TROPiCS-04 is a Phase 3 trial of the TROP-2 antibody-drug conjugate sacituzumab govitecan (Trodelvy) versus chemotherapy in pretreated locally advanced or metastatic urothelial cancer (after platinum and a checkpoint inhibitor). It did not meet its primary overall-survival endpoint and showed higher early mortality from neutropenic complications. The U.S. urothelial accelerated approval was voluntarily withdrawn; Trodelvy remains approved in breast cancer. Sponsor: Gilead Sciences.
Discover KOL Sentiment on TROPiCS-04 →Design — Phase 3, randomized confirmatory trial; sacituzumab govitecan (Trodelvy) vs physician's-choice chemotherapy, pretreated locally advanced/metastatic urothelial cancer (post-platinum, post-checkpoint inhibitor), NCT04527991. (ESMO 2024)
Overall survival (primary) — NOT met — no statistically significant OS benefit in the ITT population; a numerical trend and some subgroup/secondary signals favored sacituzumab govitecan but were not alpha-controlled. (ESMO 2024)
Early mortality signal — More deaths due to adverse events with sacituzumab govitecan, concentrated early in treatment and related to neutropenic complications including infection. (ESMO 2024)
Safety — No new safety signals beyond the known Trodelvy profile — severe/life-threatening neutropenia (Boxed Warning) and diarrhea — but the early-mortality imbalance was decisive. (ESMO 2024 / label)
Regulatory (indication-critical) — Urothelial accelerated approval (April 2021, TROPHY-U-01 basis) VOLUNTARILY WITHDRAWN after TROPiCS-04 failed; Trodelvy no longer available for bladder cancer. Breast cancer indications unaffected. (FDA.gov)
Sponsor / Drug — Gilead Sciences; sacituzumab govitecan (Trodelvy), a TROP-2-directed antibody-drug conjugate. (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.













Top tweets by impressions — click to view on X
Just in @Annals_Oncology by @tompowles1 @PGrivasMDPhD & team👉Ph3 TROPiCS-04 trial result👉Sacituzumab govitecan (SG) vs physician’s choice chemoRx in pretreated mUC #bladdercancer👉No OS or PFS…
We just published TROPiCS04 P3 trial data @Annals_Oncology with @tompowles1 @y_loriot @DrScottTagawa et al.
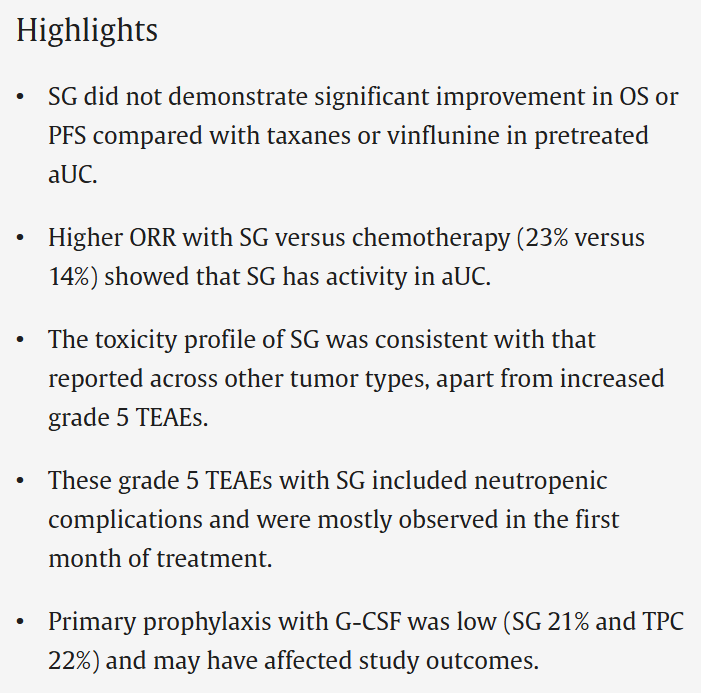
Primary OS endpoint was not met, higher ORR with SG (23%) vs taxane/vinflunine (14%), G-CSF…
So important that this dataset from @tompowles1 @Uromigos @BartsECMC, @PGrivasMDPhD @fredhutch @UW, et al is out there for our detailed evaluation. The role of #sacituzumab in #BladderCancer appears…
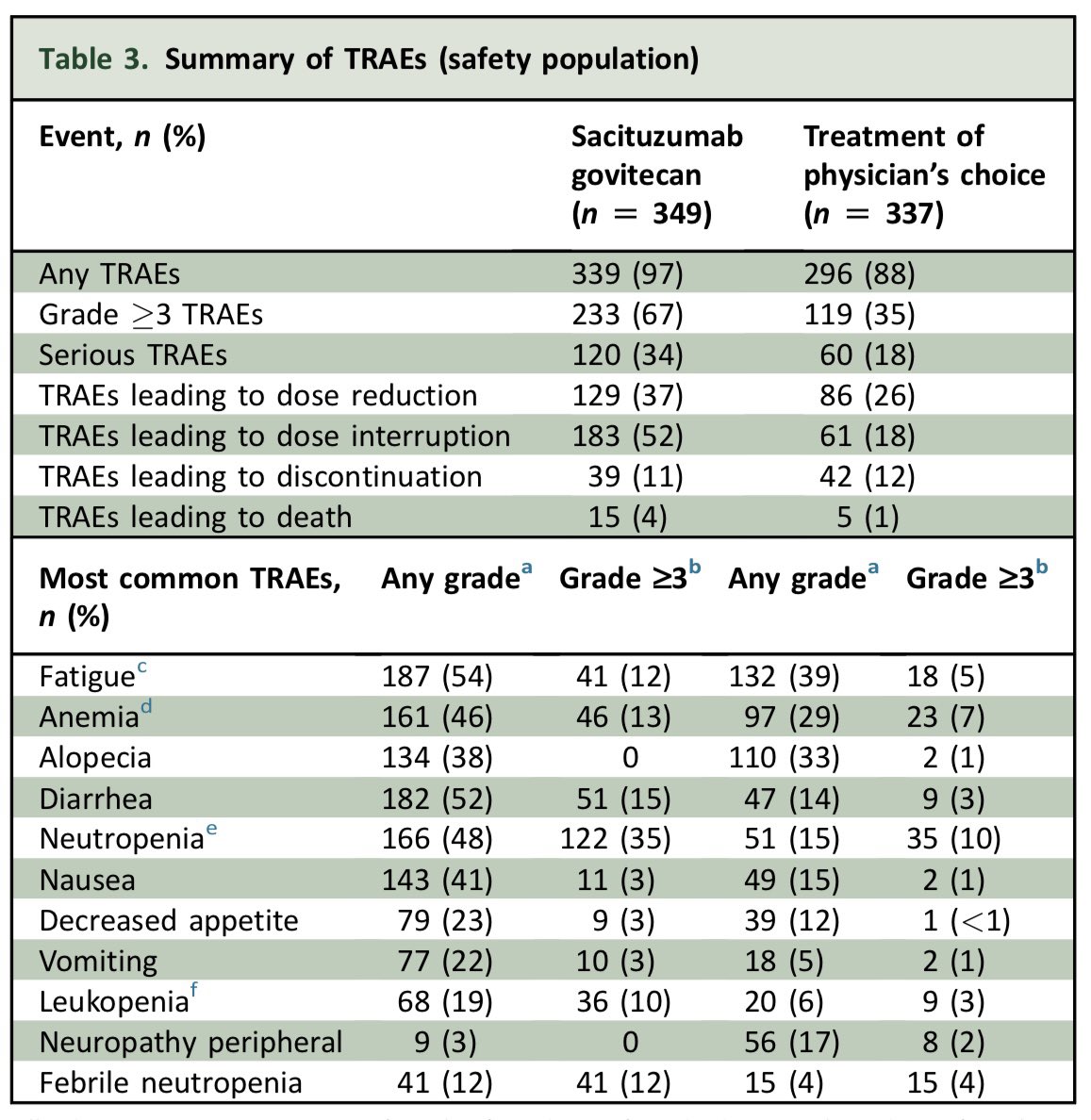
TROPICS4 sacituzimab govitecan vs chemo in pretreated UC @Annals_Oncology OS & PFS HRs=0.86. RR 23 vs 14, but G3+ TRAE 67 vs 35% with ⬆️ G5 TRD. While there is activity the ⬆️ tox & lower RR…
Phase 3 TROPiCS-04 in Metastatic Bladder Cancer: single agent ADC (SG) was not superior to trt choice chemo in terms of OS
@BladderCancerUS @DanaFarber_GU @OncoAlert @OncoBellmunt…
TROPiCS-04 trial out on @Annals_Oncology: no statistical improvement in OS with the Trop2 ADC #SG vs TPC in met urothelial cancer, with higher rate of G5 AEs with SG. Led to the withdrawal of SG…

Congrats @tompowles1 @PGrivasMDPhD @y_loriot @AndreaNecchi & entire TROPICS-04 team on getting the data out in @Annals_Oncology
It is crucial to learn from negative trials & important…

Phase 3 TROPiCS-04 Study in metastatic #BladderCancer (post platinum & CPI) of sacituzimab govitecan #SG vs 2L chemo did not meet OS endpoint. However, drug is active & well tolerated. Will…

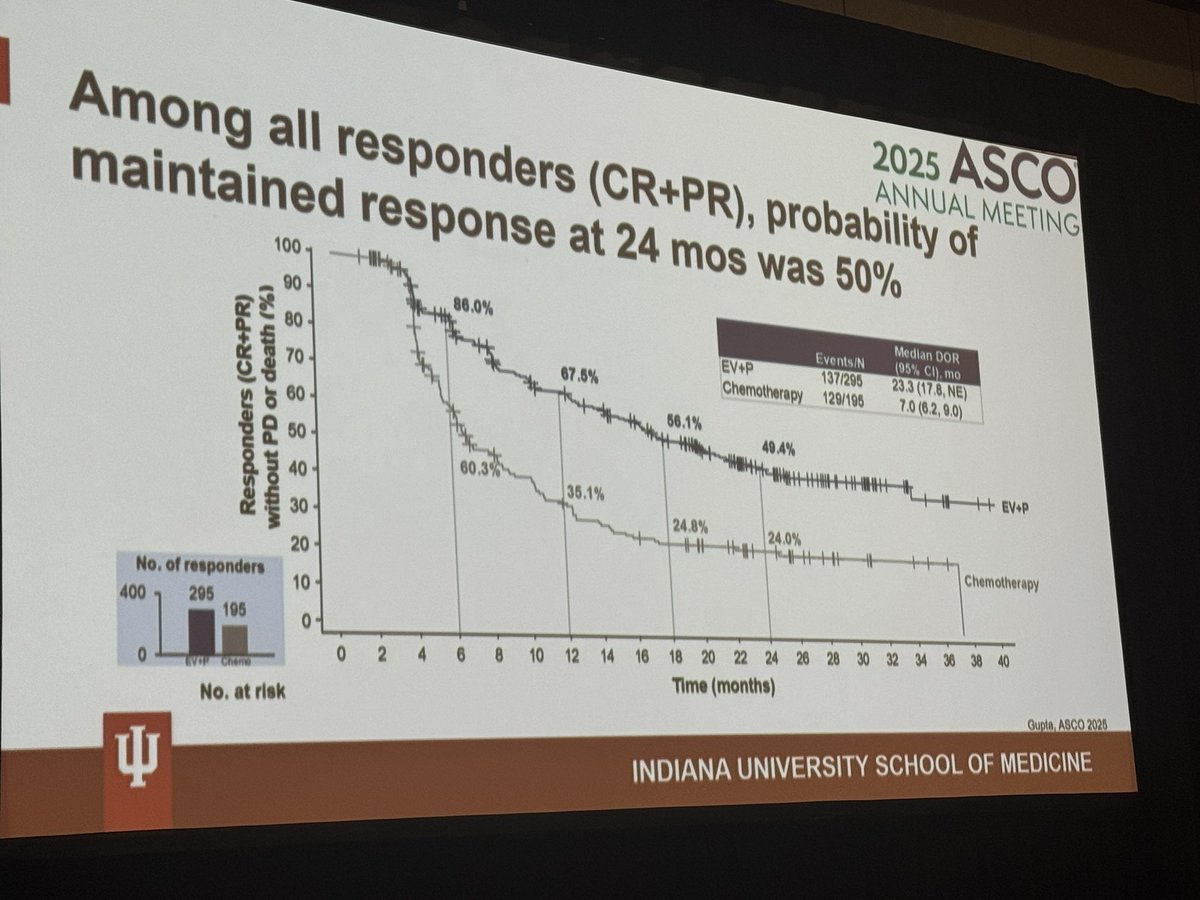
Dr Jennifer King with bladder cancer updates: NIAGARA shows perioperative durvalumab improves EFS regardless of pCR/ctDNA status. EV-302 demonstrates 50% maintained response at 24 months among…
TROPiCS-04 is the archetype of an accelerated-approval confirmation trial failure leading to voluntary withdrawal. The prior accelerated approval (April 2021) was based on TROPHY-U-01 ORR data. When TROPiCS-04 missed OS (and showed higher early mortality from neutropenic complications), Gilead withdrew the indication. Sacituzumab govitecan remains approved for metastatic TNBC and HR+/HER2- breast cancer. The mUC treatment landscape has since shifted decisively toward EV-302 (enfortumab vedotin + pembrolizumab) as 1L SOC.
TROPiCS-04 did NOT meet its primary endpoint of overall survival in the ITT population. A numerical OS improvement favoring sacituzumab govitecan was observed, along with trends in secondary endpoints (PFS, ORR) and prespecified subgroups, but these were not alpha-controlled for formal statistical testing. Exact OS medians, HR, and CI not disclosed in topline release. 711 patients randomized 1:1 to sacituzumab govitecan 10 mg/kg on days 1 and 8 of 21-day cycle vs. physician's choice chemotherapy (paclitaxel, docetaxel, or vinflunine).
Primary endpoint was OS (see above). No statistically significant OS benefit.
Higher number of deaths due to adverse events with sacituzumab govitecan vs. chemotherapy — primarily early in treatment and related to neutropenic complications including infection. No new safety signals beyond known Trodelvy profile (severe/life-threatening neutropenia per Boxed Warning; diarrhea). Gilead emphasized G-CSF use for prevention of neutropenic complications.
❌ Negative Phase 3; accelerated approval voluntarily withdrawn. No longer available for urothelial cancer. TROPiCS-04 is the archetype of an accelerated-approval confirmation trial failure leading to voluntary withdrawal. The prior accelerated approval (April 2021) was based on TROPHY-U-01 ORR data. When TROPiCS-04 missed OS (and showed higher early mortality from neutropenic complications), Gilead withdrew the indication. Sacituzumab govitecan remains approved for metastatic TNBC and HR+/HER2- breast cancer. The mUC treatment landscape has since shifted decisively toward EV-302 (enfortumab vedotin + pembrolizumab) as 1L SOC.
TROPiCS-04 (NCT04527991) is a Phase 3, randomized confirmatory trial of the TROP-2-directed antibody-drug conjugate sacituzumab govitecan (Trodelvy) versus physician's choice of chemotherapy in patients with pretreated locally advanced or metastatic urothelial (bladder) cancer that progressed after platinum-based chemotherapy and a checkpoint inhibitor. It was sponsored by Gilead Sciences.
No. TROPiCS-04 did not meet its primary endpoint of overall survival in the intent-to-treat population. A numerical trend and some secondary and subgroup signals favored sacituzumab govitecan, but these were not statistically controlled. There were also more deaths due to adverse events with sacituzumab govitecan, concentrated early in treatment and related to neutropenic complications.
No. Following the negative TROPiCS-04 result, the U.S. urothelial accelerated approval — granted in April 2021 based on TROPHY-U-01 objective-response data — was voluntarily withdrawn, and sacituzumab govitecan is no longer available for bladder cancer. Its breast cancer indications remain in place.
Trodelvy remains FDA approved in breast cancer — for metastatic triple-negative breast cancer and for HR-positive/HER2-negative metastatic breast cancer. Only the urothelial (bladder) cancer indication was withdrawn; the TROPiCS-04 failure does not affect the breast cancer approvals.
TROPiCS-04 is a textbook example of an accelerated-approval confirmatory trial that failed, triggering voluntary withdrawal of the indication. The accelerated approval had rested on objective-response data from TROPHY-U-01; when the confirmatory Phase 3 missed overall survival and showed higher early mortality, the benefit-risk no longer supported the urothelial indication.
