Transplant-ineligible newly diagnosed multiple myeloma (TI NDMM) — GSK
Visit Interactive Trial Page →







Top tweets by impressions — click to view on X
DREAMM-9 results are in!
Would anyone (other than an ophthamologist) consider using belantamab-VRd as an induction for patients with multiple myeloma not eligible for ASCT?
I have said this…
#ASH24 excellent presentation by @szusmani of Bela-VRd in frontline ASCT-ineligible #MMsm.
Trick is to space out the dose frequency as keratopathy develops - pretty nice rates of MRD…
Great Presentation, thank you @szusmani - Abstract #497 looking forward to "Bela is Back" #ASH24 #IMFASH24 #MMsm
Phase I Study of Belantamab Mafodotin in Combo with Standard of Care in…
Abstract 497: Phase 1 Bela in combo with SOC transplant ineligible NDMM-Dreamm-9 Updated Interim Analysis @szusmani @TerryGlassman #ASH24 #IMFASH24 #MMsm https://t.co/hBJsBFQzlt
Frontline bela for ND TIE MM? Courageous study but interesting results. With bela dose adjustmemts rate of dfiscontinuation low and responses are deep. A new fight is brewing between QUADs (PN!),…
#ASH24 and the most important slide of DREAMM-9 by @szusmani with Bela-VRd in frontline myeloma #MMsm.
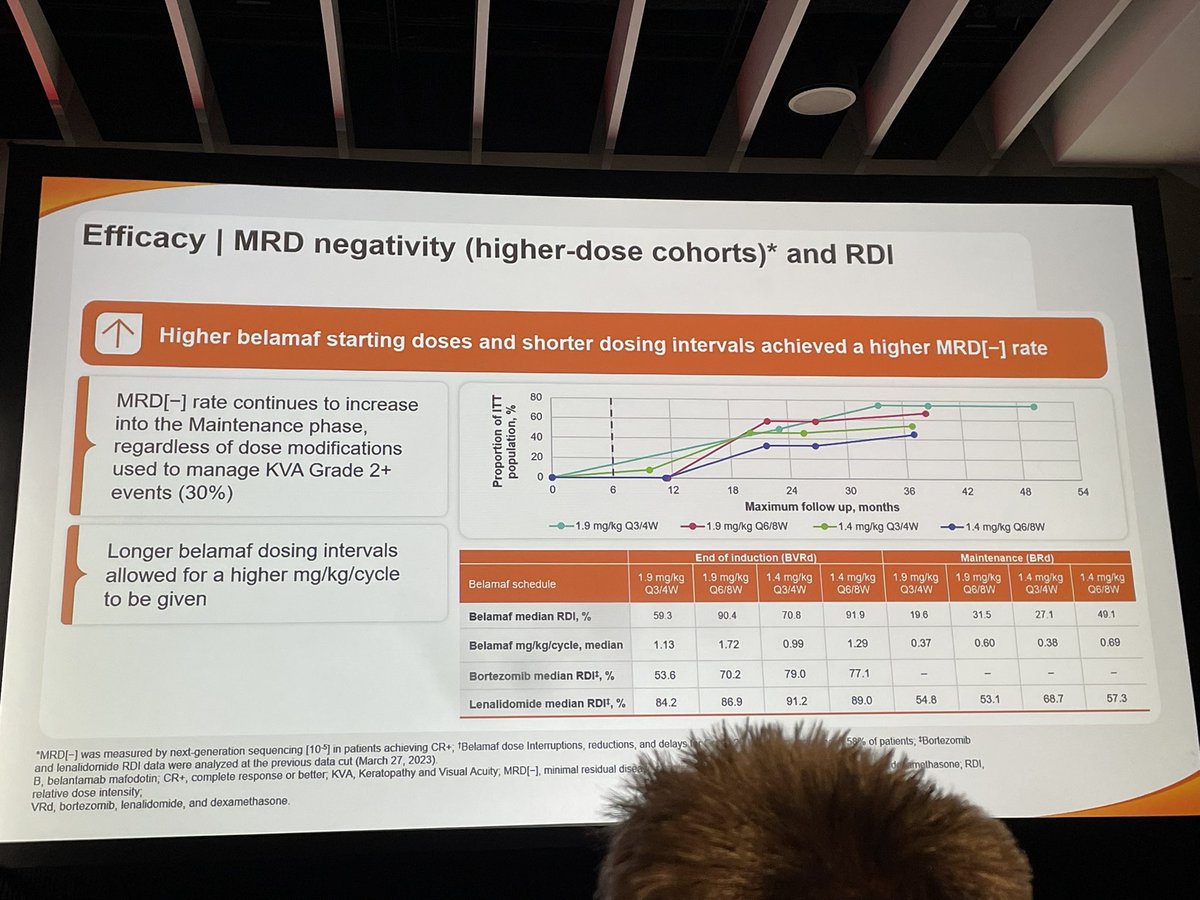
MRD rates improve over time, even in patients where belantamab is held for toxicities! Maybe…
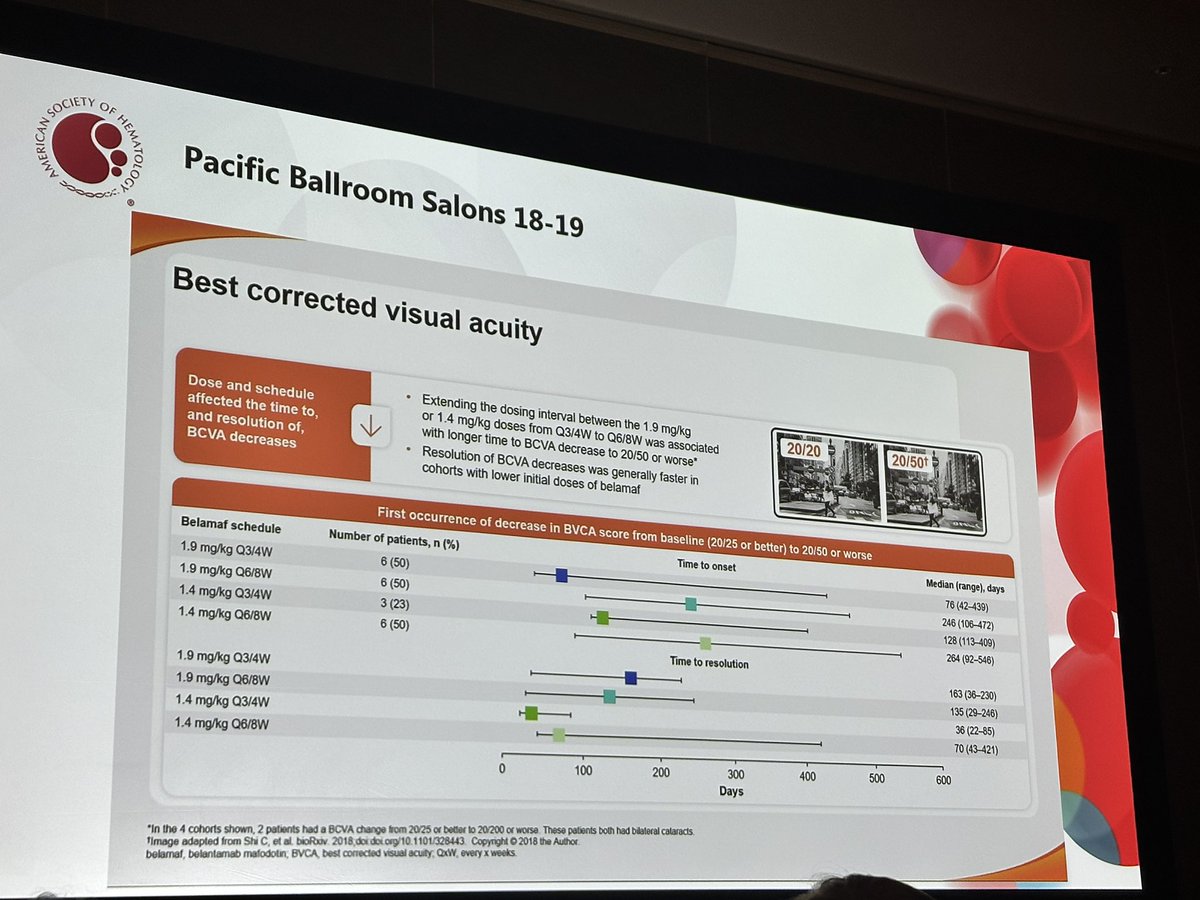
DREAMM-9: Belamaf - VRd for 1st line TNE myeloma. Very interesting data on spacing out frequency of Belamaf to reduce ocular toxicity but achieving high responses and gradual MRD negativity rates.…
🧵The DREAMM-9 study tests belantamab mafodotin + VRd in newly diagnosed myeloma patients ineligible for ASCT. Higher doses boost MRD negativity, with a favorable safety profile despite ocular events.…

#ASH24 #mmsm @ASH_hematology
Oral myeloma: Dreamm-9
Higher doses of Blenrep better responses and worse AEs (eye issues and thrombocytopenia)
Lower doses of Blenrep lower responses and better AEs…

@szusmani on Belamaf in combo w RVD for TI NDMM, several dosing and frequency cohorts.
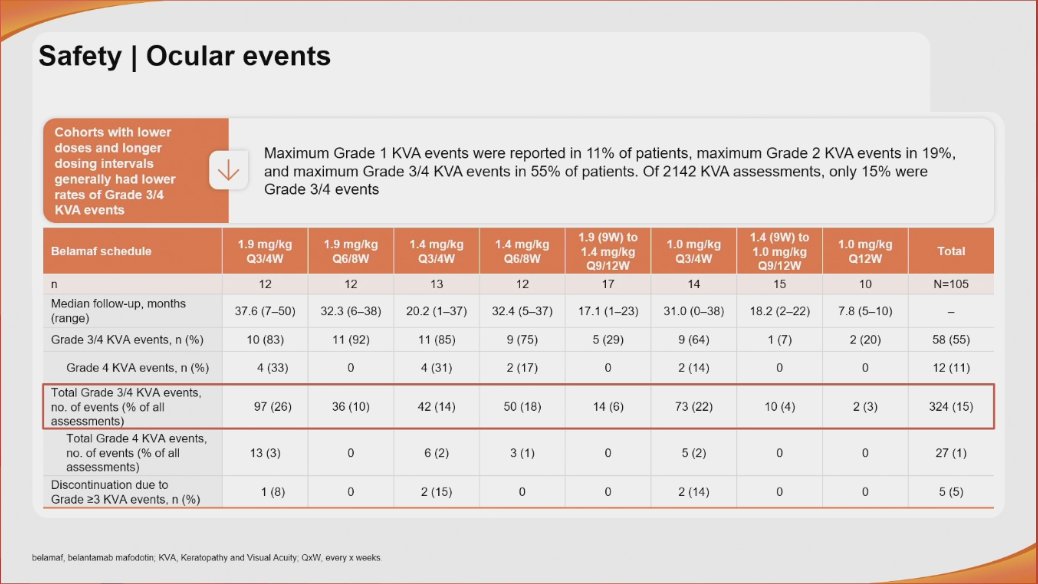
G3+ KVA 50%, Lower and less frequent dosing delays onset and improves recovery of KVA; deeper & faster MRD…
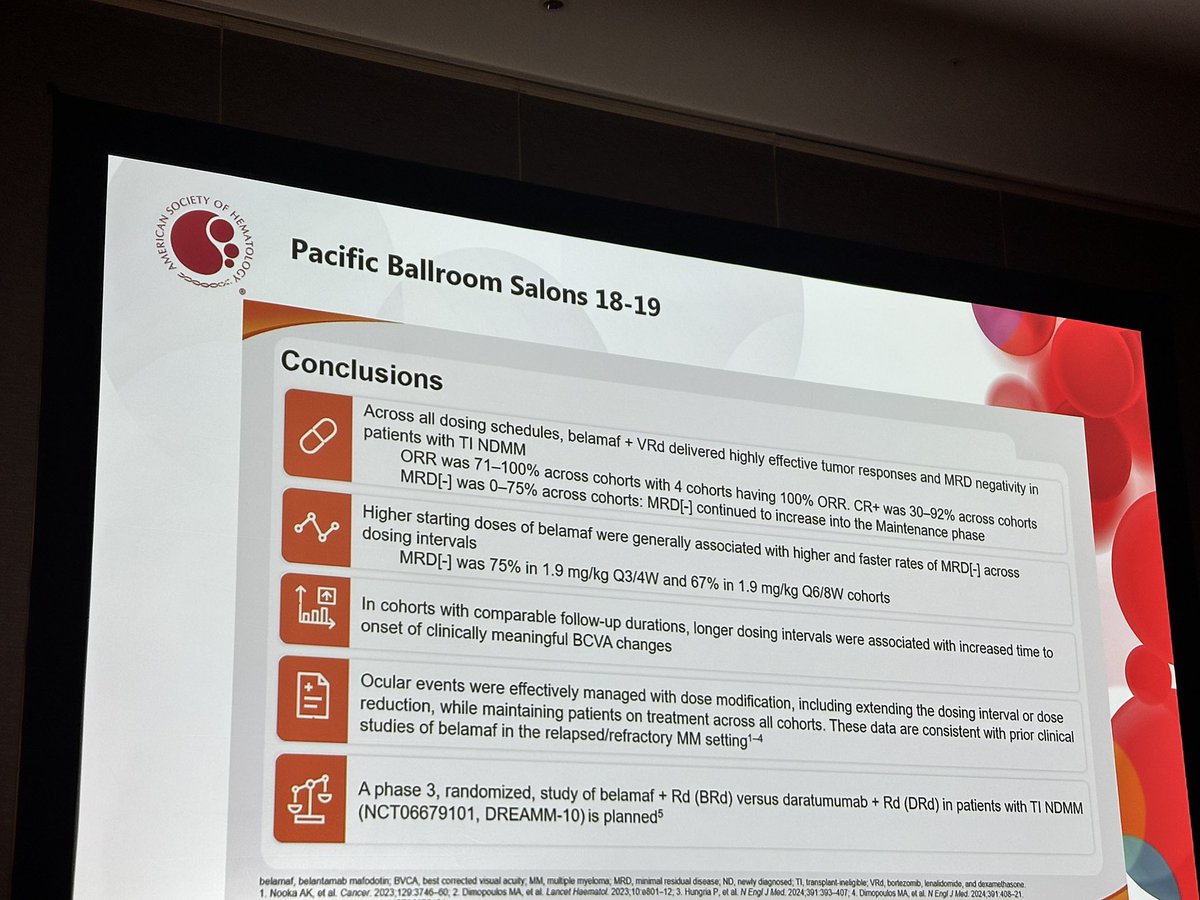
DREAMM-9 provides dose/schedule optimization data for belantamab + VRd in TI NDMM. High response rates and MRD negativity are encouraging but Phase 1 design precludes practice-changing conclusions. Belantamab mafodotin returned to the U.S. market in RRMM combinations (DREAMM-7 FDA approval July 2025 — belamaf + BVd). Ocular toxicity (keratopathy) remains the defining class challenge; DREAMM-9 cohorts explore lower doses / longer intervals to mitigate.
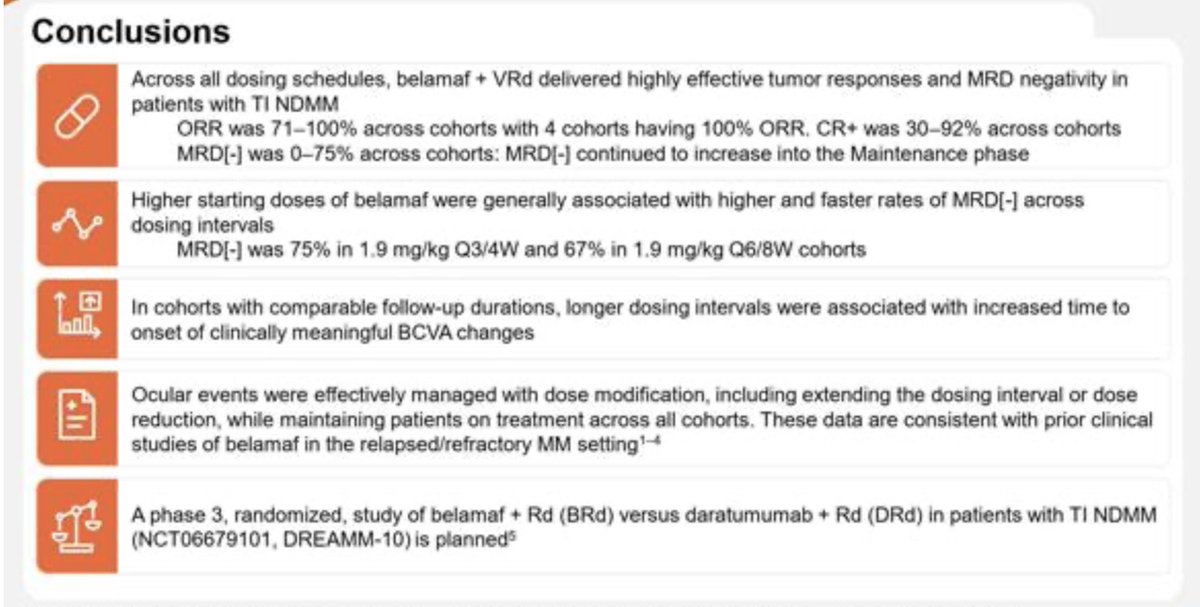
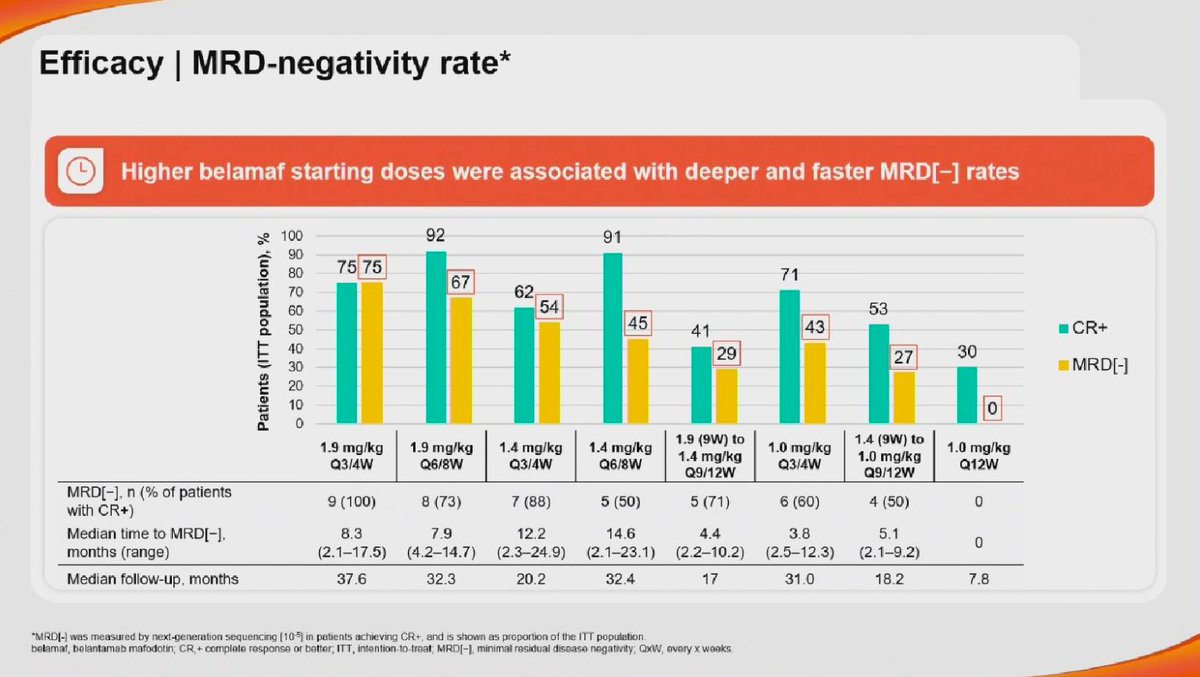
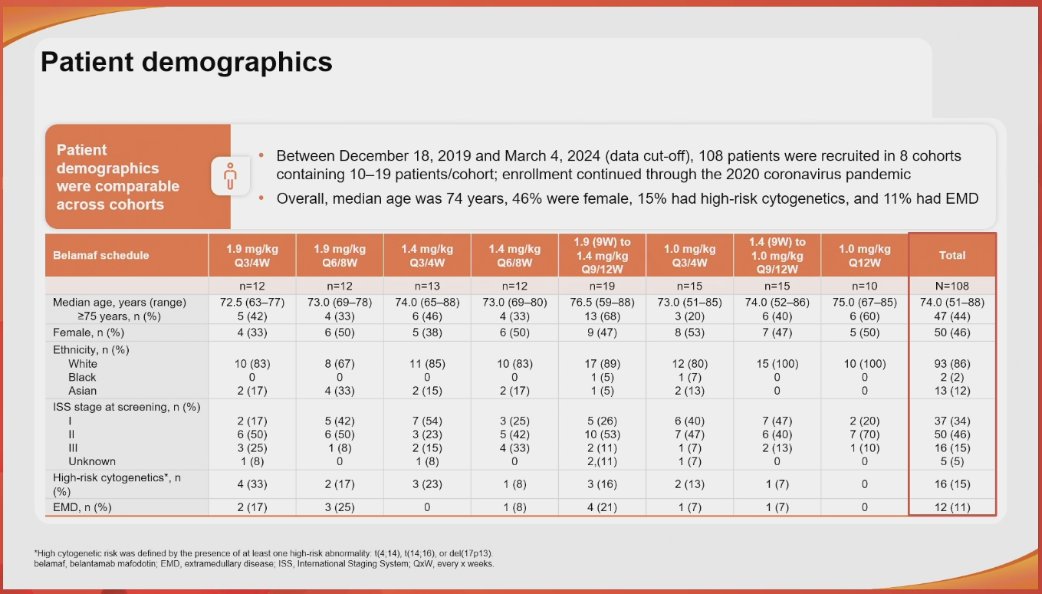
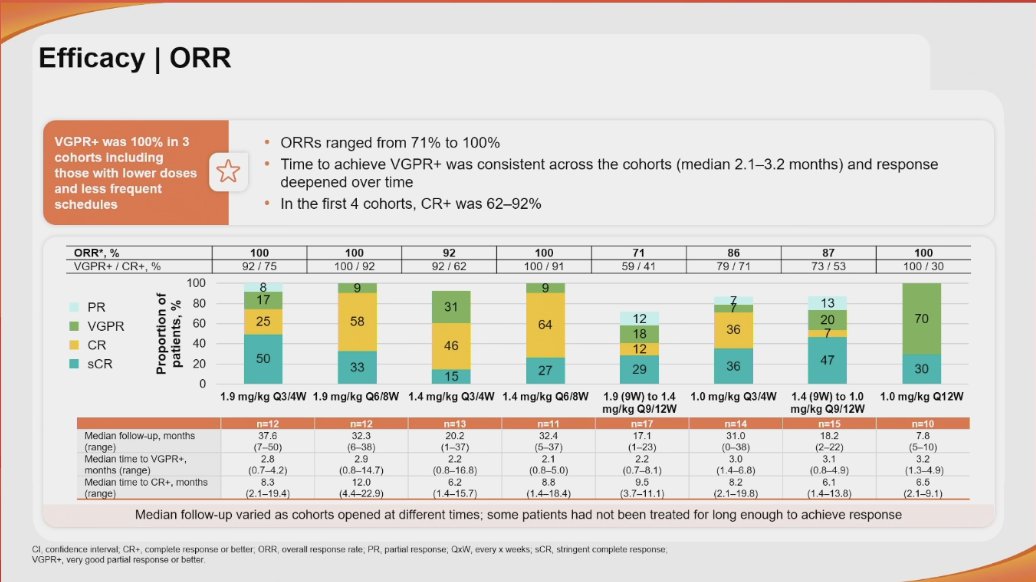
Phase 1 dose-optimization study (N=108) across 8 cohorts of belantamab mafodotin dose/schedule combined with VRd. Primary endpoints are DLTs and AEs — no PFS/OS comparison yet. Best response rates (ORR) ranged from 71-100% across cohorts. ≥VGPR rate was 100% in three cohorts, including lower-dose/less-frequent schedules. ≥CR rates in cohorts 1-4 ranged from 62-92% with responses deepening over time. Higher starting doses associated with deeper, faster MRD negativity; in Cohort 1, 100% of patients with CR achieved MRD negativity. No randomized comparator — response rates are single-arm.
Key AEs: thrombocytopenia (30% Grade 3/4), neutropenia (26% Grade 3/4), COVID-19 pneumonia (14% Grade 3/4), ocular / keratopathy (class effect of belantamab — specific rates not in published sources). Belantamab-related Grade 3/4 AEs in 33% of 105 safety-evaluable patients overall. Lower doses and longer intervals associated with lower Grade 3/4 AE rates. Most frequent non-ocular Grade 3/4 AEs: thrombocytopenia (30%), neutropenia (26%), COVID-19 pneumonia (14%). Ocular/keratopathy AEs (hallmark belantamab toxicity) not quantified in available summary sources. Discontinuation rates not reported.
🔬 Phase 1 dose optimization — investigational; not for clinical use in TI NDMM. DREAMM-9 provides dose/schedule optimization data for belantamab + VRd in TI NDMM. High response rates and MRD negativity are encouraging but Phase 1 design precludes practice-changing conclusions. Belantamab mafodotin returned to the U.S. market in RRMM combinations (DREAMM-7 FDA approval July 2025 — belamaf + BVd). Ocular toxicity (keratopathy) remains the defining class challenge; DREAMM-9 cohorts explore lower doses / longer intervals to mitigate.