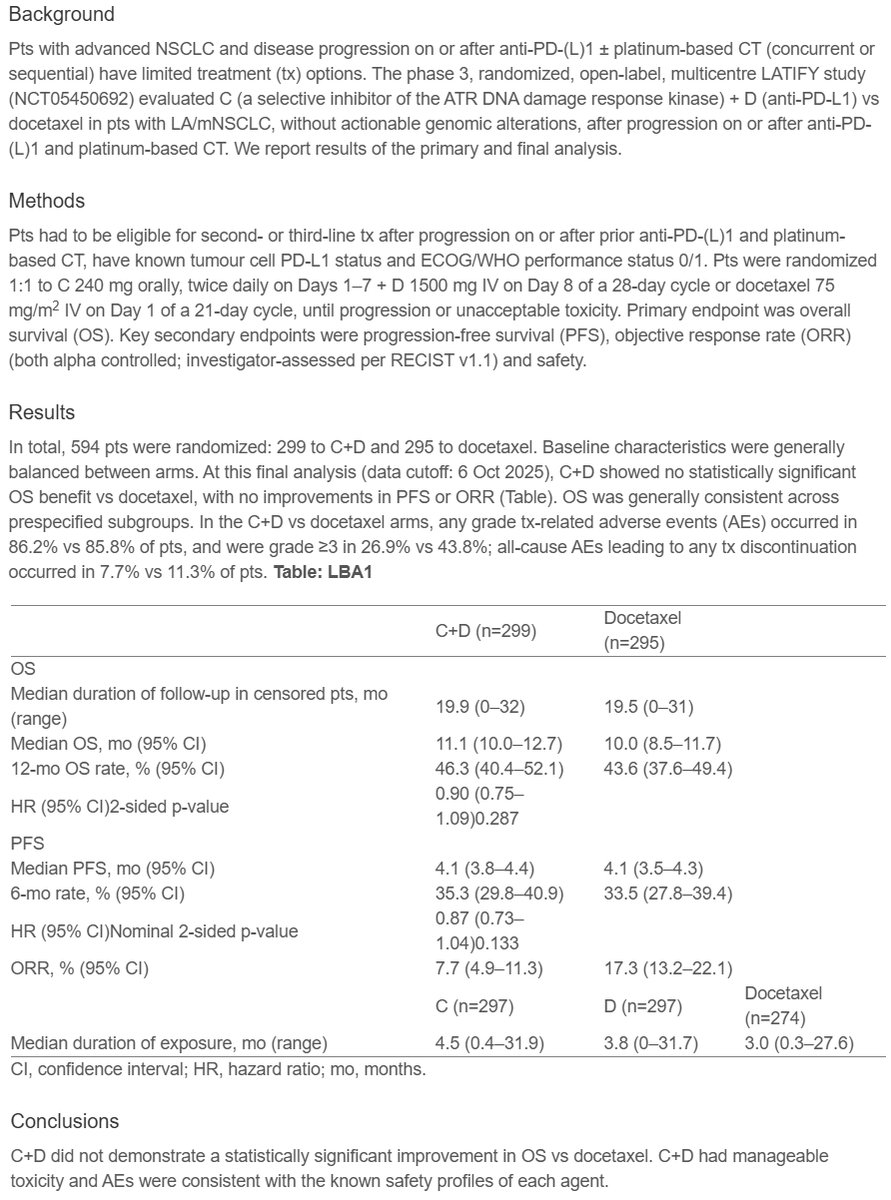
🎯No statistically significant OS benefit vs docetaxel, with no improvements in PFS or ORR
🎙️…
🆙 #ELCC26 @myESMO @IASLC 🇩🇰
🔥Proffered Paper session 2
☑️LATIFY: ceralasertib + durvalumab
🎯No statistically significant OS benefit vs docetaxel, with no improvements in PFS or ORR
🎙️…
🚨 ATR inhibition + IO fails to beat chemo in post-IO NSCLC #ELCC26
LATIFY trial: Ceralasertib + Durvalumab vs docetaxel 👇
🧬 Study population
• LA/mNSCLC
• Progressed after anti-PD-(L)1 ± platinum…
Conclusion in one Line
The LATIFY Trial is Negative for all outcomes . @esmo #elcc26 https://t.co/Xd8pdCHpYF
Disappointing to see that the LATIFY trial didn't meet it's primary endpoint!
But there are patients who do benefit from PD(L)1 rechallenge in the second line as highlighted by @BenjaminBesseMD…

@myESMO #ELCC26: Top Trials from Day 3
SHR-A2009-201 | KEYNOTE-671 | LATIFY | OptiTROP-Lung03 | NCT04938804 | NCT06107686 | PRESERVE-003 | NCT06505837
#ELCC #ELCC2026 #Cancer #Oncology #LungCancer…
LATIFY is a high-profile Phase 3 failure for AstraZeneca's ATR kinase inhibitor ceralasertib in combination with durvalumab in previously treated advanced NSCLC without actionable genomic alterations. Trial missed OS primary endpoint vs. docetaxel (SOC). Well-tolerated with no new safety signals but efficacy signal did not translate. Analyst perspective (Biswajit Podder, GlobalData): 'narrows ATR's role to biomarker-selected subsets'. The trial design was criticized for not evaluating each therapy as monotherapy, limiting attribution of benefit to ATR inhibition specifically. Post-IO NSCLC treatment remains a high unmet need; docetaxel + ramucirumab or chemo ± bevacizumab remain default; emerging agents (SG, BL-B01D1, Dato-DXd) under investigation.
Phase 3 randomized open-label global trial, ~594 patients across 20+ countries, randomized 1:1. Experimental: ceralasertib 240mg BID x 7 days + durvalumab 1500mg fixed dose Q4W on day 8. Control: docetaxel Q3W. Trial FAILED primary endpoint of OS — ceralasertib + durvalumab did NOT improve OS vs. docetaxel. Specific HR, 95% CI, and P-value NOT disclosed in AstraZeneca press release. Detailed results to be presented at upcoming medical meeting. AstraZeneca statement: 'We remain committed to pioneering new medicines...' — disappointment.
OS was the primary endpoint (see above). Detailed results pending medical meeting presentation. Secondary endpoints (PFS, ORR, DoR, TTR, DCR, TTSPD, 12-mo OS, HRQoL time-to-deterioration) also pending. Analyst commentary suggests ATR inhibition may retain role in biomarker-selected subsets but not unselected post-IO NSCLC.
Combination was generally well tolerated. Safety profile consistent with known profiles of each individual agent (durvalumab + ceralasertib). No new safety signals identified per AstraZeneca press release.
❌ Negative Phase 3: Ceralasertib + durvalumab does not improve OS in post-IO NSCLC vs. docetaxel. LATIFY is a high-profile Phase 3 failure for AstraZeneca's ATR kinase inhibitor ceralasertib in combination with durvalumab in previously treated advanced NSCLC without actionable genomic alterations. Trial missed OS primary endpoint vs. docetaxel (SOC). Well-tolerated with no new safety signals but efficacy signal did not translate. Analyst perspective (Biswajit Podder, GlobalData): 'narrows ATR's role to biomarker-selected subsets'. The trial design was criticized for not evaluating each therapy as monotherapy, limiting attribution of benefit to ATR inhibition specifically. Post-IO NSCLC treatment remains a high unmet need; docetaxel + ramucirumab or chemo ± bevacizumab remain default; emerging agents (SG, BL-B01D1, Dato-DXd) under investigation.
LATIFY (NCT05450692) is a Phase 3, AstraZeneca-sponsored, open-label randomized global trial of about 594 patients that compared the investigational ATR kinase inhibitor ceralasertib plus durvalumab (Imfinzi) against docetaxel in patients with locally advanced or metastatic non-small cell lung cancer without actionable genomic alterations, after progression on platinum chemotherapy and anti-PD-(L)1 immunotherapy.
LATIFY did not meet its primary endpoint. According to AstraZeneca's December 22, 2025 announcement, ceralasertib plus durvalumab did not improve overall survival compared with docetaxel in this previously treated NSCLC population. The combination was generally well tolerated, but detailed efficacy results are pending a medical-meeting presentation.
No. Ceralasertib is an investigational ATR (ataxia telangiectasia and Rad3-related) kinase inhibitor and is not FDA approved for any indication. Durvalumab (Imfinzi) is separately approved in other settings, but the ceralasertib-durvalumab combination tested in LATIFY is not FDA approved and did not meet its primary endpoint.
AstraZeneca reported that the ceralasertib-durvalumab combination was generally well tolerated, with a safety profile consistent with the known profiles of each individual agent and no new safety signals identified. Full safety details are expected at a future medical meeting.
LATIFY is a high-profile Phase 3 failure for AstraZeneca's ATR inhibitor ceralasertib in combination with durvalumab in previously treated NSCLC. The negative overall-survival result is an important data point for the ATR-inhibitor field and for strategies attempting to re-sensitize immunotherapy-pretreated patients, underscoring how difficult the post-IO, post-platinum setting remains.