EGFR-mutant locally advanced or metastatic NSCLC, non-progressing after osimertinib induction — MD Anderson Cancer Center (academic investigator-initiated)
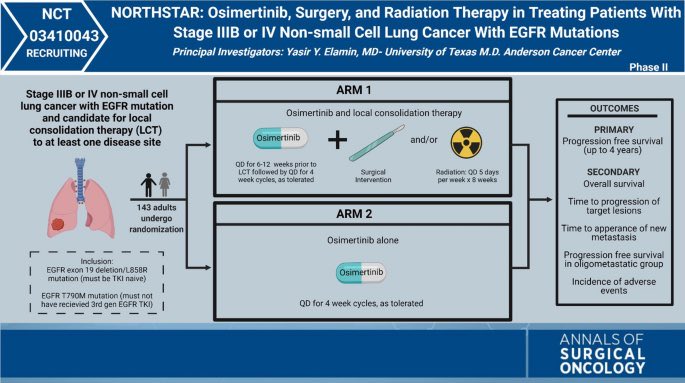
Discover KOL Sentiment on NorthStar →Design - Randomized Phase 2 investigator-initiated trial: osimertinib (Tagrisso) +/- local consolidative therapy (surgery and/or radiotherapy) in EGFR-mutant advanced NSCLC non-progressing after osimertinib induction (NCT03410043; MD Anderson).
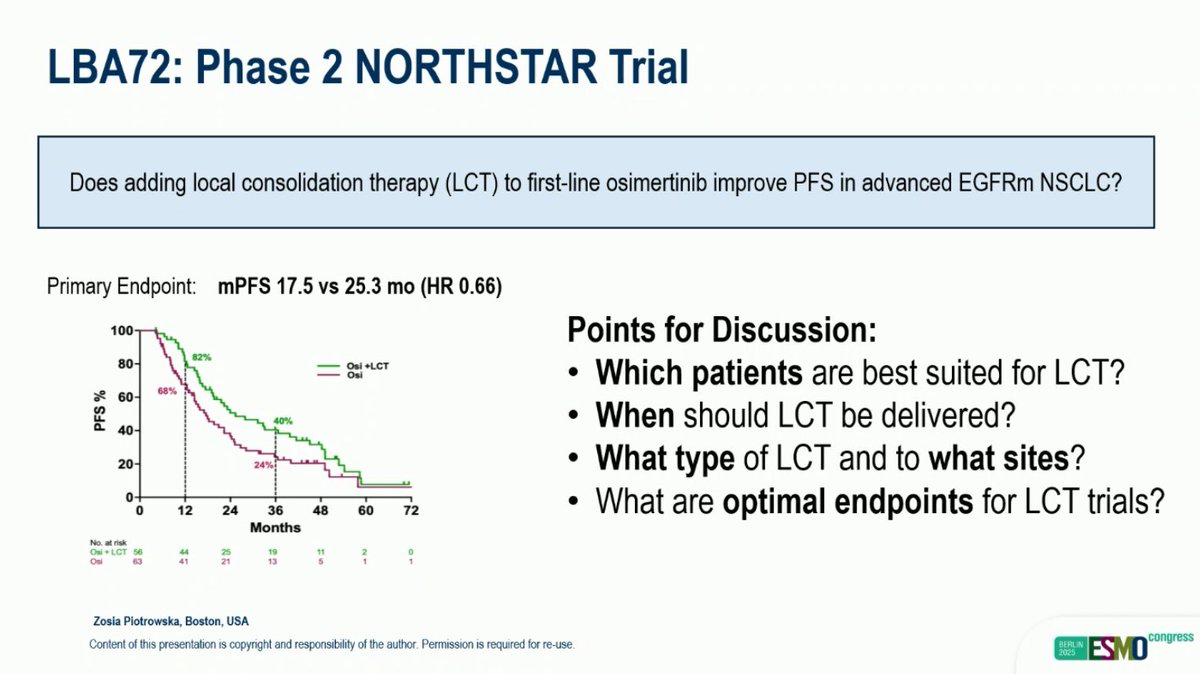
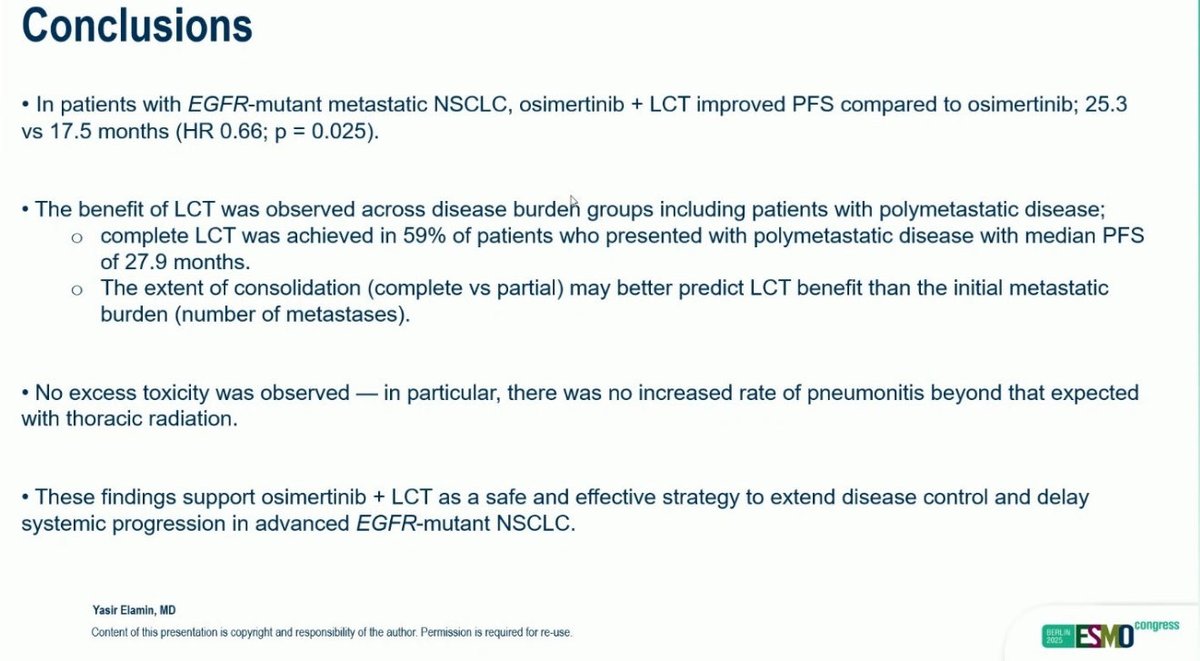
PFS (primary) - Median 25.3 vs 17.5 months, HR 0.66, P=0.025 favoring osimertinib plus local consolidative therapy - a 7.8-month improvement.
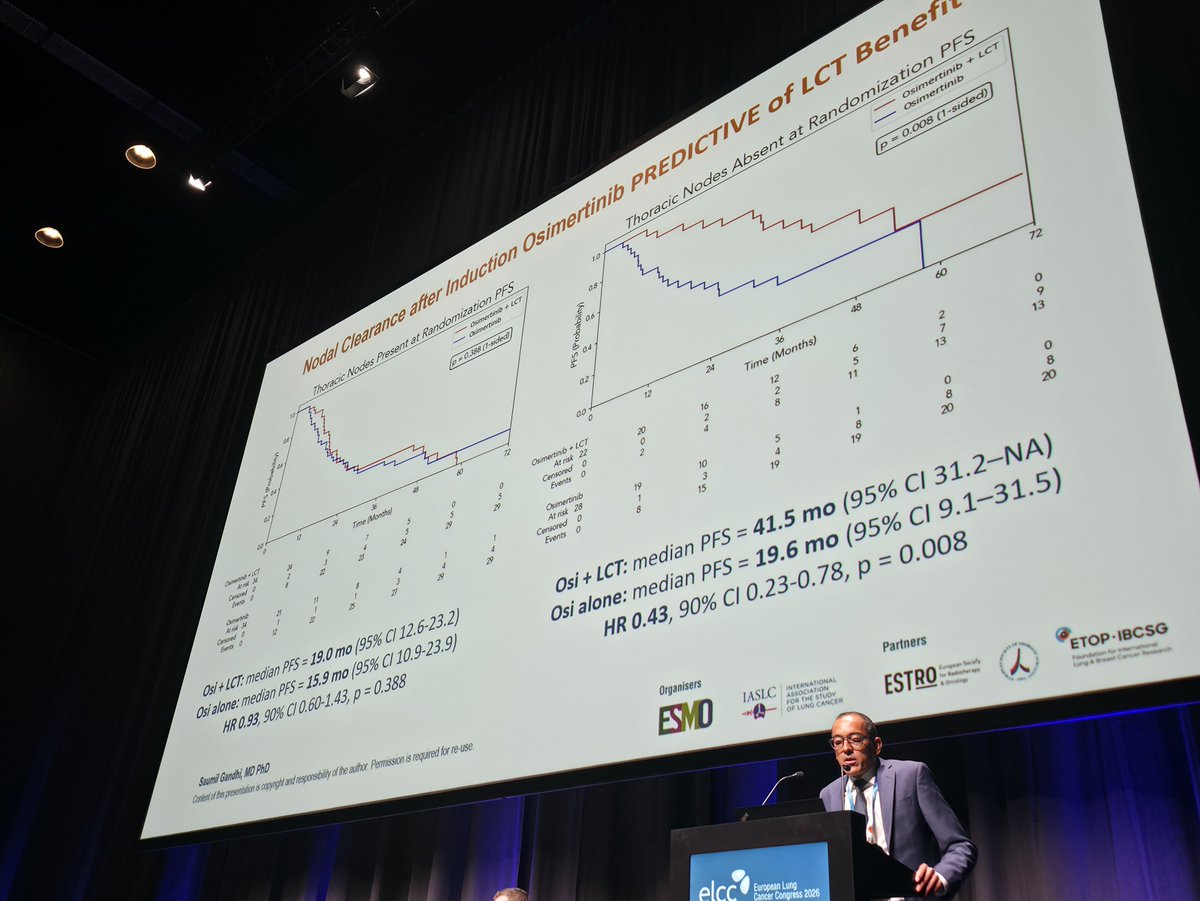
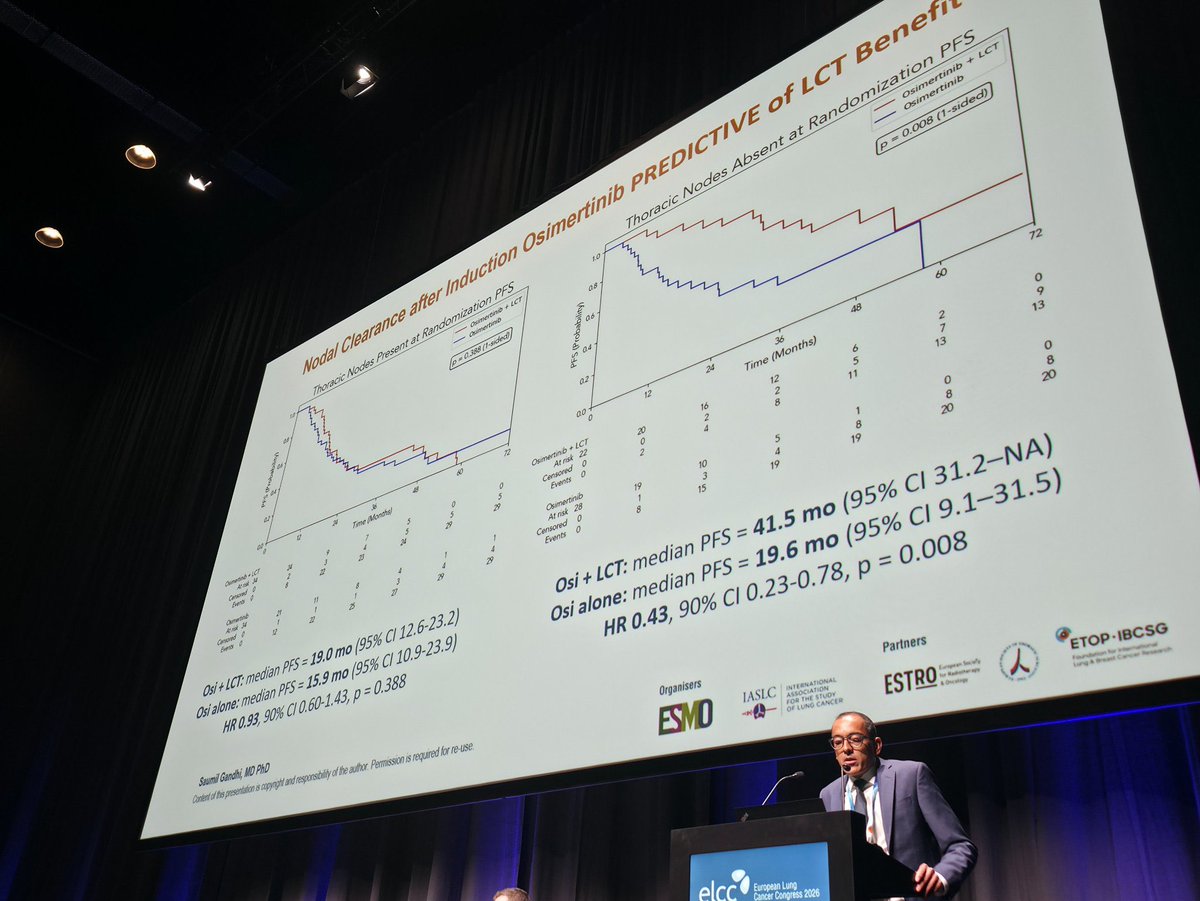
Subgroup / predictors - ELCC 2026 secondary analysis: clearance of thoracic nodal disease after induction identified the strongest local-consolidative-therapy responders (mPFS 41.5 vs 19.6 months); residual thoracic nodal disease or persistent pleural effusion did not derive benefit.
Safety - Local-consolidative-therapy-specific grade 3 events were uncommon (pneumonitis, arterial injury, empyema - 1 case each); treatment overall well tolerated.
Regulatory - Investigational strategy. Osimertinib (Tagrisso) is separately FDA-approved in EGFR-mutant NSCLC; the local-consolidative-therapy addition is not.
Sponsor / drug - MD Anderson Cancer Center; osimertinib (Tagrisso) plus local consolidative therapy.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.










Top tweets by impressions — click to view on X
Dr. @ZPiotrowskaMD discusses NORTHSTAR #ESMO25 - impressive PFS benefit in #EGFR NSCLC when local consolidation therapy added, but notable heterogeneity. Pt selection important, need uniform…
4. #NorthStar: PhII, Osimertinib +/- local consolidative therapy (LCT)for mNSCLC EGFR+:
- ⬆️ PFS w/ LCT (25.3mos vs 17.5mos, HR: 0.66)
- Benefit even with polymetastatic disease
- No new AEs or…
The long-awaited results of NORTHSTAR are finally reported at #ESMO25. @fifimcdrmh https://t.co/GJfCUwnGCO
🆙 #ELCC26 @myESMO @IASLC 🇩🇰
🔥Mini Oral session 1
☑️NorthStar
🎯PFS Osi +/- LCT 41.5m vs. 19.6m (HR 0.43, 90%CI 0.23–0.78)
🎙️Dr. Saumil Ghandi
🎙️Chair: @DocSacher Dr. Andreas…
🔥 Not all EGFRm metastatic NSCLC patients benefit from LCT
#ELCC26
NorthStar (LBA3) secondary analysis finally tells us who truly benefits from adding local consolidative therapy (LCT) to…
#NORTHSTAR update #ELCC26
1️⃣Post-osi CT @ 6-12 wks
•Nodes cleared: 41.5 v 19.6 mo
•Persistent: no benefit
•Effusion gone: 32.7 v 22.3 mo
•Persistent: no benefit
2️⃣RT w/ strong local control
•8%…

“Very few negatives — only positives here.”
Dr. @StephenVLiu wraps up #ESMO2025 in Berlin with his expert insights on HARMONi-6, OptiTROP-Lung04 & a surprise from NorthStar.
🎥 Watch the reports…
🆙 #ELCC26 @myESMO 🇩🇰
🔥Mini Oral session 1
☑️NorthStar
🎯PFS Osi +/- LCT 41.5m vs. 19.6m (HR 0.43, 90%CI 0.23–0.78)
🎙️Dr. Saumil Ghandi
🎙️Chair: @DocSacher Dr. Andreas Rimner
📍NCT04479306
@OncoAlert…
Not all EGFRm NSCLC pts should get LCT
#ELCC26
NorthStar (LBA3) deep dive clarifies who truly benefits from osimertinib + LCT
🧪 After 6–12 weeks induction osimertinib (no progression):
🟢 Best…

Addition of local RT to Osimertinib improves PFS in metastatic NSCLC ( egfr mutated ) Northstar Trial update . @myESMO #elcc26 @DrewMoghanaki @Alfdoc2 @RManochakian https://t.co/pKR0y1G5Sq
NorthStar is the first randomized Phase 2 to show that adding local consolidative therapy (surgery and/or radiotherapy) to osimertinib induction improves PFS in EGFR-mutant metastatic NSCLC (HR 0.66, P=0.025). Best responders are those achieving thoracic nodal clearance after induction, where mPFS reached 41.5 months with LCT vs. 19.6 months without. Small sample size and heterogeneous population are caveats. Applicability in the context of emerging 1L combinations (MARIPOSA [ami + lazertinib], FLAURA2 [osi + chemo]) awaits further study.
Median: 25.3 months (osimertinib + LCT) vs. 17.5 months (osimertinib alone). HR 0.66, P=0.025 PFS in EGFR ex19del subgroup rate: 39.8% (osi+LCT) vs. 22.8% (osi alone). PFS in EGFR L858R subgroup rate: 19.1% (osi+LCT) vs. 11.0% (osi alone). PFS comprehensive LCT vs partial LCT rate: 33.1% (comprehensive) vs. 15.1% (partial). Phase II randomized trial (N=119 non-progressors after 6-12 weeks of osimertinib induction). Median PFS 25.3 months with osimertinib + LCT vs. 17.5 months with osimertinib alone; HR 0.66 (P=0.025) — 34% reduction in progression risk. Subgroups: EGFR ex19del (mPFS 39.8 vs. 22.8 mo, HR 0.58); L858R (19.1 vs. 11.0 mo, HR 0.60); >3 metastases (20.7 vs. 15.9 mo, HR 0.73); comprehensive LCT (33.1 mo) vs. partial LCT (15.1 mo), HR 0.42 (95% CI 0.19-0.90). LCT arm (n=56): surgery 17, radiotherapy 33, both 6. Control (n=63): osimertinib alone.
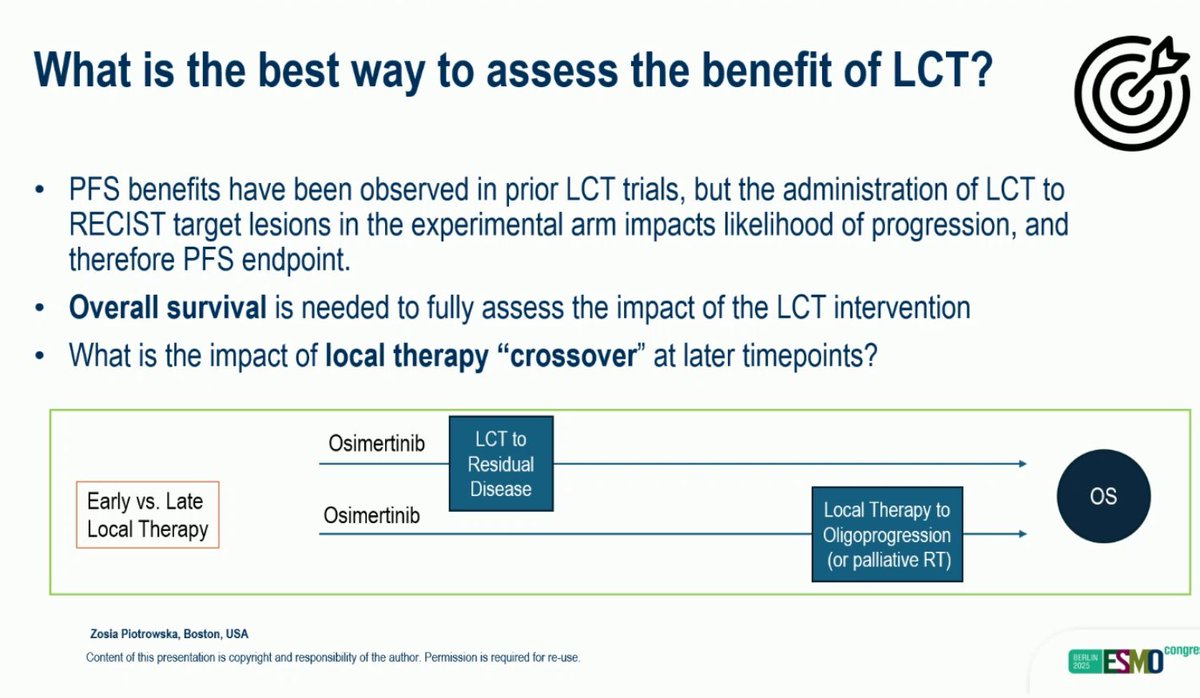
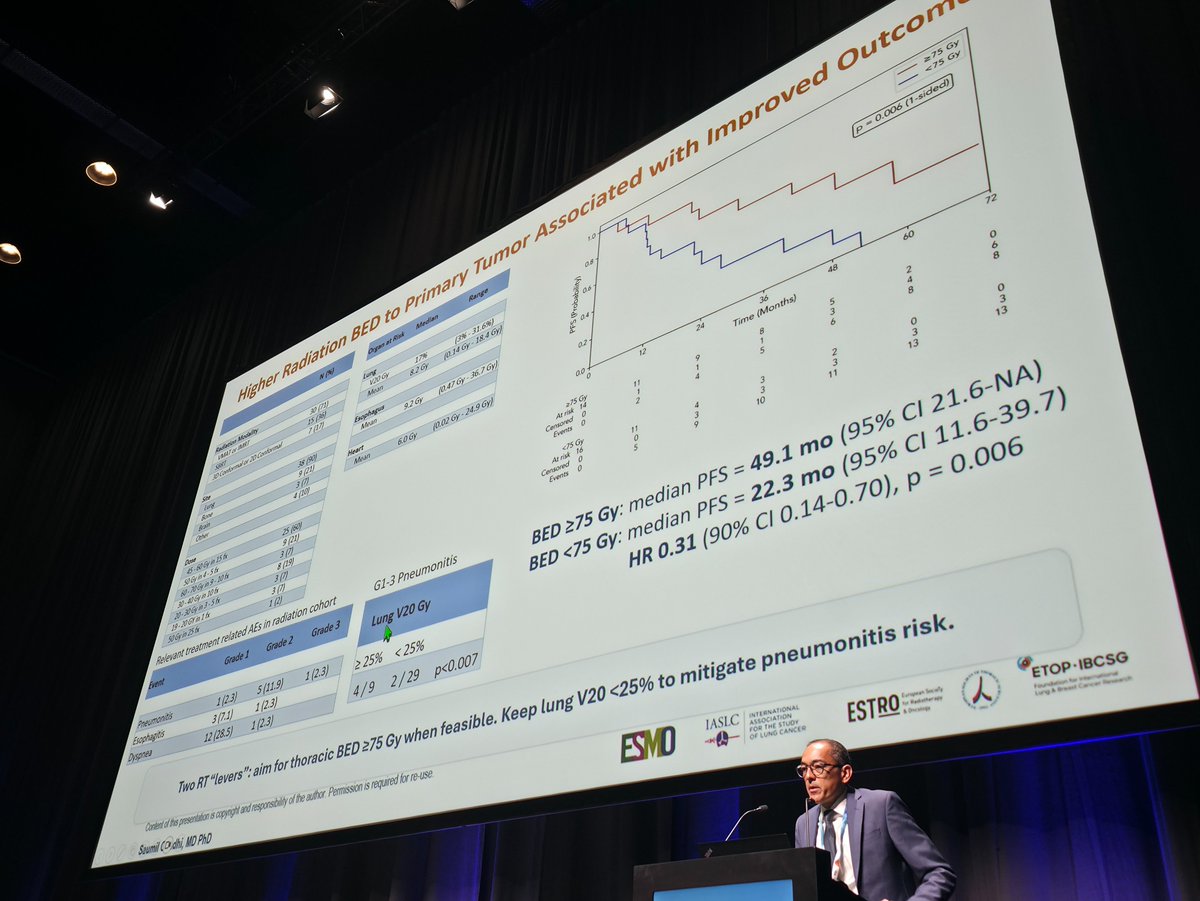
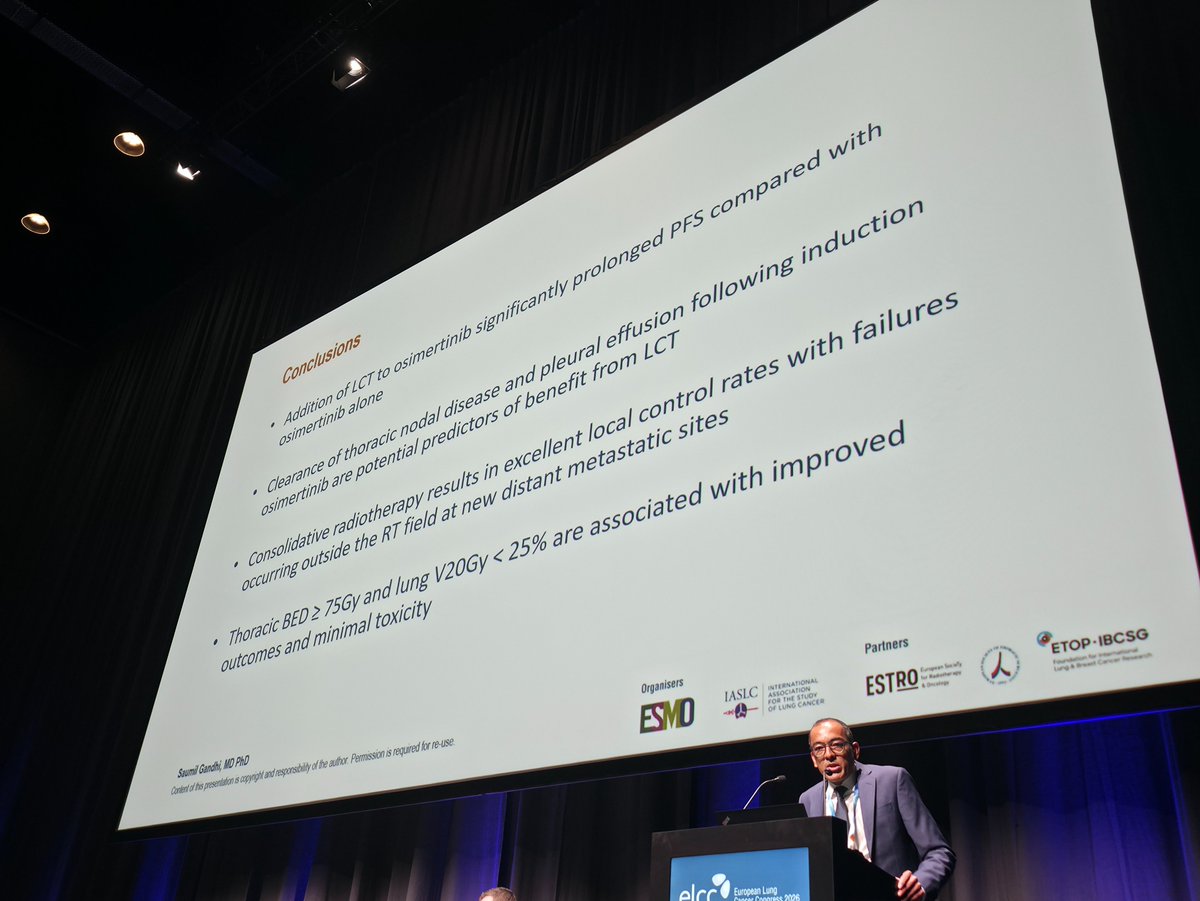
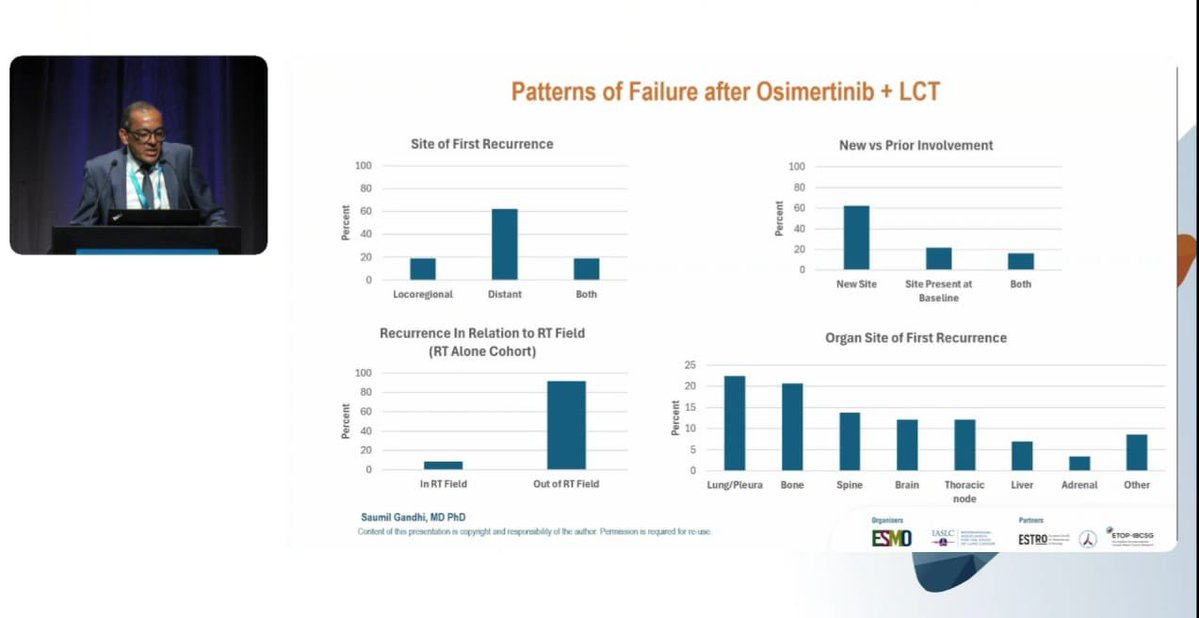
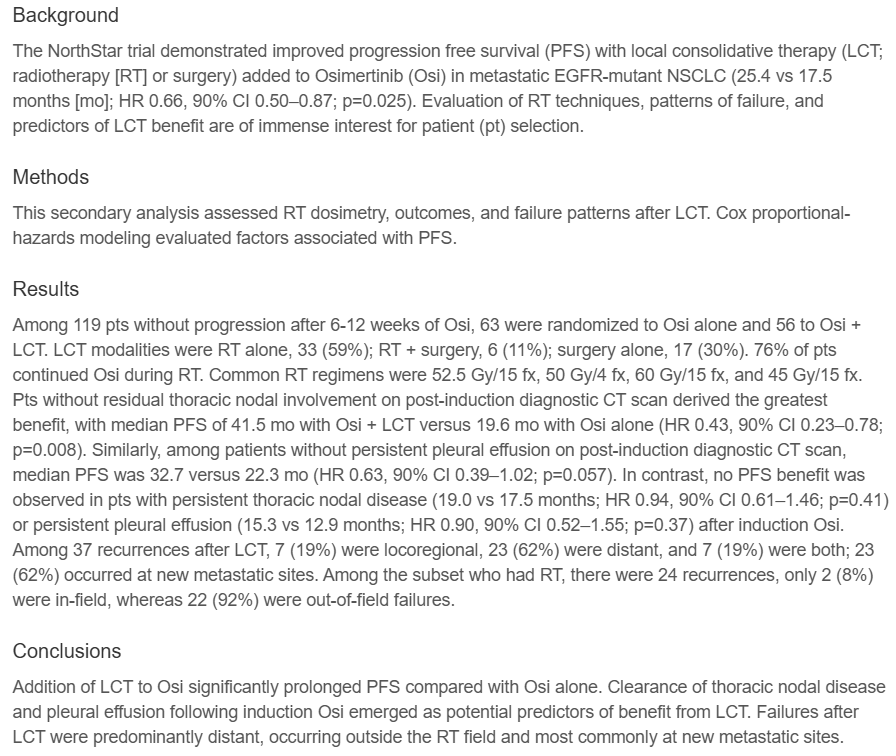
ELCC 2026 secondary analysis: clearance of thoracic nodal disease after induction identifies strongest LCT responders (mPFS 41.5 vs. 19.6 mo). Absence of persistent pleural effusion also predictive. Residual thoracic nodal disease or persistent pleural effusion do NOT derive benefit. 92% of recurrences after LCT were distant (out-of-field); only 8% in-field — systemic progression remains dominant challenge. Maintaining lung V20 <25% reduces toxicity. Higher radiation dose (BED ≥75 Gy) improves outcomes. Median OS data not yet reported.
Key AEs: LCT-specific pneumonitis (1 case, Grade 3), arterial injury (1 case, Grade 3), empyema (1 case, Grade 3). LCT-specific Grade 3 AEs: 3 total cases in LCT arm — pneumonitis, arterial injury, empyema (1 each). Treatment was overall well tolerated. Long-term toxicity assessment needed per investigator commentary.
🔄 Investigational Phase 2: consolidative LCT improves PFS by 7.8 mo (25.3 vs. 17.5) on top of osimertinib in oligometastatic EGFR NSCLC. NorthStar is the first randomized Phase 2 to show that adding local consolidative therapy (surgery and/or radiotherapy) to osimertinib induction improves PFS in EGFR-mutant metastatic NSCLC (HR 0.66, P=0.025). Best responders are those achieving thoracic nodal clearance after induction, where mPFS reached 41.5 months with LCT vs. 19.6 months without. Small sample size and heterogeneous population are caveats. Applicability in the context of emerging 1L combinations (MARIPOSA [ami + lazertinib], FLAURA2 [osi + chemo]) awaits further study.
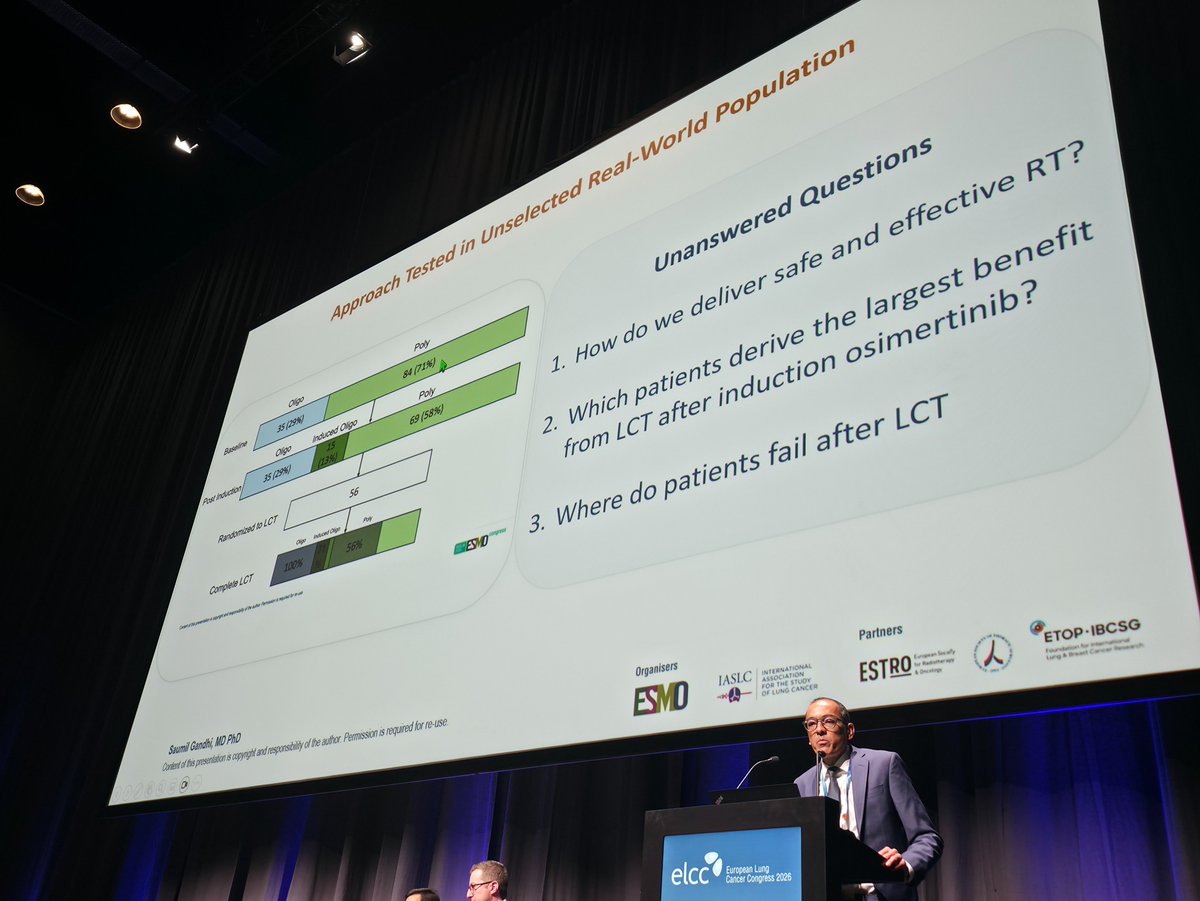
NorthStar (NCT03410043) is a randomized Phase 2 investigator-initiated trial from MD Anderson Cancer Center that tests whether adding local consolidative therapy - surgery and/or radiotherapy - to osimertinib (Tagrisso) improves outcomes in patients with EGFR-mutant locally advanced or metastatic NSCLC whose disease is non-progressing after osimertinib induction.
Adding local consolidative therapy to osimertinib improved median progression-free survival to 25.3 versus 17.5 months with osimertinib alone (hazard ratio 0.66, P=0.025), a 7.8-month improvement. It was the first randomized Phase 2 trial to demonstrate this benefit in oligometastatic EGFR-mutant NSCLC (Elamin et al, ESMO 2025, LBA72).
The addition of local consolidative therapy to osimertinib as tested in NorthStar is an investigational treatment strategy and is not itself an FDA approval. Osimertinib (Tagrisso) is separately FDA-approved for EGFR-mutant NSCLC; local consolidative therapy (surgery and radiotherapy) are established modalities used here in a specific investigational sequence.
An ELCC 2026 secondary analysis found that patients who cleared thoracic nodal disease after osimertinib induction derived the greatest benefit from local consolidative therapy (median progression-free survival 41.5 versus 19.6 months), while those with residual thoracic nodal disease or persistent pleural effusion did not benefit as much - suggesting response to induction can help select candidates.
Local-consolidative-therapy-specific grade 3 adverse events were uncommon, with single cases of pneumonitis, arterial injury and empyema reported in the local-consolidative-therapy arm. Treatment was overall well tolerated, though the investigators noted that long-term toxicity assessment is still needed.