EGFR-mutant NSCLC (post-3rd gen TKI + platinum chemo) and HR+/HER2- breast cancer (post-CDK4/6i) — MediLink Therapeutics (Suzhou, China) + BioNTech (co-development license Oct 2023)
Discover KOL Sentiment on YL202 →Design - Phase 1 first-in-human dose-escalation/expansion of YL202/BNT326, a HER3-directed antibody-drug conjugate (topoisomerase I payload; MediLink Therapeutics + BioNTech) in post-TKI EGFR-mutant NSCLC and post-CDK4/6i HR+/HER2- breast cancer (NCT05653752).
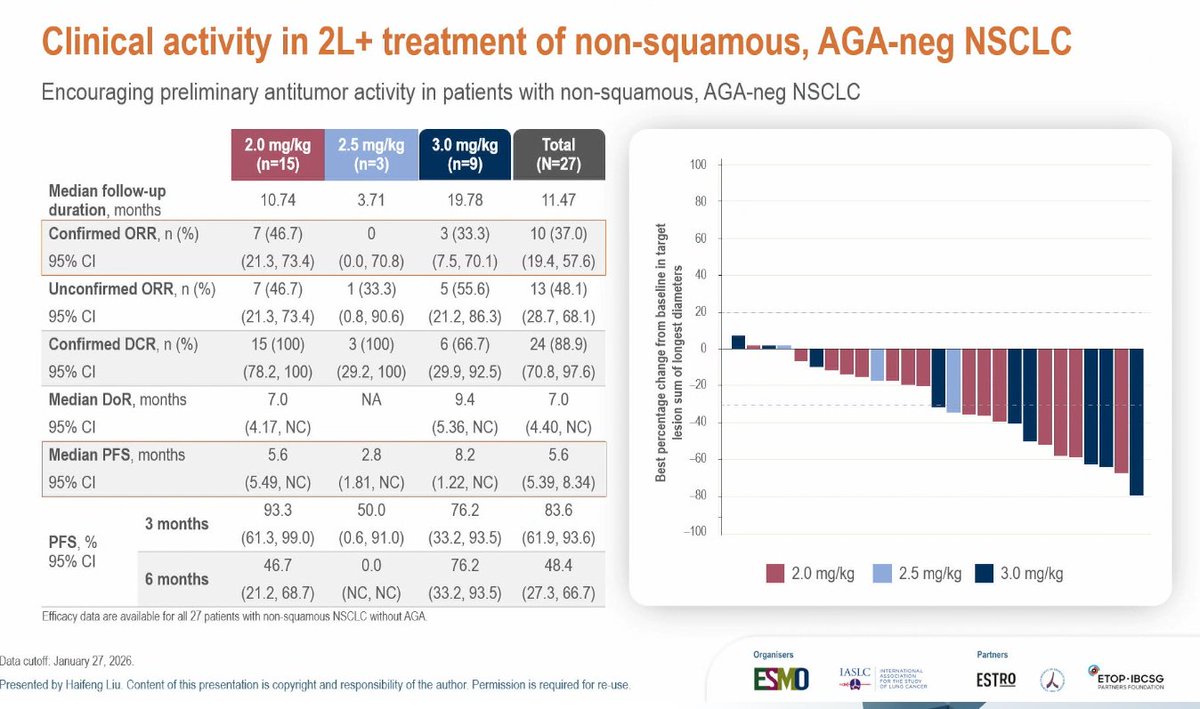
Response (all evaluable, N=46) - ORR 37.0%, disease control rate 93.5%, median duration of response 8.4 months, 6-month PFS 61.6%.
Response (DL3-DL5, N=39) - ORR 41.0% (95% CI 25.6-57.9), disease control rate 94.9%.
Breast cancer subset - Heavily pretreated HR+/HER2- breast cancer ORR 54.5% - a strong early signal.
Safety - Common grade >=3 events were hematologic (anemia, decreased white cells/neutrophils); one interstitial lung disease case was reported. Mature PFS/OS not reported (Phase 1).
Regulatory / sponsor - Investigational; not FDA approved. MediLink Therapeutics (China) + BioNTech (co-development).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.











Top tweets by impressions — click to view on X
🆙 #ELCC26 @myESMO 🇩🇰
🔥Mini Oral session 2
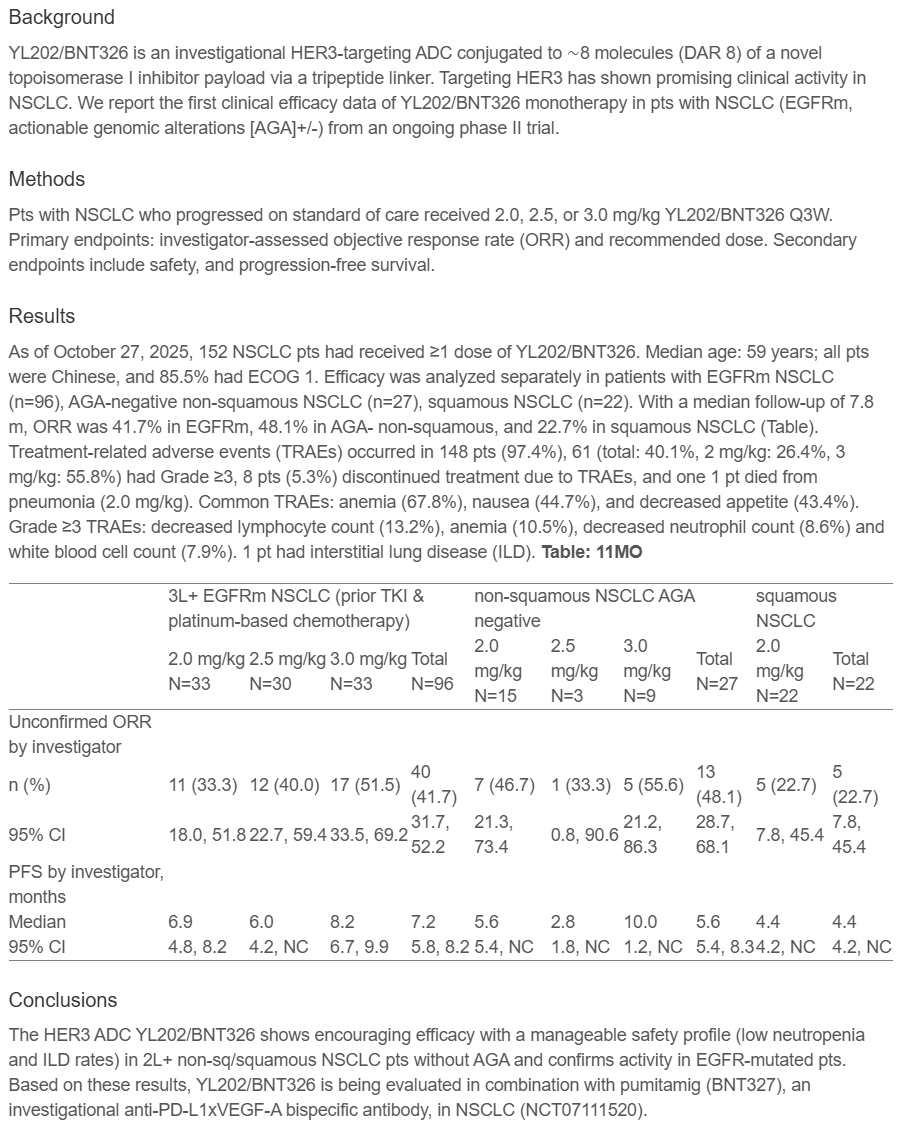
☑️YL202/BNT326: HER3 ADC
🎯ORR across doses: 22.7-55.6%
🎯mPFS across doses: 2.8-10.0m
🎙️Dr. Haifeng Liu
🎙️Chair: Dr. Kersti Oselin…
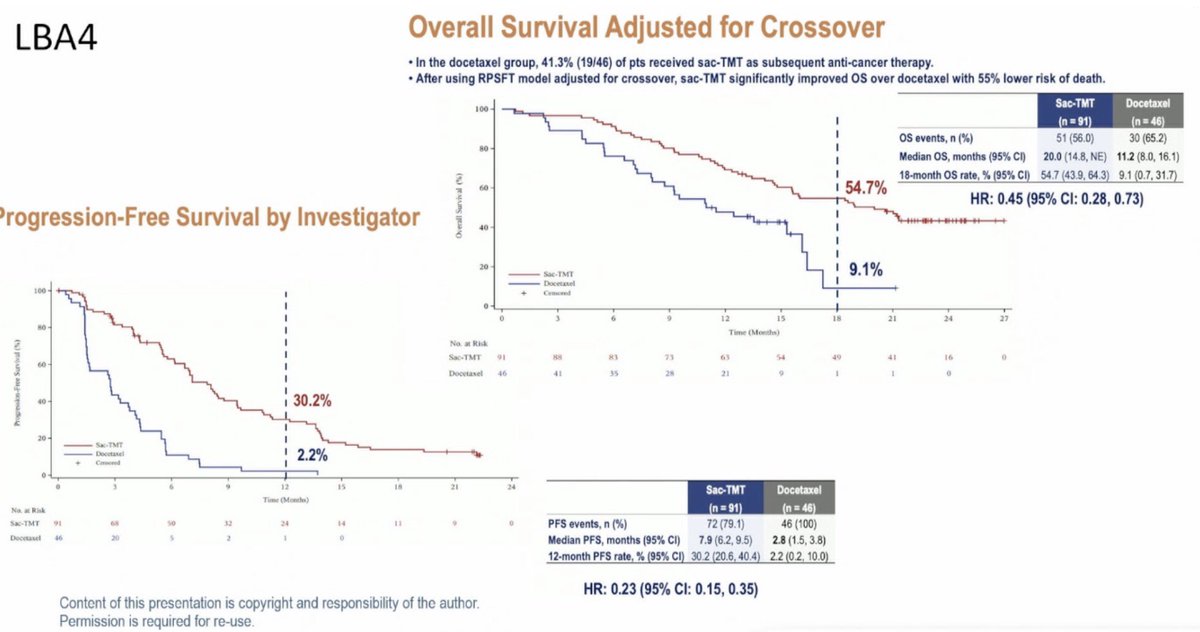
Great EGFR-mutant NSCLC session. Impressed by the Sac-TMT results (anti-TROP2 ADC), which show the most positive outcomes across two Chinese studies. Other ADCs are also in the pipeline, things are…
🔥 HER3 ADC enters the NSCLC space #ELCC26
First efficacy data of YL202/BNT326 in heavily pretreated NSCLC 👇
🧬 Study population
• ≥3L NSCLC post TKI + platinum
• EGFRm (n=96) | AGA– non-sq (n=27) |…
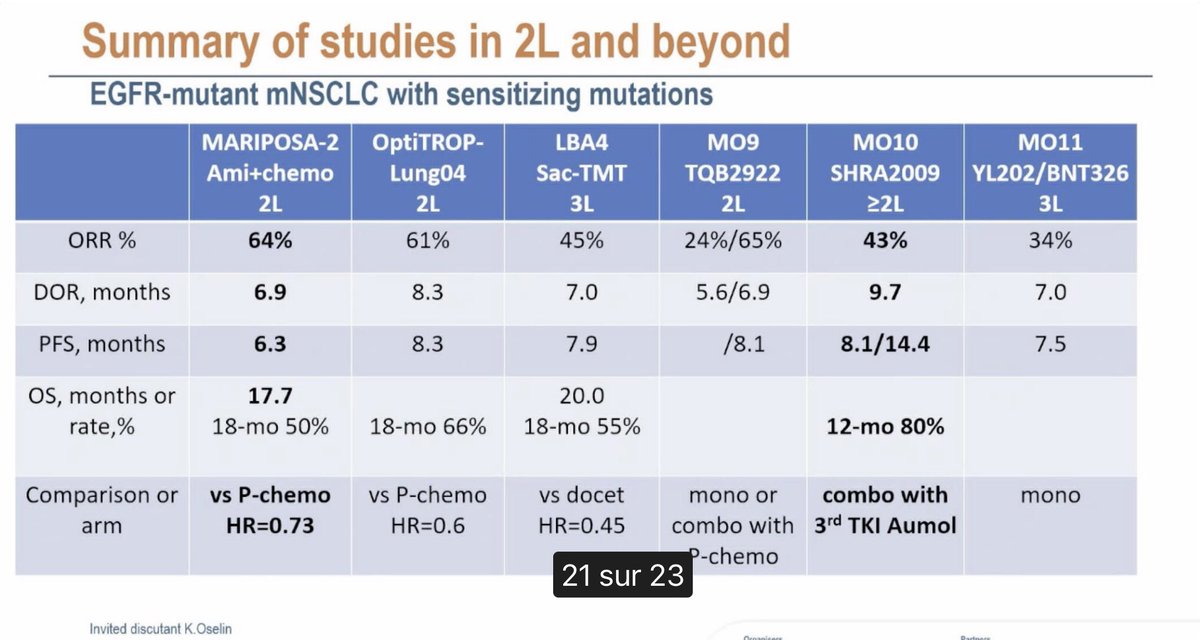
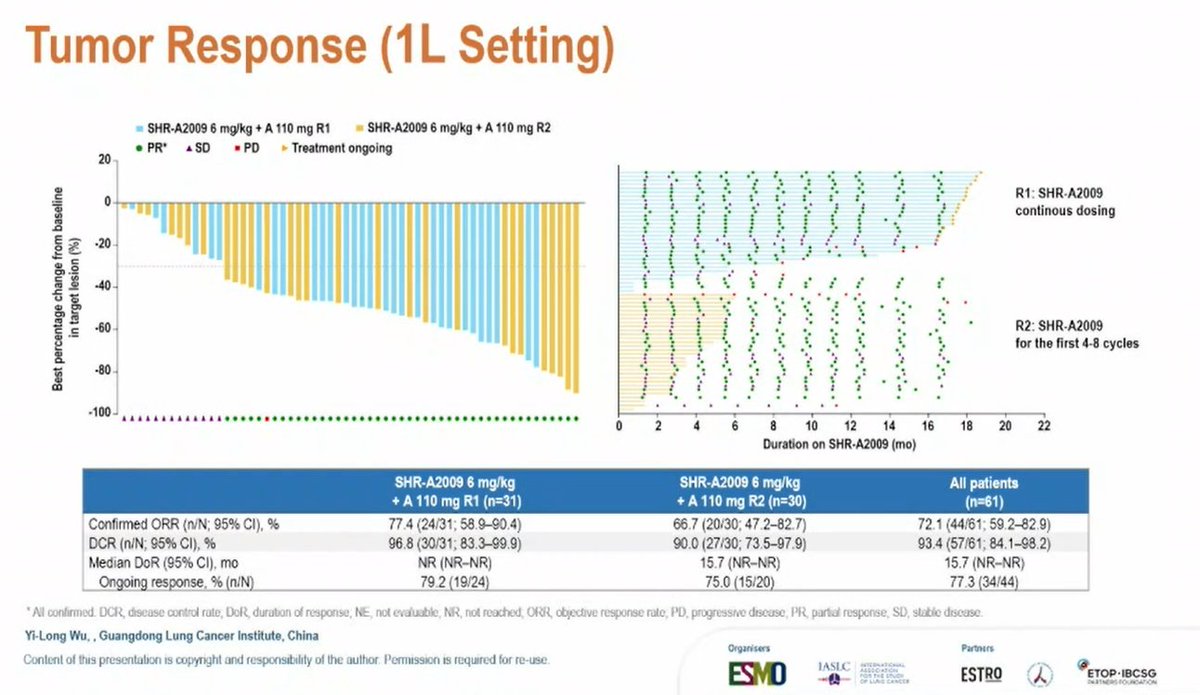
✨ Mini oral session 2 at #ELCC26: SHR-A2009 (HER3 ADC) + aumolertinib in EGFRm NSCLC (Ph1b/2)
🎯 ORR: 72.1% (1L) | 42.9% (≥2L)
📈 Durable responses (DoR up to 15.7 mo)
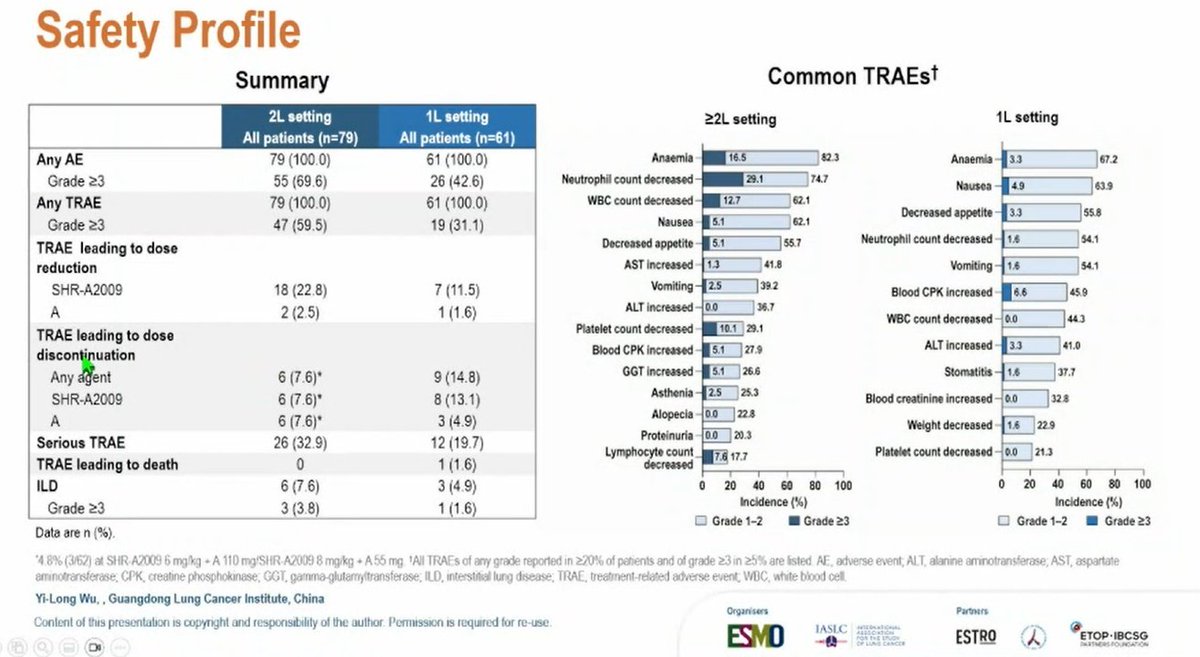
⚠️ TRAE G≥3: 31.1% (1L) | 59.5%…
✨ Mini oral session 2 at #ELCC26: YL202/BNT326 (HER3 ADC) in NSCLC with EGFRm (cohort A2) and squamous NSCLC (cohort E1) (Ph2)
🎯 ORR 34.4%/mPFS 7.5-8.1 mo (EGFRm ≥3L)
👍 Manageable safety, low…
YL202/BNT326 is MediLink Therapeutics' (China) + BioNTech's HER3-directed ADC, structurally analogous to Daiichi Sankyo's patritumab deruxtecan (HER3-DXd). Phase 1 first-in-human (N=52): encouraging ORR 41% in DL3-5 (54.5% in heavily pretreated HR+/HER2- BC), DCR 93.5% across all, low ILD rate (1 case after COVID). Directly competes with HER3-DXd which HERTHENA-Lung01 failed to achieve FDA approval in EGFR NSCLC (Daiichi withdrew application 2024) — YL202/BNT326 may face similar regulatory headwinds in this line/biomarker context. Clinical value depends on Phase 2/3 confirmation.
All evaluable (N=46) rate: 37.0% (ORR %) vs. 93.5% (DCR %) vs. 8.4% (mDOR months) vs. 61.6% (6-mo PFS %). DL3-DL5 dose range (N=39) rate: 41.0% (ORR %) vs. 25.6-57.9% (95% CI) vs. 94.9% (DCR %) vs. 82.7-99.4% (95% CI DCR). Breast cancer subset (n=13) rate: 54.5% (ORR %) vs. 23.4-83.3% (95% CI) vs. 100% (DCR %) vs. 71.5-100% (95% CI DCR). Phase 1 first-in-human, open-label, multinational trial. HER3-targeted ADC: anti-HER3 IgG1 mAb + 8 molecules YL0010014 (novel topo-I inhibitor) via tripeptide linker. N=52 enrolled (39 NSCLC, 13 BC). Dose escalation: 6 dose levels Q3W with BOIN design + cohort backfill. Population: EGFR-mutant NSCLC post-3rd gen TKI + platinum chemo; HR+/HER2- mBC post-CDK4/6i + ≥1 chemo (median 4 prior lines, range 2-8). Primary endpoints: safety/tolerability (DLTs, AEs). DLT: 1 Grade 3 febrile neutropenia at highest dose (DL6). ORR all evaluable (N=46) 37.0% (95% CI 23.2-52.5); DCR 93.5% (95% CI 82.1-98.6); mDOR 8.4 months. DL3-DL5 dose range: ORR 41.0% across all tumor types; BC subset ORR 54.5%, DCR 100%. 6-month PFS 61.6%. Zhang et al., JCO 2024;42(16)_suppl:3034.
Phase 1 — mature PFS/OS not reported. Strong signal in BC (54.5% ORR heavily pretreated) supports further Phase 2/3 development. Safety generally manageable.
Key AEs: anemia (71% all-grade, 20% G≥3), WBC decreased (67% all-grade, 31% G≥3), neutrophil decreased (63% all-grade, 29% G≥3), nausea (52%), decreased appetite (42%), lymphocyte decreased (37% all-grade, 23% G≥3), thrombocytopenia (37% all-grade, 10% G≥3), vomiting, dry mouth, fatigue, stomatitis, alopecia. Interstitial pneumonia in 1 patient (2%, after COVID-19 infection) — notable given class risk of topoisomerase-I ADCs. PK exposure increased with dose escalation; low systemic payload exposure; no accumulation upon repeated administration. Hematologic toxicity predominant; non-heme TRAEs largely low-grade.
🔬 Phase 1 signal: MediLink/BioNTech HER3 ADC active in post-TKI EGFR NSCLC + HR+/HER2- BC. YL202/BNT326 is MediLink Therapeutics' (China) + BioNTech's HER3-directed ADC, structurally analogous to Daiichi Sankyo's patritumab deruxtecan (HER3-DXd). Phase 1 first-in-human (N=52): encouraging ORR 41% in DL3-5 (54.5% in heavily pretreated HR+/HER2- BC), DCR 93.5% across all, low ILD rate (1 case after COVID). Directly competes with HER3-DXd which HERTHENA-Lung01 failed to achieve FDA approval in EGFR NSCLC (Daiichi withdrew application 2024) — YL202/BNT326 may face similar regulatory headwinds in this line/biomarker context. Clinical value depends on Phase 2/3 confirmation.
YL202/BNT326 is an investigational HER3-directed antibody-drug conjugate that links an anti-HER3 antibody to a topoisomerase I inhibitor payload. It is being developed by MediLink Therapeutics (Suzhou, China) and BioNTech, and is structurally analogous to other HER3-directed ADCs such as patritumab deruxtecan (HER3-DXd).
In the Phase 1 first-in-human study (NCT05653752), the objective response rate was 37.0% across all evaluable patients (N=46) and 41.0% in the DL3-DL5 dose range (N=39), with disease control rates above 93%. In a heavily pretreated HR-positive/HER2-negative breast cancer subset, the response rate was 54.5%. Mature progression-free and overall survival were not reported at this early stage.
No. YL202/BNT326 is investigational and in Phase 1 first-in-human development; it is not FDA approved. Its results are early signals that would need confirmation in later-phase trials, particularly given that the related HER3 ADC patritumab deruxtecan did not achieve FDA approval in EGFR-mutant NSCLC.
The Phase 1 study enrolled patients with EGFR-mutant NSCLC whose disease had progressed after a third-generation EGFR TKI plus platinum-based chemotherapy, and patients with HR-positive/HER2-negative breast cancer after a CDK4/6 inhibitor - both heavily pretreated populations with limited options.
The most common higher-grade adverse events were hematologic, including anemia, decreased white blood cells and neutrophils; nausea and decreased appetite were also frequent. One case of interstitial lung disease was reported, a class-relevant risk for antibody-drug conjugates that warrants monitoring. Safety was described as generally manageable in the Phase 1 setting.