Relapsed/refractory MM · ≥1 prior line · BVd vs DVd · GSK
Discover KOL Sentiment on DREAMM-7 →Design — Phase 3; BVd (belantamab mafodotin + bortezomib + dex) vs DVd (daratumumab + bortezomib + dex) in R/R multiple myeloma (NCT04246047). (NEJM 2024 / FDA label)
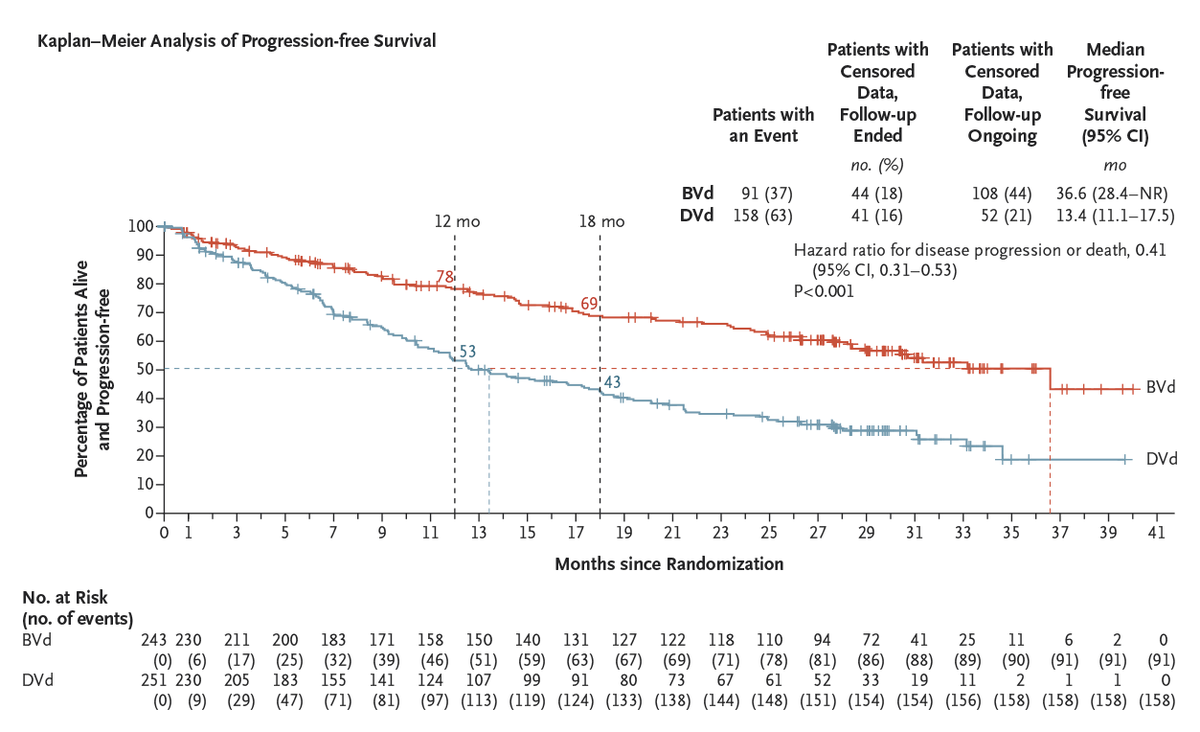
PFS — ITT (≥1 prior line): 36.6 vs 13.4 mo, HR 0.41, p<0.00001. FDA population (≥2 prior lines): 31.3 vs 10.4 mo, HR 0.31. (ITT: NEJM/ASCO; FDA pop: FDA label)
OS — ITT: 42% risk-of-death reduction, HR 0.58 (95% CI 0.43-0.79; p=0.00023), median not reached; FDA population OS HR 0.49. (ASH 2024 / FDA label)
Safety — Ocular toxicity (keratopathy/visual changes) in 92% of BVd patients, 77% Grade 3/4; boxed warning. Grade 3+ AEs 95%. (FDA label / DREAMM-7)
Regulatory — FDA approved Oct 23, 2025 for R/R MM after ≥2 prior lines incl. PI+IMiD. The DREAMM-8 BPd regimen was NOT US-approved. (FDA.gov)
Sponsor / Drug — GSK; belantamab mafodotin (Blenrep), a BCMA-directed antibody-drug conjugate, 2.5 mg/kg IV every 3 weeks. (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 20, 2026.









Top 10 by impressions - click to view on X
Original Article: Belantamab Mafodotin, Bortezomib, and Dexamethasone for Multiple Myeloma (DREAMM-7) #ASCO24 | @ASCO
🚨 Out now DREAMM-7 from NEJM BVd vs DVd @NEJM Full disclosure: I am a co-author 🧵 BVd vs DVd in early relapse myeloma: N=494 (BVd, n=243; DVd, n=251) Median follow-up 28.2 months Median...
The comparison of two manuscripts @NEJM showcasing Belantamab's superiority over other anti-myeloma treatments in a head-to-head comparison is widely considered the...
Shocker for me. ODAC votes against belantamab risk benefit for myeloma. I hope that this vote reflects the way the questions were narrowly worded. I still hope the drug still gets FDA approved.
Should give credit where its due The trial design of DREAMM-7 was bold, a head-to-head trial comparison against dara, a great drug. The control arm was ethical during the period of enrollment....
So the belantamab ODAC is on. Personally I hope the belantamab is approved for relapsed myeloma. It has many advantages and there is a unique need for the drug in relapsed refractory myeloma. If...
Looking forward to the #ASCO24! Here are the lists for five #mmsm abstracts for @OncoAlert: 1- DREAMM-8 belantamab plus pomalidomide/dex (BPd) vs PVd in...
1/ Late to #ASCO24 while on inpatient, and others have already excellently summarized our field's excitement around belantamab's comeback...

#Myeloma Paper of the Day: DREAMM-7 study shows belantamab/bortez/dex superior to dara/bortez/dex in RRMM w/ 1+ prior line, w/ median PFS 36.6 (vs. 13.4) months, OS @ 18 months 84%...

Myeloma is full of surprises: EXHIBIT A: Canova EXHIBIT B: DreaMM studies #EHA24RF #mmsm
DREAMM-7 is a pivotal Phase III, open-label, randomized trial that established belantamab mafodotin (Blenrep) in combination with bortezomib and dexamethasone (BVd) as a potent new option for patients with relapsed or refractory multiple myeloma after at least one prior line of therapy. The trial randomized 494 patients 1:1 to BVd versus daratumumab plus bortezomib and dexamethasone (DVd), demonstrating a 59% reduction in the risk of disease progression or death and a 42% reduction in the risk of death favoring BVd. Despite an ODAC vote of 5-3 against the proposed dosage due to ocular toxicity concerns, the FDA approved belantamab mafodotin in October 2025 based on the strength of efficacy data. DREAMM-7 results were published in the New England Journal of Medicine (Hungria et al., 2024) with an updated OS analysis in Lancet Oncology (2025).
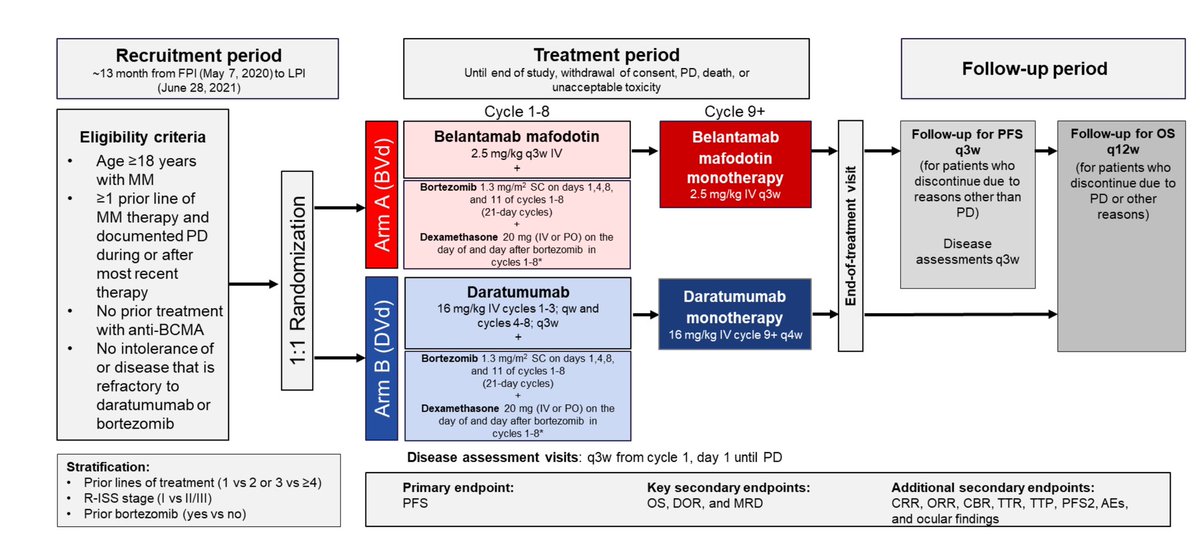
Phase III, global, multicenter, open-label, 1:1 randomized trial at 142 study centers in 20 countries comparing BVd versus DVd in patients with RRMM and at least 1 prior line of therapy. Belantamab mafodotin was dosed at 2.5 mg/kg IV every 3 weeks; bortezomib 1.3 mg/m2 SC twice weekly in 21-day cycles for up to 8 cycles. BCMA-targeted therapy-naive population required; anti-CD38 refractory patients excluded.
Adults aged 18+ with confirmed multiple myeloma per IMWG criteria, ECOG PS 0-2, documented disease progression on or after at least 1 prior line of therapy. Prior BCMA-directed therapy was not permitted. Patients with disease refractory to anti-CD38 therapy were excluded. 51% had received 1 prior line, 34% were lenalidomide-refractory, 28% had high-risk cytogenetic abnormalities. Median age 64.5 years.
BVd arm: belantamab mafodotin 2.5 mg/kg IV every 3 weeks + bortezomib 1.3 mg/m2 SC (days 1, 4, 8, 11 of 21-day cycles for up to 8 cycles) + dexamethasone 20 mg. DVd arm: daratumumab 16 mg/kg IV (weekly cycles 1-3, every 3 weeks cycles 4-8, every 4 weeks from cycle 9) + same bortezomib and dexamethasone schedule.
Primary endpoint: progression-free survival (PFS) by independent review committee. Key secondary endpoints: overall survival (OS), duration of response (DOR), minimal residual disease (MRD) negativity rate by next-generation sequencing. Other secondary endpoints: overall response rate (ORR), safety, patient-reported outcomes, PFS2.
At a median follow-up of 28.2 months, BVd demonstrated a median PFS of 36.6 months (95% CI: 28.4-NR) versus 13.4 months (95% CI: 11.1-17.5) with DVd (HR 0.41; 95% CI: 0.31-0.53; p<0.00001), representing a 59% reduction in the risk of progression or death. The FDA label analysis reported median PFS of 31.3 months (95% CI: 23.5-NR) versus 10.4 months (95% CI: 7-13.4) with HR 0.31 (95% CI: 0.21-0.47). PFS benefit was consistent across all prespecified subgroups including lenalidomide-refractory (HR 0.31) and high-risk cytogenetics (HR 0.31).
At a median follow-up of 39.4 months, the planned interim OS analysis demonstrated a statistically significant 42% reduction in the risk of death with BVd versus DVd (HR 0.58; 95% CI: 0.43-0.79; p=0.00023). Median OS was not reached in either arm; projected median OS was 84 months (BVd) versus 51 months (DVd). Three-year OS rates were 74% versus 60%. The survival benefit was observed as early as 4 months and was sustained over time. MRD negativity rate was 25.1% (BVd) versus 10.4% (DVd), with statistically significant superiority (p<0.00001).
Grade 3+ AEs occurred in 95% of BVd patients versus 78% with DVd. Ocular toxicity (keratopathy and visual acuity events) occurred in 92% of BVd patients, with 77% Grade 3/4; 76-83% required dose modifications for ocular toxicity. Clinically meaningful BCVA reductions to 20/50 or worse occurred in over 60% of patients. Grade 3+ thrombocytopenia (56%), neutropenia (14%), and anemia (9%) were the main hematologic toxicities. Despite high toxicity rates, treatment discontinuation due to ocular AEs was only 10%. The prescribing information includes a Boxed Warning for ocular toxicity risk.
Despite ODAC voting 5-3 against the proposed BVd dosage, the FDA approved Blenrep in October 2025 based on the substantial PFS and OS benefit. Key clinical debates center on whether dose optimization (lower doses or extended intervals) could reduce ocular toxicity while preserving efficacy, the real-world feasibility of rigorous ophthalmologic monitoring in community practice, and the relevance of trial data given the evolving US treatment landscape with frontline quadruplets, CAR-T, and bispecific antibodies. DREAMM-7 positions BVd as a potential new standard of care for RRMM at or after first relapse, particularly for BCMA-naive patients.
DREAMM-7 is a Phase 3 trial of belantamab mafodotin (Blenrep) + bortezomib + dexamethasone (BVd) versus daratumumab + bortezomib + dexamethasone (DVd) in adults with relapsed/refractory multiple myeloma who had received at least one prior line of therapy (NCT04246047).
Yes, for the BVd regimen. On October 23, 2025 the FDA approved Blenrep in combination with bortezomib and dexamethasone (BVd) for adults with relapsed/refractory multiple myeloma who have received at least two prior lines of therapy including a proteasome inhibitor and an immunomodulatory agent. The label carries a boxed warning for ocular toxicity.
In the intent-to-treat population, BVd nearly tripled median progression-free survival versus DVd (36.6 vs 13.4 months; HR 0.41; p<0.00001) and reduced the risk of death by 42% (OS HR 0.58; 95% CI 0.43-0.79; p=0.00023). In the FDA-approved population (≥2 prior lines), median PFS was 31.3 versus 10.4 months (HR 0.31) and the OS hazard ratio was 0.49.
Ocular toxicity. In DREAMM-7, corneal/visual-acuity events occurred in about 92% of BVd patients, with 77% Grade 3/4, and most required dose modification. Blenrep's label includes a boxed warning for ocular toxicity, including corneal changes that can cause vision deterioration.
DREAMM-7 tested the BVd regimen (belantamab + bortezomib + dexamethasone) and was FDA approved on October 23, 2025. DREAMM-8 tested a different regimen, BPd (belantamab + pomalidomide + dexamethasone); the FDA did NOT approve BPd in the US (ODAC voted 7-1 against it), although BPd is approved in several other countries.