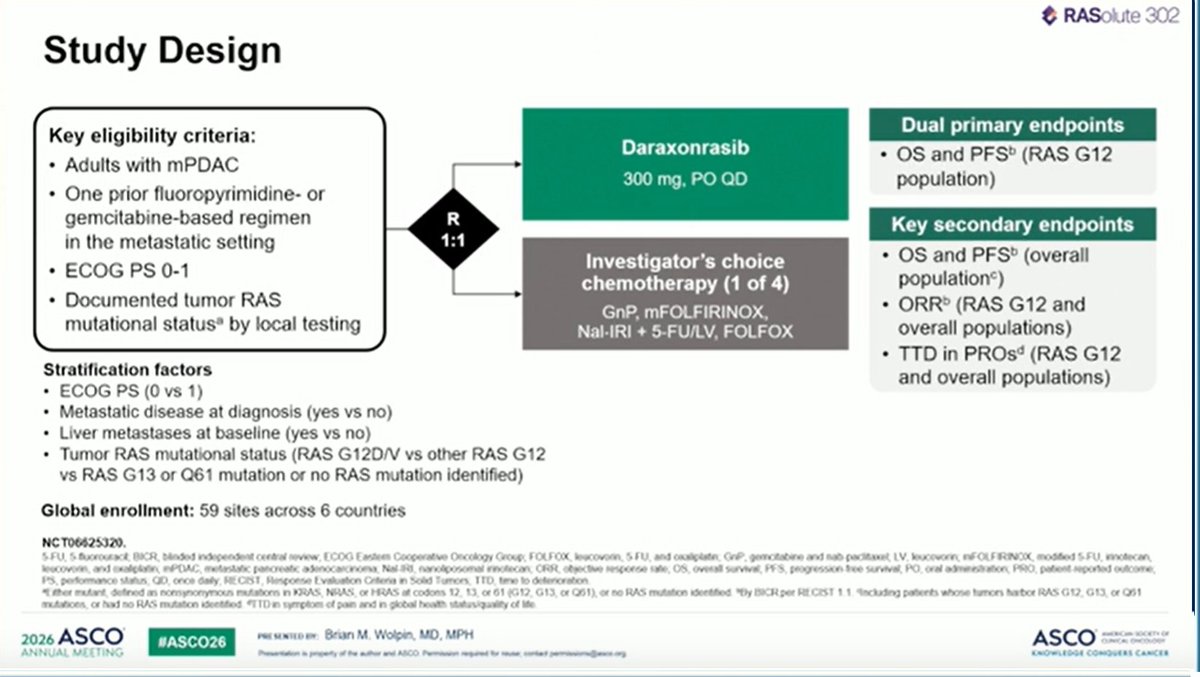
Phase 3 global, randomized trial of once-daily oral daraxonrasib (RMC-6236), a RAS(ON) multi-selective inhibitor, vs investigator's-choice chemotherapy in patients with previously treated metastatic pancreatic ductal adenocarcinoma (PDAC), regardless of RAS mutation status. Presented at the #ASCO26 Plenary (LBA5) by Brian M. Wolpin, MD, MPH (Dana-Farber): median overall survival doubled to 13.2 vs 6.7 months (HR 0.40) — called a "grand slam" from the plenary stage.
#ASCO26 · Plenary · LBA52L Metastatic PDAC (all-comers)Daraxonrasib · Revolution MedicinesPhase 3 · n=500 · global (N. America · Europe · Asia)Published in NEJM (May 31, 2026)⚠️ Investigational · not FDA-approvedFDA Expanded Access authorized (May 1, 2026)
Slides shared by KOLs at the ASCO 2026 Plenary (LBA5, presented by Brian M. Wolpin, MD, MPH, Dana-Farber) plus earlier social conversation. Click any image to expand.
[Slide 1]
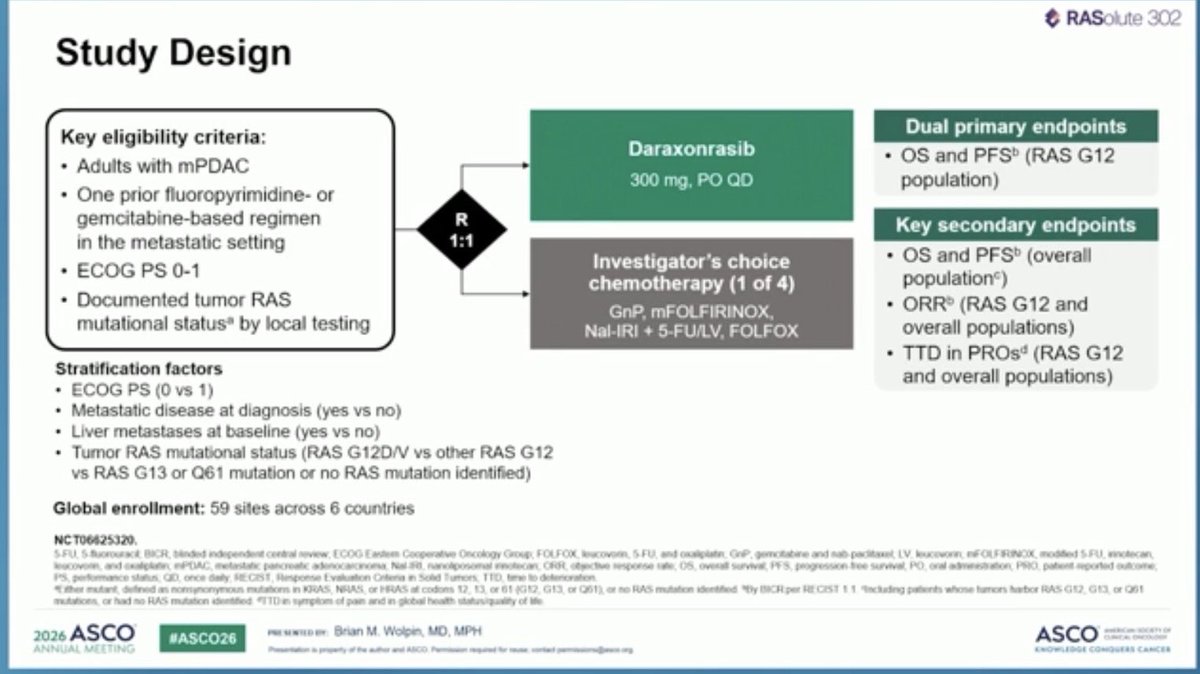
Study Design
Key eligibility criteria:
+ Adults with mPDAC
* One prior fluoropyrimidine- or
gemcitabine-based regimen
in the metastatic setting
+ ECOG PS 0-1
+ Documented tumor RAS
mutational status® by local testing
Stratification factors
+ ECOG PS (0 vs 1)
+ Metastatic disease at diagnosis (yes vs no)
+ Liver metastases at baseline (yes vs no)
* Tumor RAS mutational status (RAS G12D/V vs other RAS G12
vs RAS G13 or Q61 mutation or no RAS mutation identified)
Global enrollment: 59 sites across 6 countries
NCT06625320,
202s ASCO acsomto.y: Brian M. Wolpin, MD, MPH
Daraxonrasib
300 mg, PO QD
Investigator’s choice
chemotherapy (1 of 4)
GnP, mFOLFIRINOX,
Nal-IRI + 5-FU/LV, FOLFOX
@ RASolute 302
Dual primary endpoints
+ OS and PFS® (RAS G12
population)
Key secondary endpoints
* OS and PFS? (overall
population’)
+ ORR? (RAS G12 and
overall populations)
* TTD in PROs* (RAS G12
and overall populations)
---
[Slide 2]
@ RASolute 302
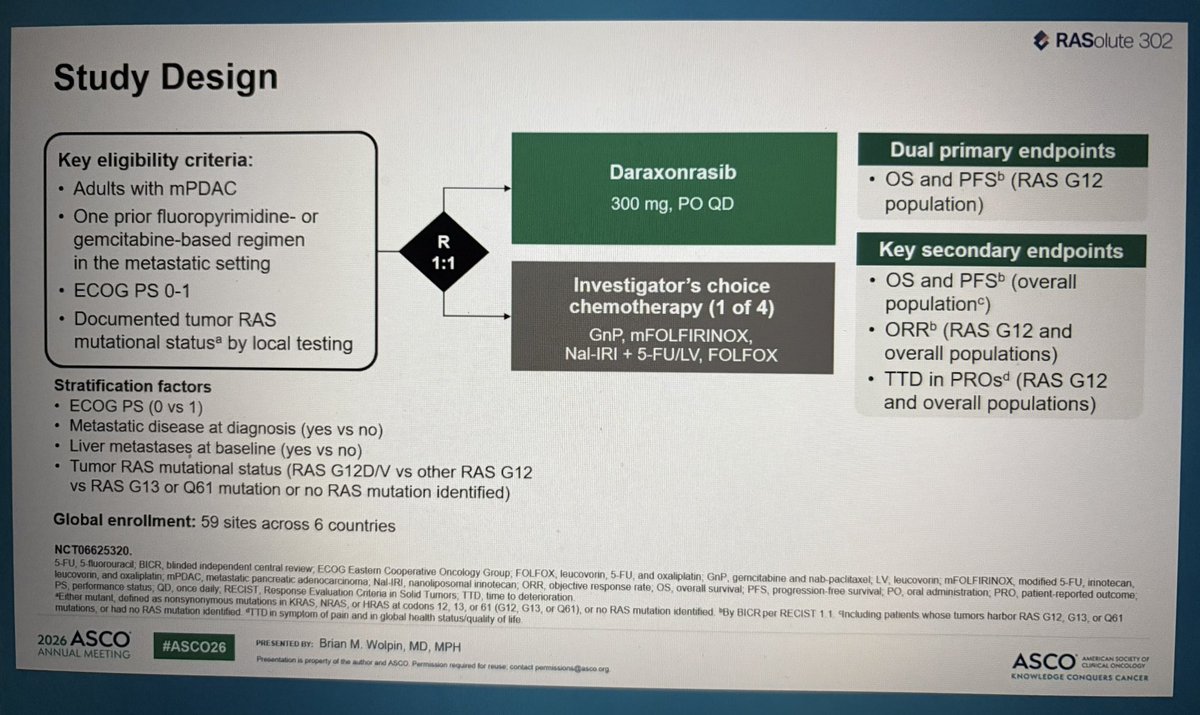
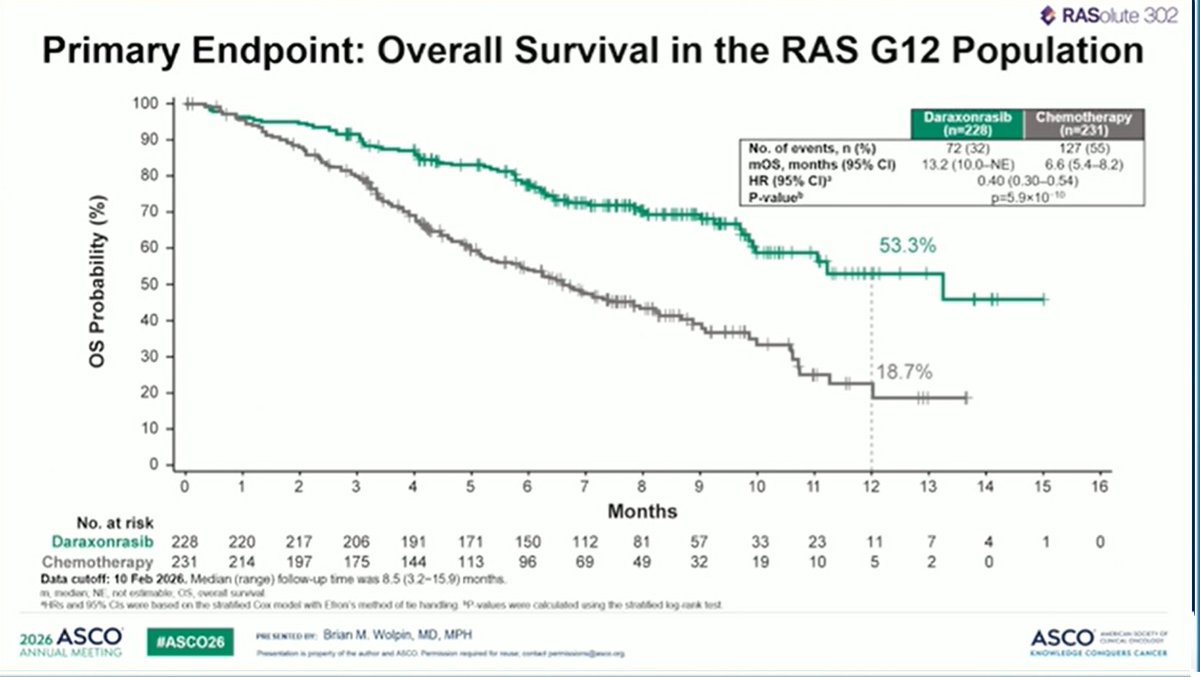
Primary Endpoint: Overall Survival in the RAS G12 Population
100
Daraxonrasib | Chemotherapy
90 (n=228) (n=231)
No. of events, n (%) 72 (32) 127 (65)
mOS, months (95% Cl) 13.2 (10.0-NE) 6.6 (5.4-8.2)
80 HR (95% Cl)? 0.40 (0.30-0.54)
P-value? p=5.9x10-10
70
60
50
40
30
=
2
a
o
3
2
a
a
fo}
20
10
0
10
No. at risk Months:
Daraxonrasib 228 220 217 206 191 171 150 112 81 57 33
Chemotherapy 231 214 197 175 144 113 96 69 49 32 19
Data cutoff: 10 2026. Median (range) follow-up time was 8.5 (3.2-15.9) months.
im, modian, NE, not ostimablo, OS, overall survival
*tHR and 95% Cis wore based on the strated Cox model wih Etron's method of te handing, "P-values were calculated using the straifiod log-rank tost
y presexrcoey: Brian M. Wolpin, MD, MPH
Devens pope te mer and ASCO Pernt reqs rune crkc permasnaiccs og
---
[Slide 3]
@ RASolute 302
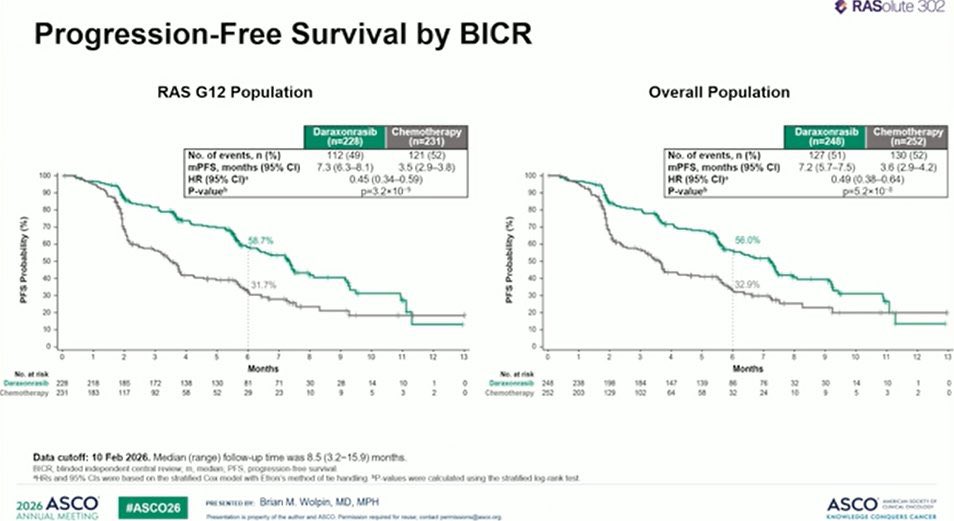
Progression-Free Survival by BICR
RAS G12 Population Overall Population
Daraxonrasib | Chemotherapy Daraxonrasib | Chemotherapy
(n=228} (n=231) (n=248) i (n=252)
No. of events, n (%) 112 (49) 121 (52) No. of events, n (%) 127 (51) 130 (52)
mPFS, months (95% Cl) 7.3(63-8.1) — 35(29-3.8) mPFS, months (95% Cl) 7.2(5.7-7.5) 3.6 (29-4.2)
HR (95% Cp 0.45 (0.34-0.59) HR (95% Clr 0.49 (0.38-0.64)
P-value” p=3.2x10 P-value p=5.2x108
Ey
*
®
Zn =
Fo z
is i
Eo é
Fy 3
| ee a
»
No. at risk
Daraxonrasib 228 218 18S
Chemotherapy 231 183117
Data cutoff: 10 Feb 2026. Median (range) follow-up time was 8.5 (3.2-15.9) months.
BICR, blinded indepondent central review, m, median, PFS, progression tree survival
SHIRS and 95% Cis were based on the stralifod Cox model with Efton's mathod of to handing, ®P.values wore calculated using the stratihod log-rank tost
202s ASCO’ ‘presewrcomy: Brian M. Wolpin, MD, MPH ASCO sess
ANNUAL MEETING prosctaton a peciy eh miter and ASCO Pemsson repre rane: crt peminerence op
---
[Slide 4]
@ RASolute 302
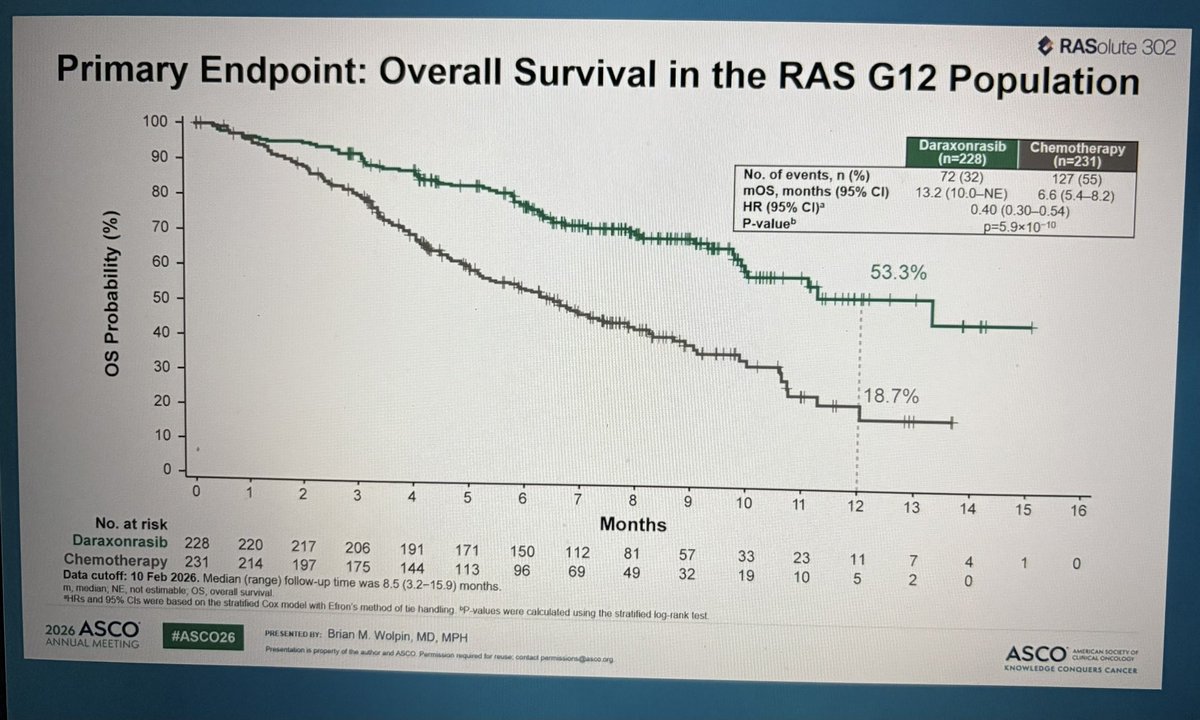
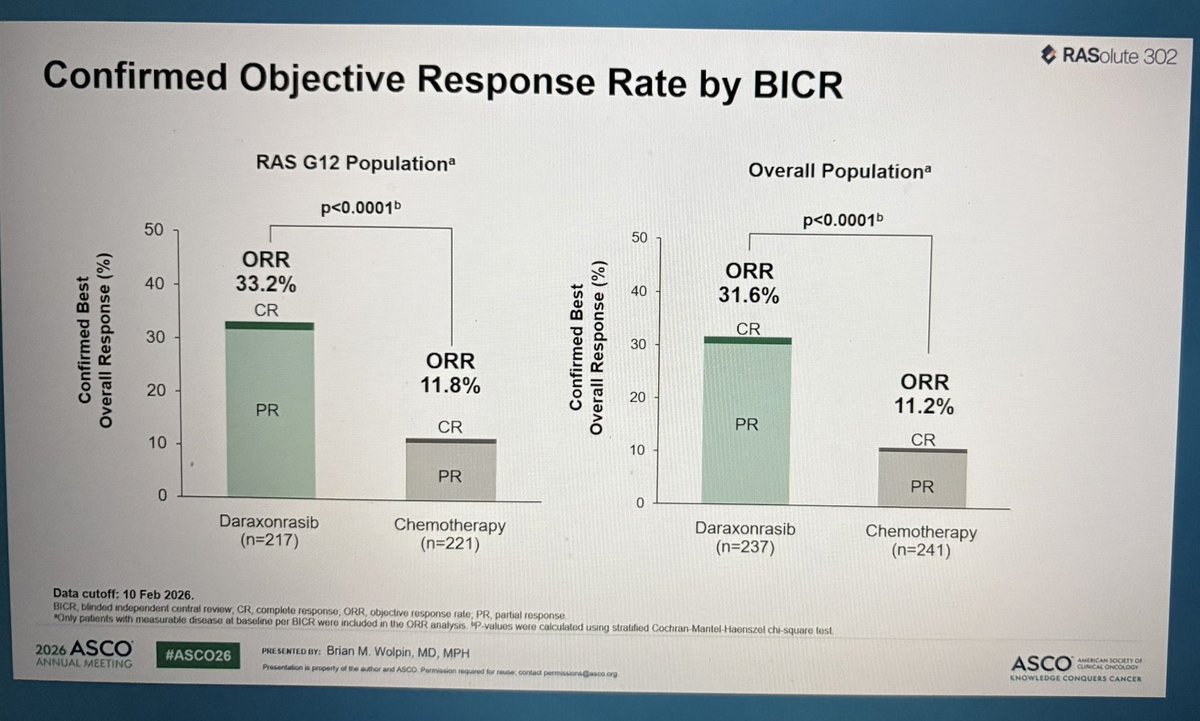
Confirmed Objective Response Rate by BICR
RAS G12 Population*® Overall Population?
p<0.0001> p<0.0001>
ze
ee
8§
g
Confirmed Best
Overall Response (%)
CR
PR
Daraxonrasib Chemotherapy Daraxonrasib Chemotherapy
(n=217) (n=221) (n=237) (n=241)
Data cutoff: 10 Feb 2026.
BBICR, bindod indopondent contral roview, CR, complote response; ORR. objective rosponso rato, PR, partial response
“Only patients wih measurable disease al baseline por BICR were included in the ORR analysis. "P-values wore calculated using stratified Cochran-Mantol-Haenszel chi-square test
2026 ASC #ASCO26 paesexreowy: Brian M. Wolpin, MD, MPH
ANNUAL MEETING Prenran op mite rd ASCO Parmar he ne crt parca on
[Slide 1]
SA tne tte
2026 ASCO
ANNUAL MEETING
Daraxonrasib, a RAS(ON) multi-selective inhibitor vs
chemotherapy in previously treated metastatic
pancreatic adenocarcinoma (mPDAC):
Primary and final analysis from the Phase 3
RASolute 302 study
rian M. Wolpin,' Zev A. Wainberg, Andrew E. Hendifar, Mitesh J. Borad, Filippo Pietrantonio, Shubham
Brian M. Wolpin
Pant, Pascal Hammel, Chiara Cremolini, Gulam A. Manji, Paul E. Oberstein, Ignacio Garrido-Laguna,
to Ueno, Stephen Y. Chui, Ying Zhang, Hina Patel, Yeonju Lee,
Christoph Springfeld, Nilofer S. Azad, Mako!
Zeena Salman, Eileen M. O'Reilly
On behalf of RASolute 302 investigators
tHale Family Center for Pancreatic Cancer Research; Dana-Farber Cancer Institute, Boston, MA, USA
ASCO =
2026ASCO
ANNUAL MEETIN
---
[Slide 2]
€ RASolute 302
Study Design
Dual primary endpoints
+ OS and PFS® (RAS G12
Daraxonrasib
population)
Key eligibility criteria:
+ Adults with mPDAC 300 mg, PO aD
+ One prior fluoropyrimidine- or si
Key secondary endpoints
= Investigator’s choice + OS and PFS? (overall
; a oe Ehenictierapyi(aron) population®)
: GnP, mFOLFIRINOX, * ORR? (RAS G12 and
mutational status® by local testing Nal-IRI + 5-FU/LV, FOLFOX overall populations)
+ TTD in PROs¢ (RAS G12
and overall populations)
gemcitabine-based regimen
in the metastatic setting
Stratification factors
+ ECOG PS (0 vs 1)
+ Metastatic disease at diagnosis (yes vs no)
+ Liver metastases at baseline (yes vs no)
+ Tumor RAS mutational status (RAS G12D/V vs other RAS G12
vs RAS G13 or Q61 mutation or no RAS mutation identified)
Global enrollment: 59 sites across 6 countries
NeT08625320,
SFU, S Arurecl ICR, binded Independent contra review, ECOG Easter, Cooperative Oncology Group; FOLFOX. leucovorin, $-FU, and oxaliplatin. GaP, gemctabine and nab-pacitaxel, LV, eset EOLESION aees CA Een
Joucovorin, and axaiipistin: POAC, stic adenocarcinoma, NalIRi, nanoliposomal innotecan, ORR, objective response rate, OS, overall survival, PFS, progression-tree survival, oral administration: PRO, patien!.reporied outcome,
Se oe re Ls PO,
“Esther mutant, defined a3 nonsynonymous mutations in KRAS, NRAS, or HRAS al codons 12, EGS 12, G13, or Q1), or no RAS mutation identified. "By BICR per RECIST 1.1. ‘inchuding patients
‘mulatons, or had no RAS mutation Kientiied. «TTD in symptom of pain and in global heath statusia aves beers BOSS OAS Gta. oat Oa
ASCO sane
MOWLIBGE CONQUERS CANCER
+6 ASCO #ASCC presexreo er: Brian M. Wolpin, MD, MPH
ANNUAL MEETING Proventaton @ procerty of he mtr ard ASCO Penrason regared toy neue Contac! permauona (hance oy
[Slide 1]
Abstract LBA5
Daraxonrasib, a RAS(ON) multi-selective inhibitor vs
chemotherapy in previously treated metastatic
pancreatic adenocarcinoma (mPDAC): Primary and final
analysis from the phase 3 RASolute 302 study.
Authors
Brian M. Wolpin, Zev A. Wainberg, Andrew Hendifar, Mitesh
J. Borad, Filippo Pietrantonio, Shubham Pant, Pascal
Hammel, Chiara Cremolini, Gulam A. Manji, Paul E.
Oberstein, Ignacio Garrido-Laguna, Christoph Springfeld,
Nilofer S. Azad, Makoto Ueno, Stephen Y. Chui, Ying Zhang,
Hina Patel, Yeonju Lee, Zeena Salman, Eileen M. O'Reilly
---
[Slide 2]
Results:
248 pts were randomized to daraxonrasib and 252 to
chemo. Baseline characteristics were balanced between
arms. At data cutoff (Feb 10, 2026; mFU: 8.5 mo), all
primary and key secondary endpoints were met.
Statistically significant, clinically meaningful
improvements in OS and PFS were observed with
daraxonrasib vs chemo in the RAS G12 and overall
populations (Table). Gr >3 TRAEs occurred in 43.6% of pts
receiving daraxonrasib vs 57.5% receiving chemo. The
most common (210%) Gr >3 TRAEs were rash (13.7%) and
stomatitis (12.0%) for daraxonrasib; neutrophil decrease
(18.2%) and anemia (16.4%) for chemo. TRSAEs occurred
in 10.8% of pts receiving daraxonrasib vs 18.7% receiving
chemo. Discontinuation due to TRAEs occurred in 1.2% of
pts for daraxonrasib vs 11.2% for chemo. Median/mean
daraxonrasib dose intensity was 93.1%/84.7%.
---
[Slide 3]
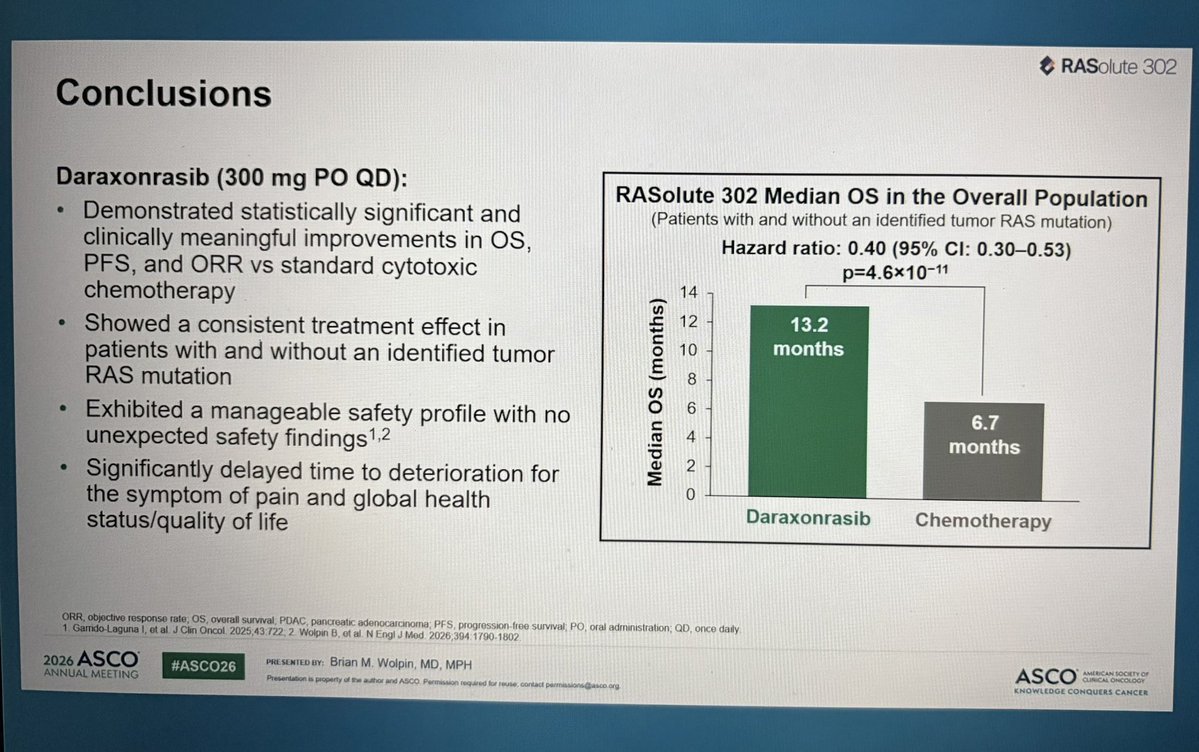
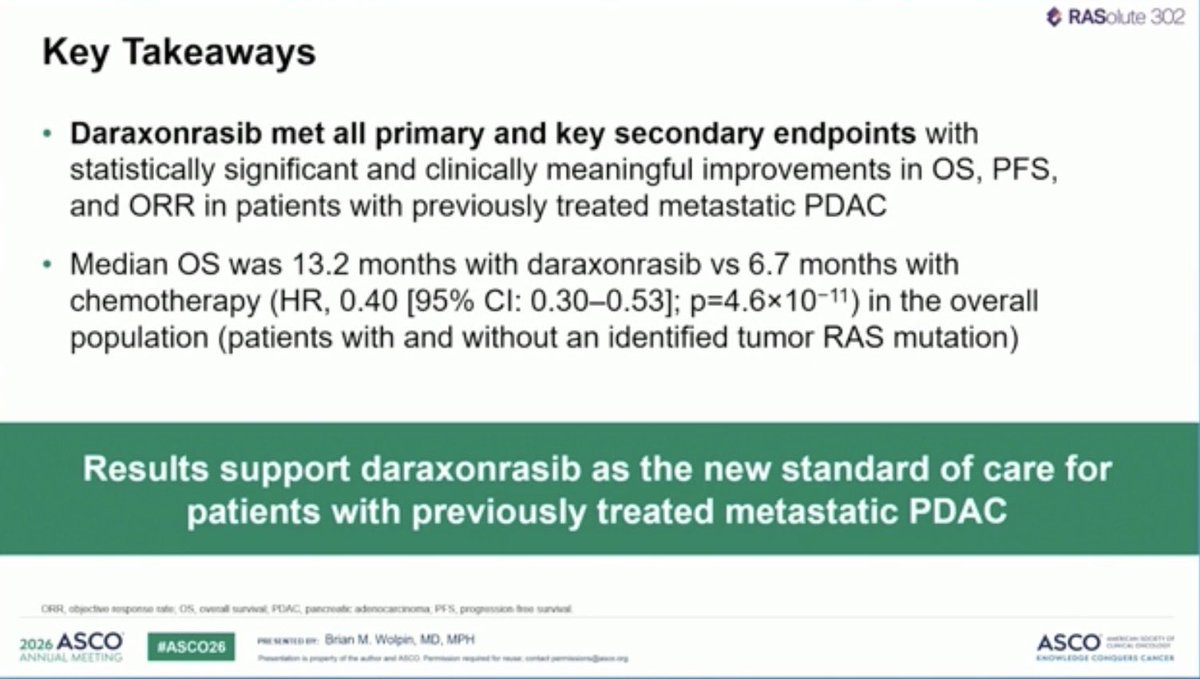
Conclusions:
Daraxonrasib demonstrated unprecedented improvements
in OS and PFS vs chemo in pts with 2L mPDAC with or
without an identified tumor RAS mut. Daraxonrasib was
generally well tolerated, with a manageable safety profile
and with no new safety signals. Results support
daraxonrasib as the new SOC for 2L mPDAC.
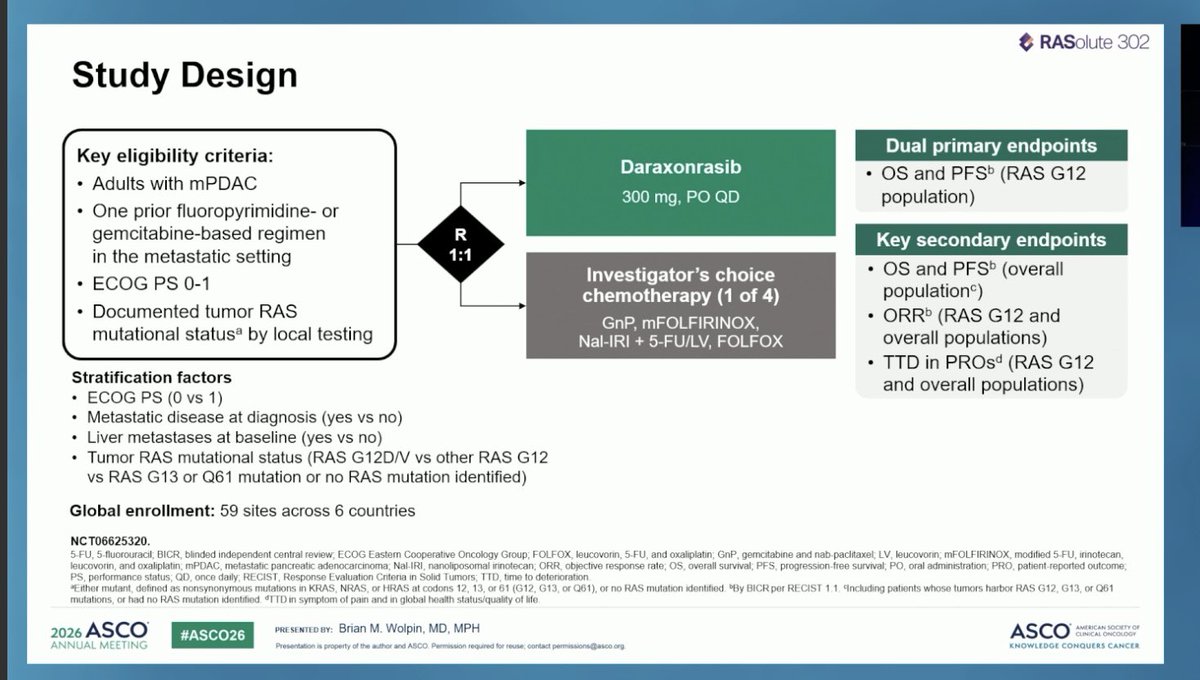
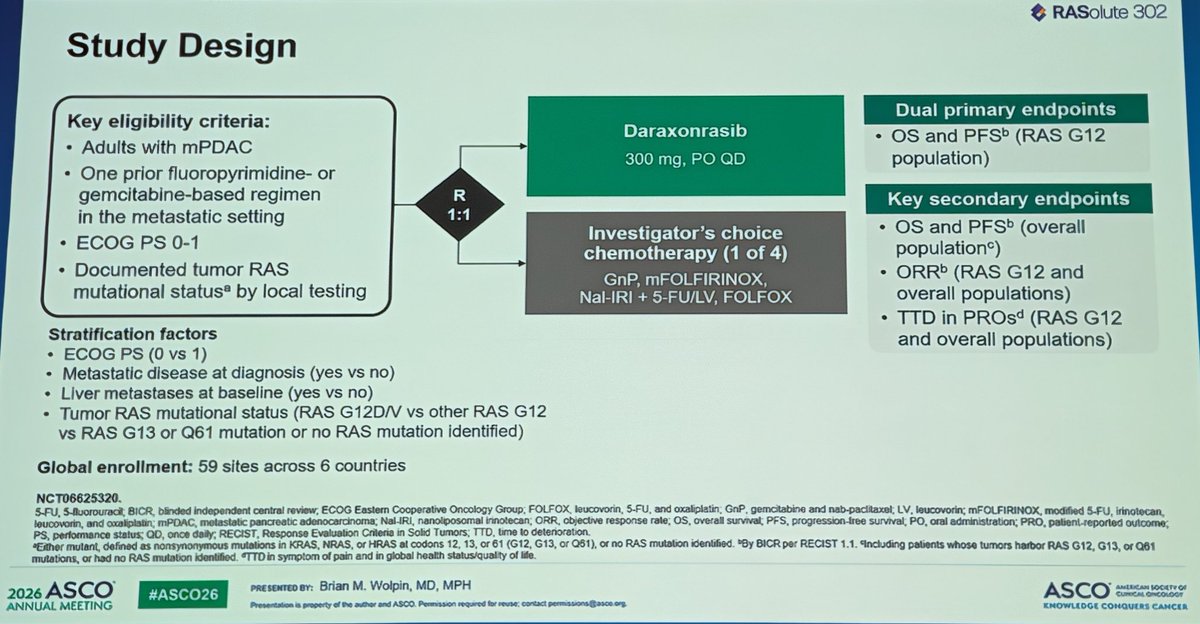
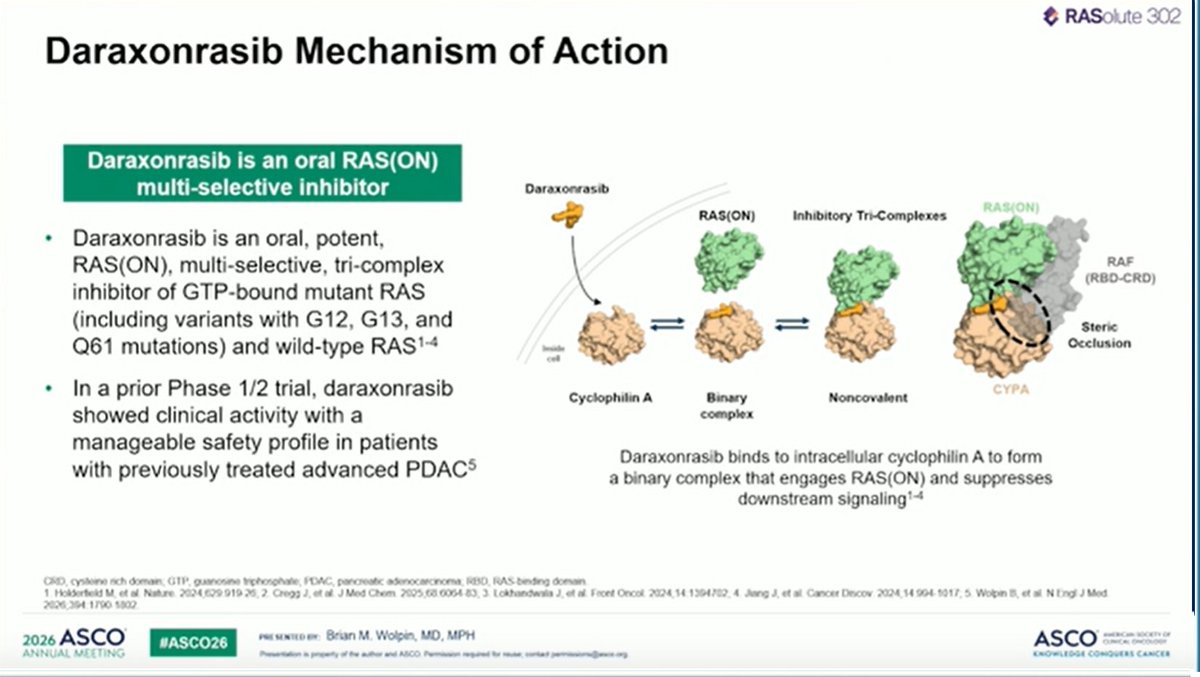
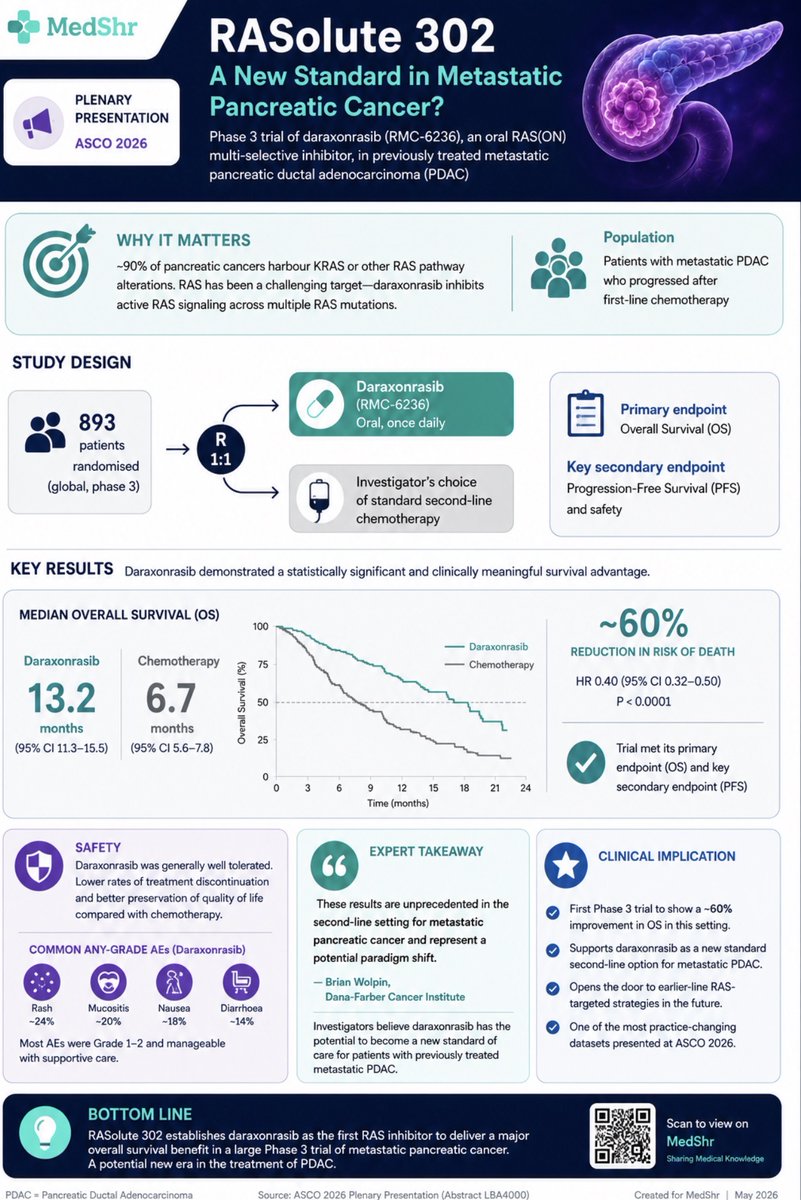
RASolute 302 is a global, randomized Phase 3 trial of daraxonrasib (RMC-6236) — the first investigational oral RAS(ON) multi-selective inhibitor — versus investigator's-choice cytotoxic chemotherapy as second-line therapy for patients with metastatic pancreatic ductal adenocarcinoma (PDAC) who progressed on one prior fluoropyrimidine- or gemcitabine-based regimen. The trial enrolled 500 patients globally (North America, Europe, and Asia), randomized 1:1 (daraxonrasib n=248; chemotherapy n=252); enrollment did not require a RAS mutation, though the large majority (459/500) harbored a RAS G12 mutation. Co-primary endpoints (OS and PFS in the RAS G12 population) were met, with consistent benefit in the intent-to-treat population. Full results were presented at the #ASCO26 Plenary Session (LBA5) by Brian M. Wolpin, MD, MPH (Dana-Farber) and published simultaneously in the New England Journal of Medicine.
Study Design
Phase 3, global, randomized, open-label. Patients with metastatic PDAC who progressed on one prior line randomized to oral daraxonrasib 300 mg once daily vs investigator's-choice chemotherapy. Stratified by RAS mutation status and region.
Population
n=500 with metastatic PDAC, one prior fluoropyrimidine- or gemcitabine-based regimen, ECOG 0-1. RAS mutation not required for entry; 459/500 (~92%) had a RAS G12 mutation. Co-primary populations: RAS G12 and ITT.
Intervention
Experimental: Daraxonrasib (RMC-6236) 300 mg orally once daily until progression or unacceptable toxicity. Control: Investigator's choice of standard second-line cytotoxic chemotherapy.
Endpoints
Co-primary: OS and PFS (BICR) in the RAS G12 population. Key secondary: OS and PFS in the ITT population, objective response rate (ORR), duration of response, safety/tolerability.
Efficacy & Safety
Primary Results — #ASCO26 Plenary (LBA5)
INVESTIGATIONALDaraxonrasib is not approved by the FDA for any indication
RASolute 302 is the first Phase 3 readout for daraxonrasib (RMC-6236). The drug is investigational and not FDA-approved; the data described here are from a single pivotal trial presented at ASCO 2026 and published in NEJM. Revolution Medicines is evaluating daraxonrasib in additional Phase 3 registrational trials, including earlier-line PDAC and RAS-mutant NSCLC.
Overall Survival (Co-Primary Endpoint — MET)
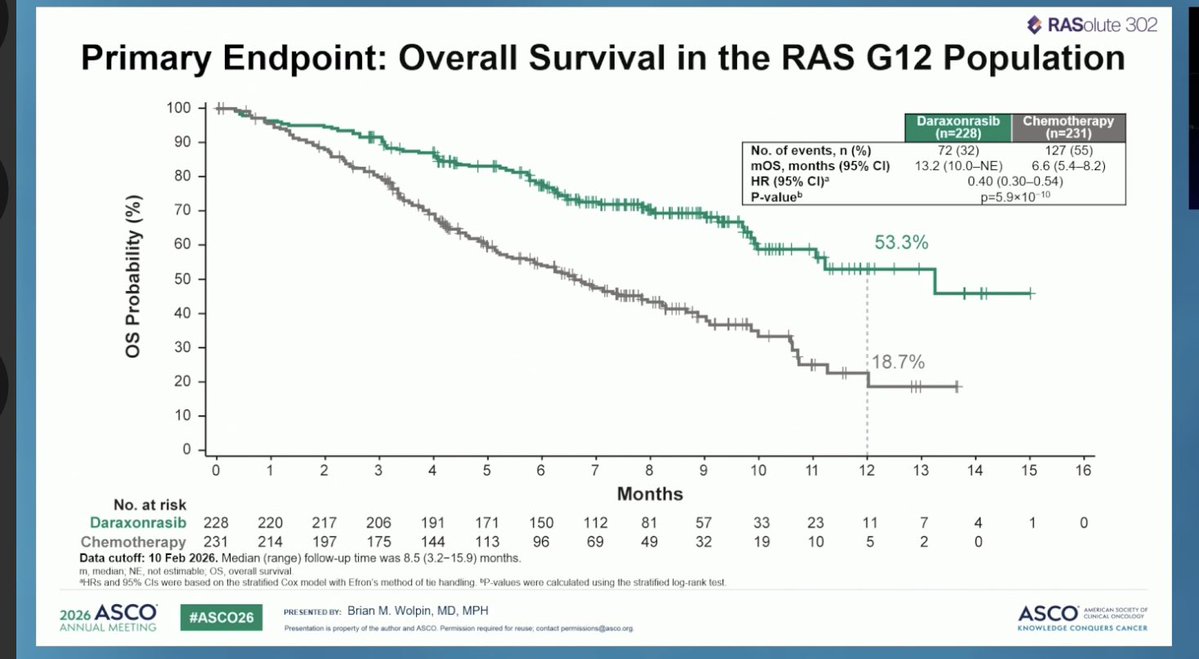
Daraxonrasib produced a statistically significant and clinically meaningful improvement in overall survival, doubling median OS versus chemotherapy. In the intent-to-treat population, median OS was 13.2 vs 6.7 months (HR 0.40; 95% CI 0.30–0.53; p<0.0001) — a 60% reduction in the risk of death. The RAS G12 population showed the same HR of 0.40 (95% CI 0.30–0.54; p<0.0001), median OS 13.2 vs 6.6 months. Median OS exceeding 12 months in the second-line PDAC setting is unprecedented.
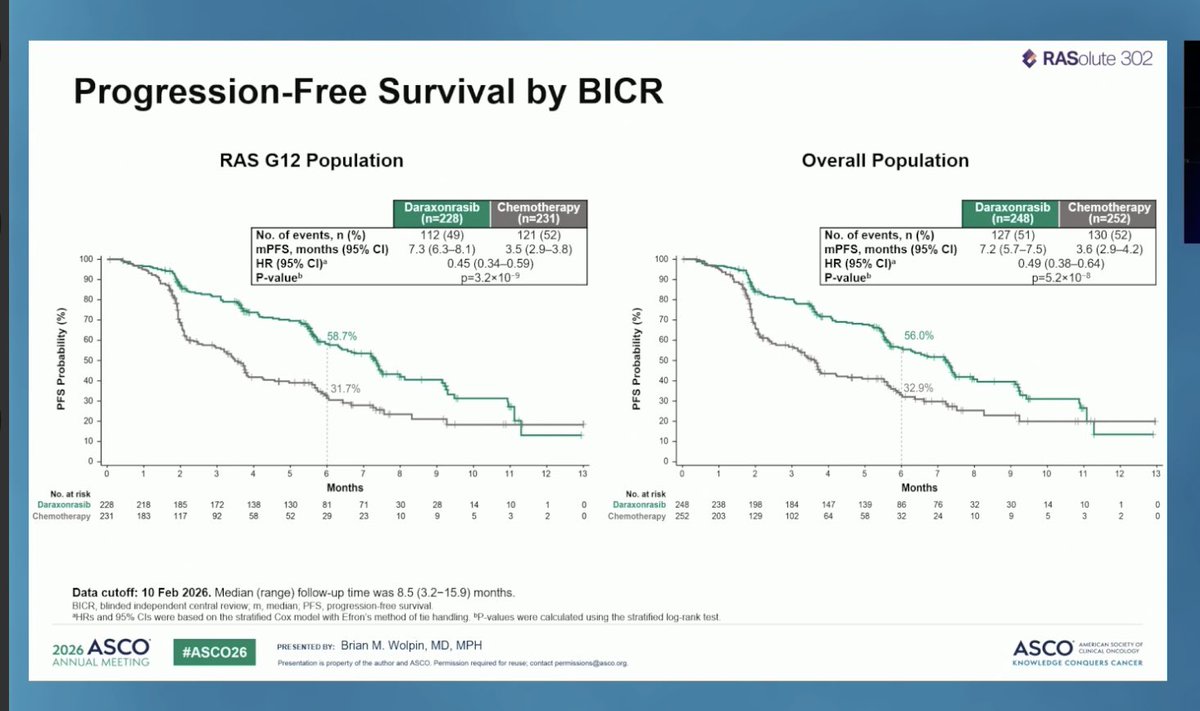
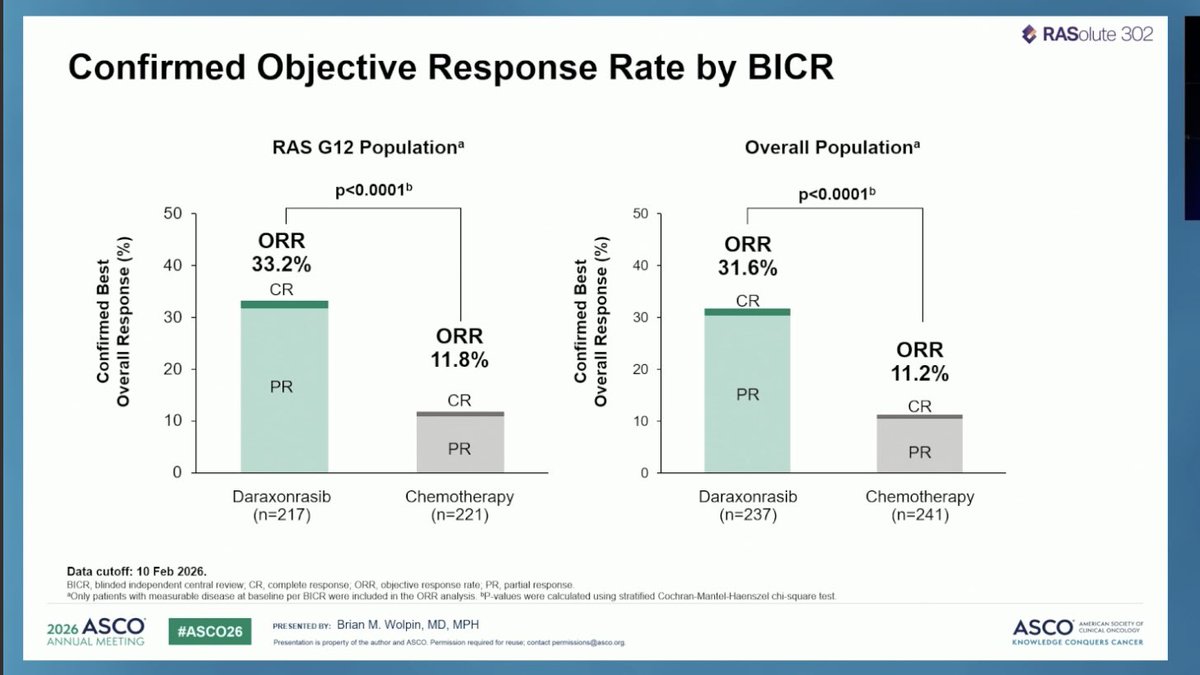
Daraxonrasib also doubled blinded independent central review (BICR) PFS, with a median of 7.2 vs 3.6 months versus chemotherapy. In the RAS G12 population, the PFS hazard ratio was 0.45 (95% CI 0.34–0.59). The objective response rate was roughly tripled — 33.2% vs 11.8% in the RAS G12 population.
Daraxonrasib is not a benign drug — it carries real, on-target RAS-pathway toxicity that demands active, ongoing management. Grade 3 or higher treatment-related adverse events (TRAEs) occurred in 43.6% of daraxonrasib patients (vs 57.5% with chemotherapy). The most frequent Grade ≥3 TRAEs were rash (14%) and stomatitis (mouth inflammation, 12%); the most common all-grade toxicities were rash, mouth inflammation (stomatitis), nausea, and diarrhea. Treatment-related serious AEs occurred in 10.8% (vs 18.7%), and there was one Grade 5 (fatal) treatment-related pneumonitis (0.4%) in the daraxonrasib arm. Rash is significant enough that the protocol recommends prophylactic oral antibiotics and topical corticosteroids. The toxicities were consistent with prior Phase 1/2 (RMC-6236-001) experience, with no unexpected new signals. Median dose intensity was 93.1%. Treatment discontinuation due to TRAEs was 1.2% vs 11.2% with chemotherapy.
RASolute 302 is the first positive Phase 3 trial of a RAS-targeted therapy in pancreatic cancer, a disease in which ~90% of tumors are KRAS-driven and second-line chemotherapy delivers only 6–7 months of median survival. ASCO leadership and discussants described the result as a "grand slam," and multiple KOLs framed daraxonrasib as a potential new second-line standard of care, pending regulatory review. The all-comers benefit (regardless of RAS mutation status) reinforces the rationale for the broader RAS(ON) multi-selective mechanism.
INVESTIGATIONALDaraxonrasib is not approved by any regulatory authority
Daraxonrasib (RMC-6236) is an investigational oral RAS(ON) multi-selective inhibitor that is not approved by the FDA or any other regulatory authority. RASolute 302 is its first Phase 3 readout. The facts below describe the drug's current U.S. regulatory standing — none of which constitutes an FDA approval.
EXPANDED ACCESSFDA authorizes an Expanded Access Program (May 1, 2026)
The FDA issued a “safe to proceed” letter to Revolution Medicines, allowing the company to initiate an expanded access treatment protocol (EAP) for daraxonrasib in patients with previously treated metastatic PDAC. The FDA received the request on April 28, 2026 and signed it on April 30 — a two-day turnaround that FDA Commissioner Marty Makary, MD, MPH cited as reflecting “the FDA’s strong commitment to facilitate early access to therapies for serious and life-threatening conditions.” The EAP provides a pathway outside a clinical trial for eligible patients who have no comparable or satisfactory alternative and are unable to enroll in an ongoing daraxonrasib trial. Per FDA regulations, requests must be initiated by a U.S.-licensed treating physician — Revolution Medicines cannot accept requests directly from patients or caregivers.
Planned NDA Submission — Commissioner’s National Priority Voucher
Revolution Medicines announced on April 13, 2026 that it intends to submit a New Drug Application (NDA) for daraxonrasib under the FDA Commissioner’s National Priority Voucher (CNPV) pilot program, which is intended to accelerate the development and review of therapies aligned with U.S. national health priorities. The FDA granted daraxonrasib a national priority voucher in October 2025. The company intends to submit the RASolute 302 data to global regulatory authorities, including the FDA.
The FDA previously granted daraxonrasib Breakthrough Therapy Designation and Orphan Drug Designation for the treatment of patients with previously treated metastatic PDAC harboring RAS G12 mutations. These designations expedite development and review but do not constitute approval.
All efficacy and safety figures cited above are sourced to the Revolution Medicines ASCO Plenary press release (May 31, 2026), the simultaneous NEJM publication (Wolpin et al.), and the Dana-Farber newsroom; ORR and discontinuation figures are from the same primary readout. RASolute 302 reflects a single data cut presented at #ASCO26.
In the News
Media Coverage & Analysis
Selected coverage and KOL analysis of the RASolute 302 Plenary readout. External links open in a new tab.