Locally advanced or metastatic NSCLC without actionable genomic alterations, post-platinum chemo + anti-PD-(L)1 — AstraZeneca
Visit Interactive Trial Page →










Top tweets by impressions — click to view on X
🔜 #ELCC26 @myESMO 🇩🇰
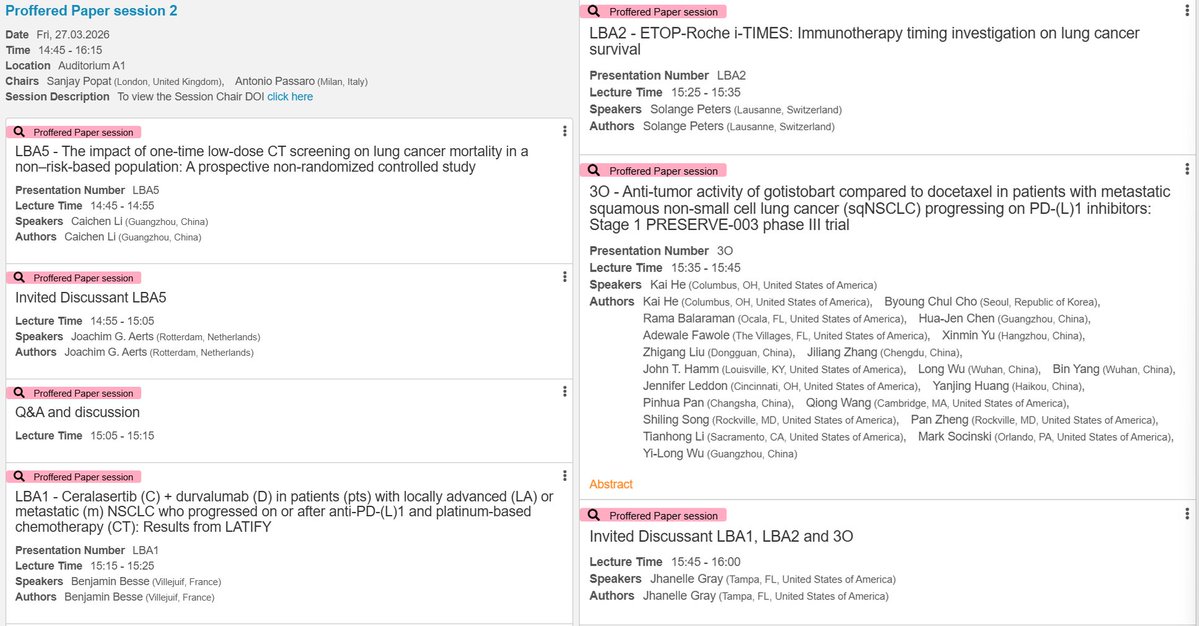
🔥Proffered Paper session 2
☑️CT screening in non-risk-based population
☑️LATIFY: ceralasertib + durvalumab
☑️ETOP-Roche i-TIMES: immunotherapy timing
☑️PRESERVE-003: gotistobart…
Post-#ELCC26 clarity in one place 😉
🔗 https://t.co/BkY68N7Kjp
From KRAS G12D degraders to ADC final OS, plus negative trials that matter (LATIFY) and practice-changing questions (i-TIMES, NorthStar)…
Superb presentation by @BenjaminBesseMD on the results of the Phase III LATIFY study. Unfortunately, the trial was negative, despite a potential benefit in 7% of patients who require molecular…
🆙 #ELCC26 @myESMO 🇩🇰
🔥Proffered Paper session 2
☑️LATIFY: ceralasertib + durvalumab
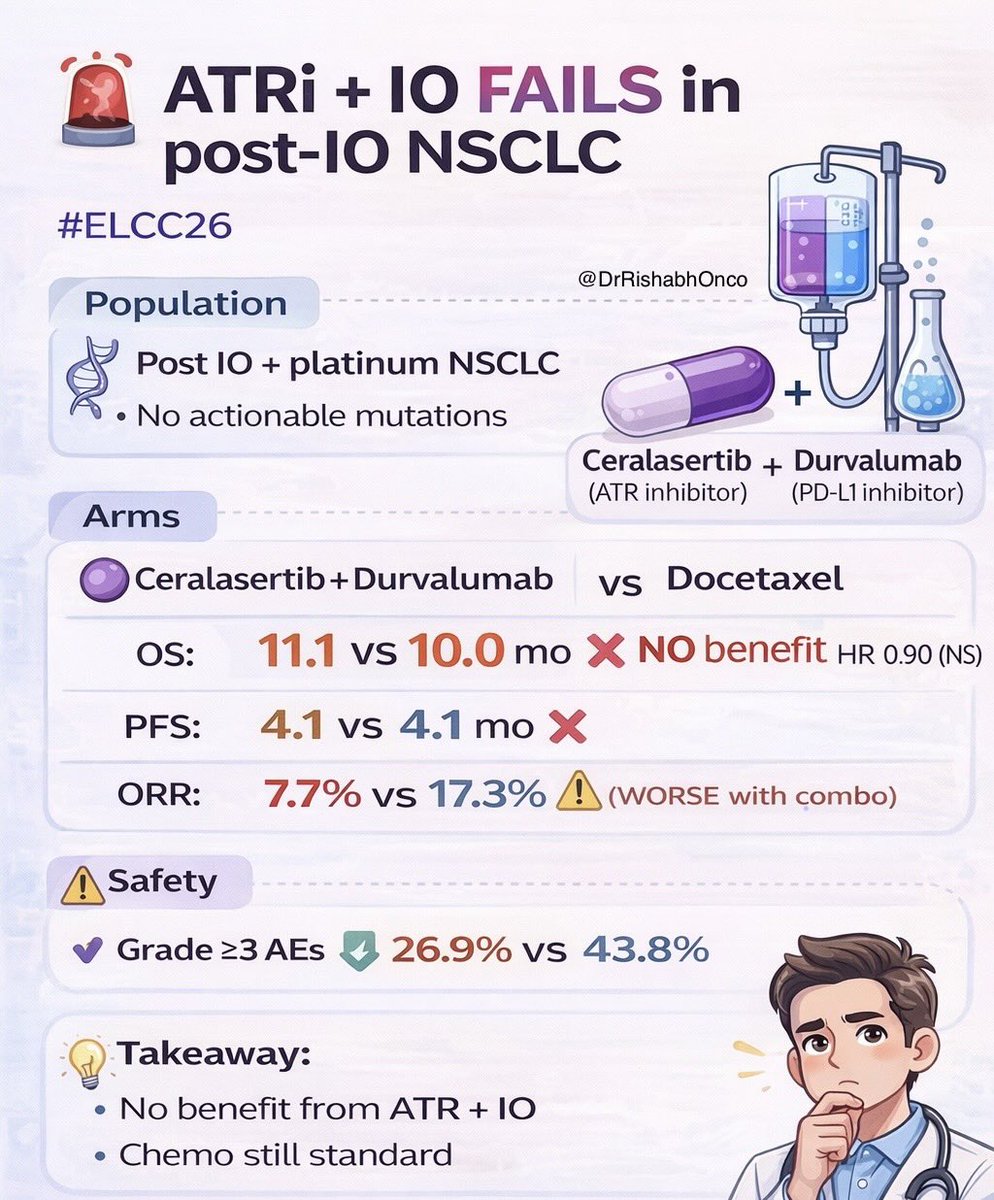
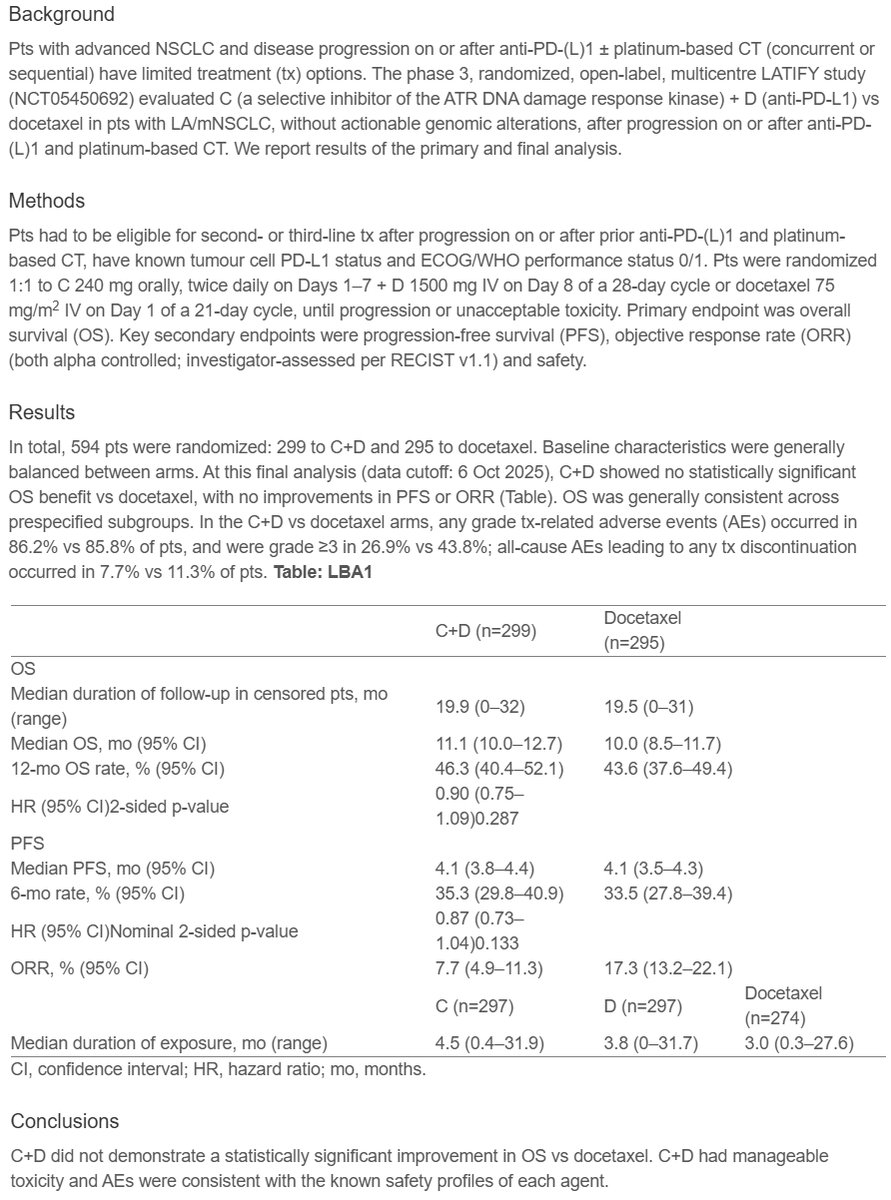
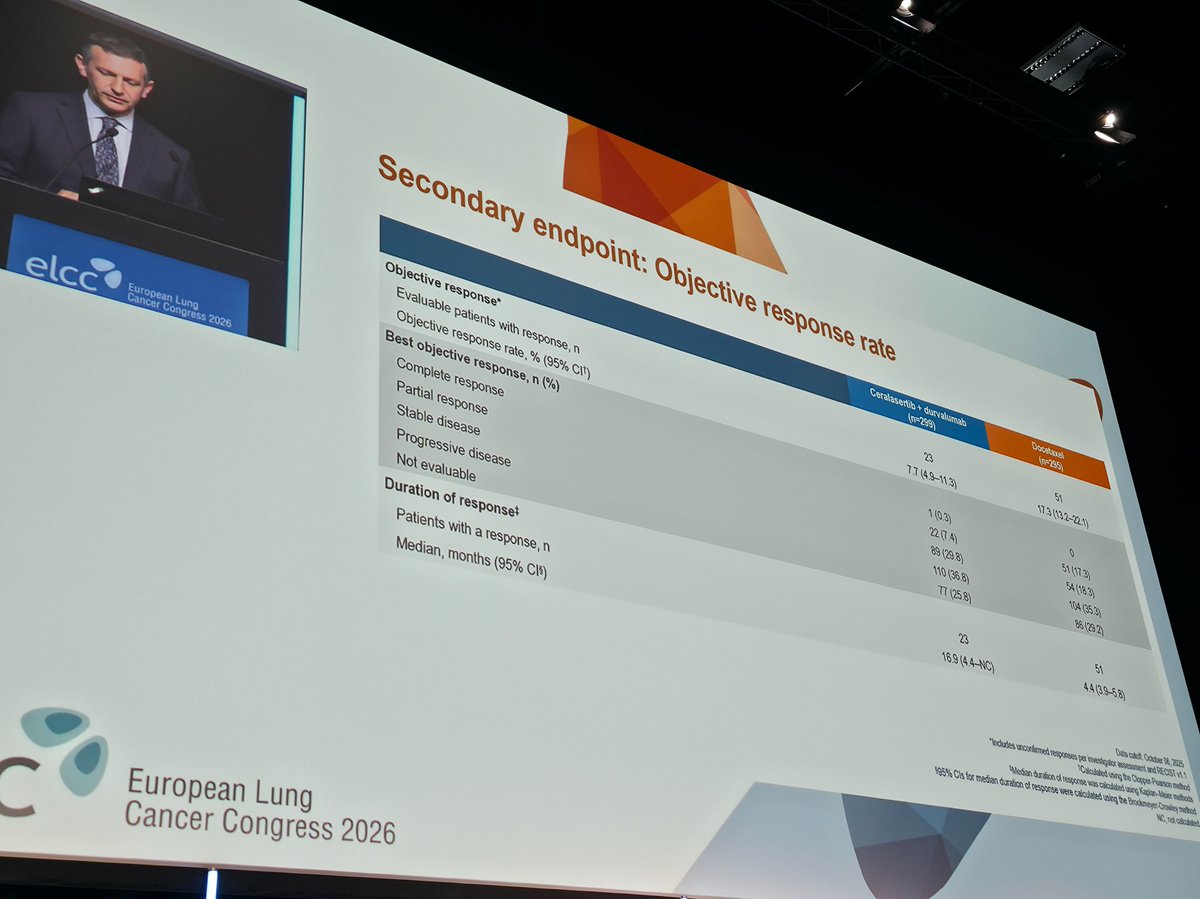
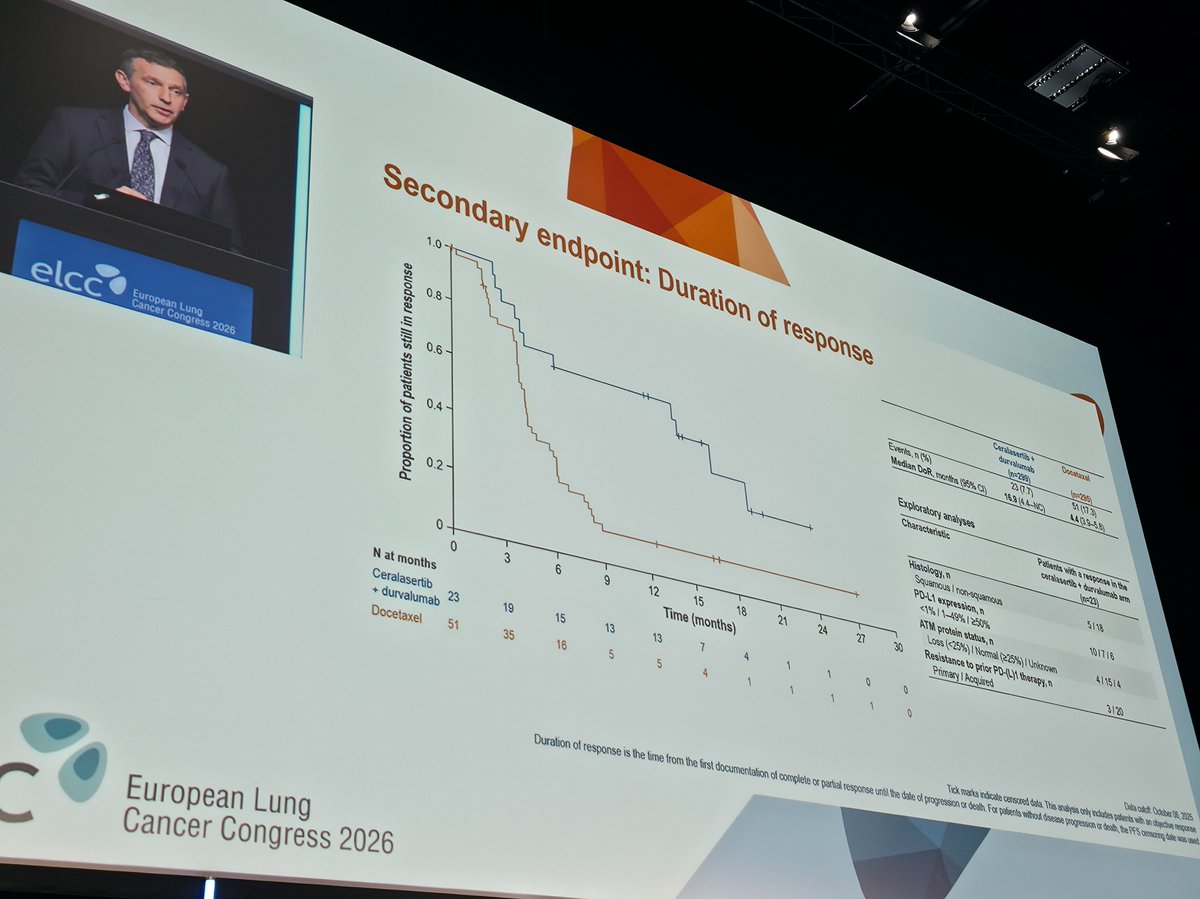
🎯No statistically significant OS benefit vs docetaxel, with no improvements in PFS or ORR
🎙️…
🆙 #ELCC26 @myESMO @IASLC 🇩🇰
🔥Proffered Paper session 2
☑️LATIFY: ceralasertib + durvalumab
🎯No statistically significant OS benefit vs docetaxel, with no improvements in PFS or ORR
🎙️…
🚨 ATR inhibition + IO fails to beat chemo in post-IO NSCLC #ELCC26
LATIFY trial: Ceralasertib + Durvalumab vs docetaxel 👇
🧬 Study population
• LA/mNSCLC
• Progressed after anti-PD-(L)1 ± platinum…
Conclusion in one Line
The LATIFY Trial is Negative for all outcomes . @esmo #elcc26 https://t.co/Xd8pdCHpYF
Disappointing to see that the LATIFY trial didn't meet it's primary endpoint!
But there are patients who do benefit from PD(L)1 rechallenge in the second line as highlighted by @BenjaminBesseMD…

@myESMO #ELCC26: Top Trials from Day 3
SHR-A2009-201 | KEYNOTE-671 | LATIFY | OptiTROP-Lung03 | NCT04938804 | NCT06107686 | PRESERVE-003 | NCT06505837
#ELCC #ELCC2026 #Cancer #Oncology #LungCancer…
LATIFY is a high-profile Phase 3 failure for AstraZeneca's ATR kinase inhibitor ceralasertib in combination with durvalumab in previously treated advanced NSCLC without actionable genomic alterations. Trial missed OS primary endpoint vs. docetaxel (SOC). Well-tolerated with no new safety signals but efficacy signal did not translate. Analyst perspective (Biswajit Podder, GlobalData): 'narrows ATR's role to biomarker-selected subsets'. The trial design was criticized for not evaluating each therapy as monotherapy, limiting attribution of benefit to ATR inhibition specifically. Post-IO NSCLC treatment remains a high unmet need; docetaxel + ramucirumab or chemo ± bevacizumab remain default; emerging agents (SG, BL-B01D1, Dato-DXd) under investigation.
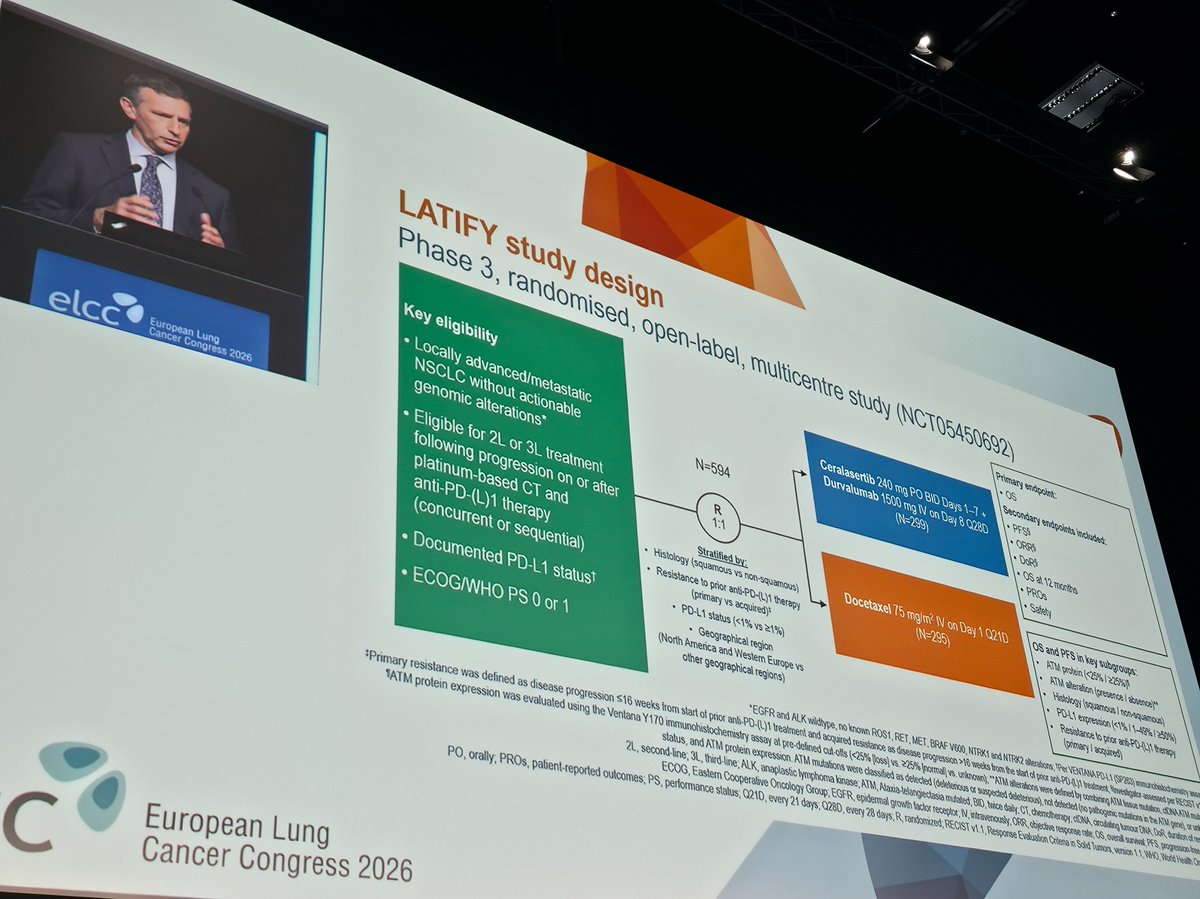
Phase 3 randomized open-label global trial, ~594 patients across 20+ countries, randomized 1:1. Experimental: ceralasertib 240mg BID x 7 days + durvalumab 1500mg fixed dose Q4W on day 8. Control: docetaxel Q3W. Trial FAILED primary endpoint of OS — ceralasertib + durvalumab did NOT improve OS vs. docetaxel. Specific HR, 95% CI, and P-value NOT disclosed in AstraZeneca press release. Detailed results to be presented at upcoming medical meeting. AstraZeneca statement: 'We remain committed to pioneering new medicines...' — disappointment.
OS was the primary endpoint (see above). Detailed results pending medical meeting presentation. Secondary endpoints (PFS, ORR, DoR, TTR, DCR, TTSPD, 12-mo OS, HRQoL time-to-deterioration) also pending. Analyst commentary suggests ATR inhibition may retain role in biomarker-selected subsets but not unselected post-IO NSCLC.
Combination was generally well tolerated. Safety profile consistent with known profiles of each individual agent (durvalumab + ceralasertib). No new safety signals identified per AstraZeneca press release.
❌ Negative Phase 3: Ceralasertib + durvalumab does not improve OS in post-IO NSCLC vs. docetaxel. LATIFY is a high-profile Phase 3 failure for AstraZeneca's ATR kinase inhibitor ceralasertib in combination with durvalumab in previously treated advanced NSCLC without actionable genomic alterations. Trial missed OS primary endpoint vs. docetaxel (SOC). Well-tolerated with no new safety signals but efficacy signal did not translate. Analyst perspective (Biswajit Podder, GlobalData): 'narrows ATR's role to biomarker-selected subsets'. The trial design was criticized for not evaluating each therapy as monotherapy, limiting attribution of benefit to ATR inhibition specifically. Post-IO NSCLC treatment remains a high unmet need; docetaxel + ramucirumab or chemo ± bevacizumab remain default; emerging agents (SG, BL-B01D1, Dato-DXd) under investigation.