R/R MM, ≥1 prior line (post-lenalidomide) · BPd vs PVd · GSK
Discover KOL Sentiment on DREAMM-8 →Design — Phase 3; BPd (belantamab mafodotin + pomalidomide + dex) vs PVd (bortezomib + pomalidomide + dex) in R/R multiple myeloma, ≥1 prior line incl. lenalidomide (NCT04484623). (NEJM 2024)
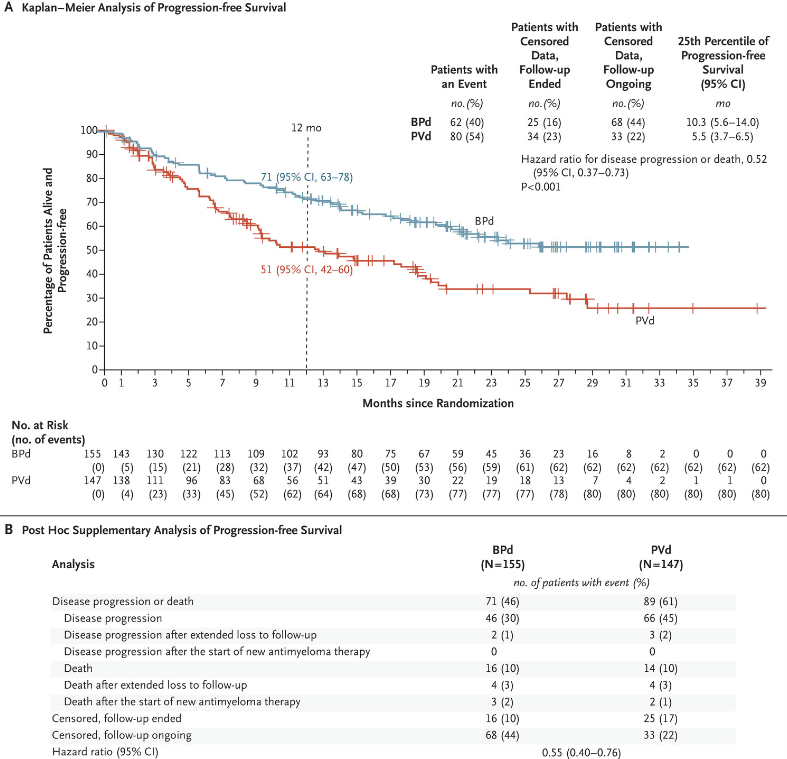
PFS — Primary analysis: median not reached vs 12.7 mo, HR 0.52 (p<0.001); updated 32.6 vs 12.5 mo, HR 0.49; 12-mo PFS 71% vs 51%. (NEJM 2024 / EHA 2025 update)
OS — Positive OS trend, not statistically significant at interim (HR ~0.77); follow-up ongoing. (page data / EHA 2025)
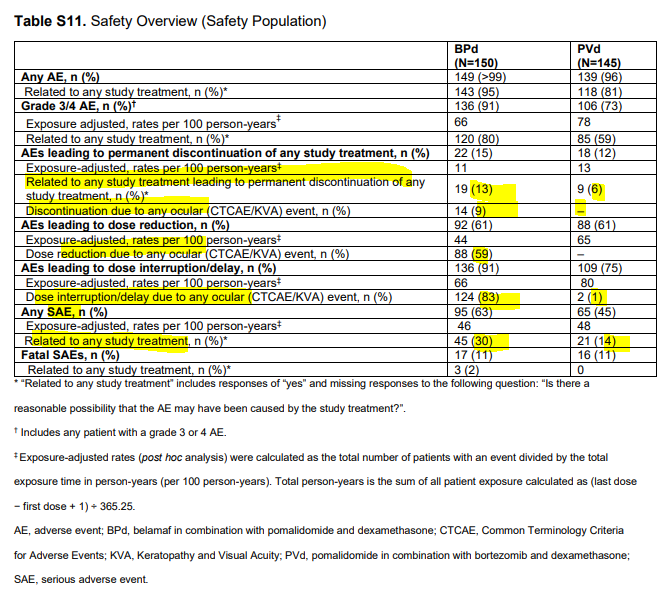
Safety — Grade 3/4 ocular AEs in 43% of BPd vs 2% PVd; ocular toxicity the principal safety concern across DREAMM trials. (page data)
Regulatory — US: NOT FDA approved — ODAC 7-1 against (Jul 17, 2025); FDA declined BPd. Approved in UK/EU/Japan/Switzerland/Canada/Brazil. Only DREAMM-7 BVd is US-approved. (FDA/ODAC; GSK)
Sponsor / Drug — GSK; belantamab mafodotin (Blenrep), a BCMA-directed antibody-drug conjugate (BPd regimen). (GSK)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 20, 2026.
















Top 10 by impressions - click to view on X
The 4 big myeloma randomized trials to watch out for @ASCO #ASCO24 1. Isa-VRd vs Isa-Rd newly diagnosed 2.Isa-VRd vs VRd (IMROZ) 3.DREAMM8 Bela-Pd vs Pd 4.Ven Dex vs Pom...
The comparison of two manuscripts @NEJM showcasing Belantamab's superiority over other anti-myeloma treatments in a head-to-head comparison is widely considered the...
2) Belantamab will make a comeback. Corneal toxicity is low with reduced frequency dosing. The drug works very well. And in many patients with refractory myeloma belantamab may be safer and easier...
Looking forward to the #ASCO24! Here are the lists for five #mmsm abstracts for @OncoAlert: 1- DREAMM-8 belantamab plus pomalidomide/dex (BPd) vs PVd in...
2 NEJM papers for $GSK belamaf @ #ASCO24, respect I bashed that drug a lot (still think its utility gonna be nullified by bispecs) but for now, I just have to shut my...
This is the trial they should have done originally for the initial phase III confirmatory study in relapsed/refractory #myeloma as opposed to the nightmarish DREAMM-3.
Myeloma is full of surprises: EXHIBIT A: Canova EXHIBIT B: DreaMM studies #EHA24RF #mmsm
Now out Belantamab/Pd vs PVd DREAMM-8 trial @NEJM in RRMM: N= 302 patients (155/BPd, and 147/PVd) 12-month PFS BPd was 71% Vs 51% with PVd. ORR: BPd 77% vs PVd 72% CR: BPd 40% vs PVd 16%...
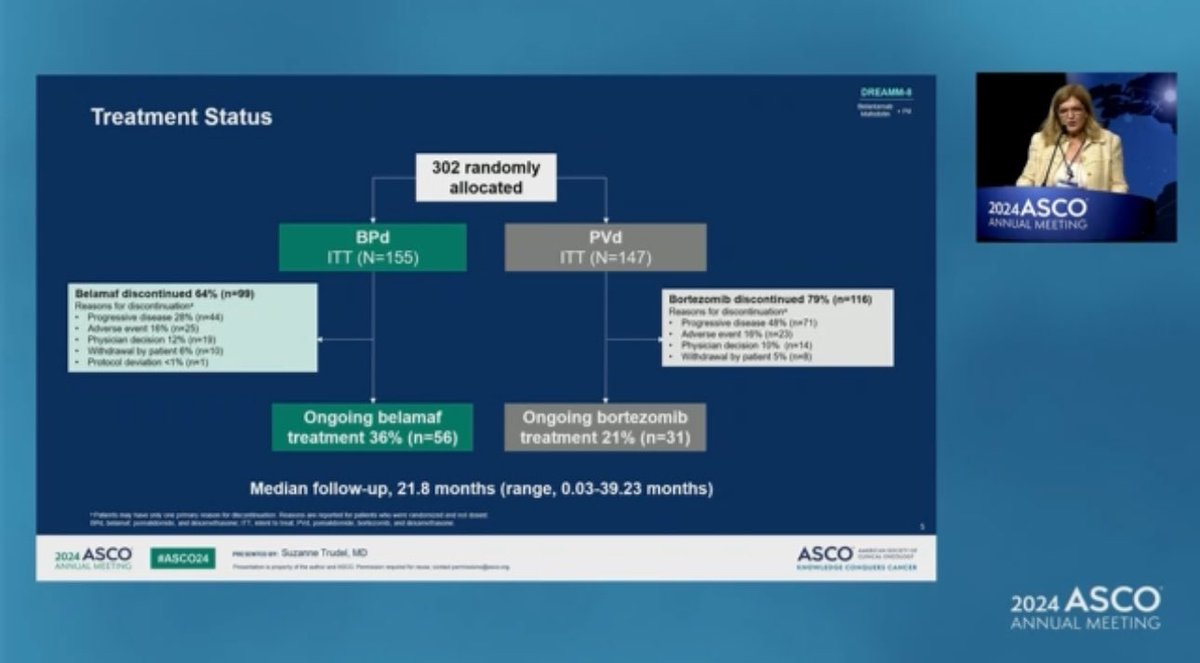
#mmsm #ASCO24 DREAMM-8 Study design 👇 Notice the dose of blenrep was lower than the older dosing with lower dose at second dose Consort diagram and reasons for...
This study also shows a belantamab based triplet providing better PFS rate than another triplet. DREAMM-7 & DREAMM-8 establish the efficacy of belantamab— will likely lead to regulatory...
DREAMM-8 is a Phase III, open-label, multicenter, randomized trial evaluating belantamab mafodotin (Blenrep) plus pomalidomide and dexamethasone (BPd) versus pomalidomide plus bortezomib and dexamethasone (PVd) in patients with relapsed/refractory multiple myeloma who have received at least one prior line of therapy including lenalidomide. The trial enrolled 302 patients and demonstrated a significant PFS benefit for BPd, supporting belantamab mafodotin combinations as a new treatment paradigm in RRMM alongside the companion DREAMM-7 trial.
Phase III, open-label, 1:1 randomized, multicenter trial (NCT04484623). BPd arm: belantamab mafodotin 2.5 mg/kg IV cycle 1, then 1.9 mg/kg Q4W from cycle 2; pomalidomide 4 mg PO days 1-21; dexamethasone 40 mg days 1, 8, 15, 22. PVd arm: bortezomib 1.3 mg/m2 SC days 1, 4, 8, 11 (cycles 1-8), then days 1, 8; pomalidomide 4 mg days 1-14; dexamethasone 20 mg on day of/after bortezomib. Stratified by prior lines, prior bortezomib, and prior anti-CD38. Treatment until progression, death, or unacceptable toxicity.
Adults with relapsed/refractory multiple myeloma who received at least 1 prior line including lenalidomide and had documented disease progression during or after most recent therapy. 78% were lenalidomide-refractory. No prior anti-BCMA or pomalidomide exposure. Not refractory or intolerant to bortezomib. 25% had prior daratumumab exposure.
Arm A: Belantamab mafodotin + pomalidomide + dexamethasone (BPd). Arm B: Pomalidomide + bortezomib + dexamethasone (PVd). Treatment continued until progression, death, unacceptable toxicity, withdrawal of consent, or study cessation.
Primary endpoint: PFS by independent review committee per IMWG criteria. Key secondary endpoints: OS, MRD negativity by NGS. Other secondary: ORR, DOR, CR rate, VGPR or better, time to progression, PFS2, AEs, ocular findings, and patient-reported outcomes.
BPd demonstrated a significant PFS benefit with HR 0.52 (95% CI 0.37-0.73; p<0.001) at primary analysis (median follow-up 21.8 months). Median PFS was not reached (95% CI 20.6-NR) for BPd vs 12.7 months (95% CI 9.1-18.5) for PVd. 12-month PFS rate: 71% vs 51%. Updated analysis at 28 months showed median PFS of 32.6 months vs 12.5 months (HR 0.49). ORR: 77% vs 72%, with CR or better of 40% vs 16%. Median duration of response: not reached vs 17.5 months.
At the interim analysis, a positive trend in OS was observed favoring BPd but was not yet statistically significant. Follow-up for OS continues. The companion DREAMM-7 trial demonstrated a significant OS benefit (HR 0.58) for belantamab mafodotin + BorDex vs daratumumab + BorDex, providing supportive evidence for the class.
AEs occurred in >99% of BPd vs 96% of PVd patients. Ocular toxicity was the primary safety concern: grade 3/4 ocular AEs in 43% of BPd vs 2% of PVd. Over 90% of patients experienced keratopathy/visual acuity events across DREAMM trials, with 77-78% high-grade. Worsening vision-related function (OSDI) in 73% BPd vs 51% PVd, though 92% improved after median 57 days. Over 75% required dose modifications due to KVA events. Fewer than 50% received full intended dose by cycle 3. Despite this, treatment discontinuation due to ocular toxicity was low, and QOL was maintained per EORTC QLQ-C30.
DREAMM-8 positions BPd as a potential new option for RRMM at first relapse, particularly for lenalidomide-refractory patients. At the July 17, 2025 ODAC meeting the committee voted 7-1 against BPd, citing ocular toxicity and dosing-optimization concerns; the FDA subsequently declined BPd in the US and approved only the DREAMM-7 BVd regimen (October 23, 2025, with a REMS program for ocular toxicity). BPd is approved outside the US (UK, Japan, Switzerland, the EU, Canada and Brazil) for RRMM after at least one prior line. Key debates include optimal dose-finding (DREAMM-14 exploring lower doses), real-world management of keratopathy without the strict protocol-driven monitoring used in trials, sequencing with bispecifics and CAR-T, and whether the ODAC dissent and US decision will shape ex-US adoption and the path back to US approval.
DREAMM-8 is a Phase 3 trial of belantamab mafodotin (Blenrep) + pomalidomide + dexamethasone (BPd) versus bortezomib + pomalidomide + dexamethasone (PVd) in adults with relapsed/refractory multiple myeloma who had received at least one prior line including lenalidomide (NCT04484623).
No. The US FDA did not approve the BPd regimen (belantamab mafodotin + pomalidomide + dexamethasone). At the July 17, 2025 ODAC meeting the committee voted 7-1 against BPd, citing ocular toxicity, dosing uncertainty, and limited US trial enrollment. Only the separate DREAMM-7 BVd regimen was FDA approved (October 23, 2025).
Yes. Outside the US, BPd is approved for relapsed/refractory multiple myeloma after at least one prior line including lenalidomide in markets such as the UK, European Union, Japan, Switzerland, Canada, and Brazil.
BPd showed a significant progression-free survival benefit versus PVd: at primary analysis median PFS was not reached versus 12.7 months (HR 0.52, p<0.001), and with longer follow-up 32.6 versus 12.5 months (HR 0.49). The 12-month PFS rate was 71% versus 51%. Overall survival showed a positive but not yet statistically significant trend.
DREAMM-8 tested BPd (belantamab + pomalidomide + dexamethasone); DREAMM-7 tested BVd (belantamab + bortezomib + dexamethasone). The two regimens have different US regulatory status: BVd (DREAMM-7) is FDA approved (Oct 23, 2025), while BPd (DREAMM-8) was not approved in the US.