Phase 3 head-to-head Chinese plenary study at ASCO 2026 (LBA4) — Ivonescimab (PD-1/VEGF bispecific) + platinum chemo vs Tislelizumab (anti-PD-1) + platinum chemo in 1L advanced squamous NSCLC, irrespective of PD-L1. PI Shun Lu (Shanghai Chest). The first IO regimen to beat a PD-1 + chemo control head-to-head on OS.
Slide decks captured live from the ASCO 2026 Plenary (LBA4, presented May 31, 2026 by Prof Shun Lu), newest first, followed by single-slide highlights and discussion captures. Click any image to expand; expand “View OCR Text” to read the slide content.
[Slide 1]
Possibly VEGF-related adverse events
. Possibly YEGP- - NEW - - requestly . the ivonescimab - most of
which - grade N
- -
- -
I I
-
-
- -
-- -
-
.
- I
i
my -
- .
- a
Date 13
2026AS
I
name
MODD
wate
MAR
MISS
---
an
2
ANNUAL MEE
I
---
W/MS
was
104
MORN
MAN
FOR
-
I
-
FOR
was
NONE
can
PAIS
FOR
-
-
-
-
.
and
.
.
.
.
-
-
.
-
.
0.00
.
on
-
I
-
.
-
a
.
.
#
.
I
-
- a -
ASCO
-
-
ASCO -
---
[Slide 2]
Study design
A candiamized, paraliel-controled phase 3 Mudy
- - -
$ 8. $ I
|
I
- -
-
use)
- MKAC
1 I
# a t *
2026
ASC
- - - -
of
ANNUAL MEETIN
I
$ 1 I , .
-
-
-
more - -
I
FOR -
- -
rige ADING -
- expense - by RRC - RECIST RT
POLI - in - is
My security - -
- - . - DOR an TER and -
ASCO
-
-
ASCO -
---
[Slide 3]
Overall survival (interim analysis)
Ivonescimab with chemotherapy significantly improved os
1
Tistelizumeb
1 chemo
chemo
(N-266)
(N-266)
HOS, months
27.89
23.09
100
(94% CI)
(27.89.NE)
(20.11.NE)
90
78.9%
Strattied HR
0.66
so
64.7%
(99% CO
(0.50.0.87)
I I 8
TO
I
0.0017
60
72.2%
8
I 8 - I I I
.
The median 09 - - - PINE -
2
45.0%
have not - - - - - - -
30
20
a
- -
0
- I I
9
,
.
.
a
10
-
21
a
:
00
- -
Months
-
I
-
-
I
-
I
I
I
I
I
and
-
Date - - - 27 -
-
I
I
I
I
-
I
I
I
-
I
-
Median - 21.36 months
- HOL - - - a - - - a unlesse -
3036. ASCO
BASCOUN
- - - -
ASCO -
[Slide 1]
HARMONi-6: Outcomes for Elderly Patients
Ivonescimab-chemo
Tislelizumab-chemo
2026ASCO
Events/Number of
Events/Number of
Hazard ratio
ANNUAL MEETING
Characteristic
Subjects
Subjects
(95% CI)
Favors Ivonescimab+chemo Favors Tislelizumab-chemo
Overall
84/266
120/266
0.66 (0.50,0.87)
Age, years
<65
31/135
63/139
0.43 (0.28.0.67)
265
53/131
57/127
0.93 (0.64, 1.36)
0.125
0.25
0.5
1
2
4
Hazard ratio (95% CI)
The study excluded patients with age > 75 years
Median Age - 64
Median age for lung cancer patients in the US is ~ 70 years
Elderly patients (>70) in E4599 experienced more toxicity without a
survival advantage with the addition of bevacizumab.
Lu S et al ASCO 2026,
2026 ASCO
#ASCO26
PRESENTED BY: Julie R Brahmer, MD, MSc, FASCO, FAIO
Ramalingham S et al JCO 2008; 26:60-65
ASCO
ANNUAL MEETING
Presentation property of the author and A500 Permission required to - contact
KNOWLEDGE CONQUERS CANCER
2026
ASCO
ANNUAL MEETING
---
[Slide 2]
HARMONi-6 Patient Selection
Baseline
Ivonescimab
Tislelizumab
Protocol-specified exclusion
Characteristics
+ chemo
+chemo
2026ASCO
criteria:
ANNUAL MEETING
Major blood
18%
17%
Major blood vessel invasion
vessel
Significant tumor
encasement
cavitation/necrosis
With cavity
9%
9%
Significant hemoptysis
With
32%
30%
hemoptysis
history
These criteria limit Ivonescimab's use in patients with squamous cell carcinoma.
Lu S et al ASCO 2026
2026 ASCO
#ASCO26
PRESENTED BY Julie R Brahmer, MD. MSc. FASCO, FAIO
ASCO
ANNUAL MEETING
Presentation property of - - and ASCO Permission required for - -
KNOWLEDGE CONQUERS CANCER
2026 ASCO
ANNUAL MEETING
---
[Slide 3]
Salient Adverse Events Related to Ivonescimab
2026ASCO
Ivonescimab + chemo
ANNUAL MEETING
Possibly VEGF-
(N=266)
Related AEs"
Any Grade
Grade 1
Grade 2
Grade ≥3
Grade ≥ 3 and serious TRAEs were more
Proteinuria
113 (42.5)
35 (13.2)
60 (22.6)
18 (6.8)
common with Ivonescimab
Haemorrhage
66 (24.8)
39 (14.7)
20 (7.5)
7 (2.6)
No difference in treatment related deaths
Hypertension
39 (14.7)
7 (2.6)
22 (8.3)
10 (3.8)
or hematologic toxicities between arms
Arterial
thromboembolism
4 (1.5)
1 (0.4)
0
3 (1.1)
Grade 3 and higher VEGF-related AEs
Venous
were relatively uncommon.
2 (0.8)
0
thromboembolism
2 (0.8)
0
Fistula
1 (0.4)
0
1 (0.4)
0
Lu S et al ASCO 2026
2026 ASCO
PRESENTED BY: Julie R Brahmer, MD. MSc, FASCO, FAIO
#ASCO26
ASCO
ONCOLOGY
ANNUAL MEETING
Presentation property of the author and ASCO Permission required for - contact permissione@waco.org
KNOWLEDGE CONQUERS CANCER
2026 ASCO
ANNUAL MEETING
---
[Slide 4]
Key Takeaway Points
Ivonescimab plus taxane/carboplatin chemotherapy is
effective for Chinese patients with advanced squamous
2026ASCO
ANNUAL MEETING
NSCLC based on the interim overall survival advantage.
Ivonescimab results in VEGF-related AEs, and there is some
uncertainty regarding patient selection.
Applicability to the global, generally older, squamous lung
cancer population is unclear.
2026 ASCO
PRESENTED BY: Julie R Brahmer, MD, MSc, FASCO, FAIO
ASCO
ANDICAN 10CETY OF
#ASCO26
CLINICAL
ANNUAL MEETING
Presentation property of the who and ASCO Permission required or rease, contact
KNOWLEDGE CONQUERS CANCER
2026
ASCO
ANNUAL MEETING
[Slide 1]
hat's Old is New Again -
years Later VEGF Blockade is Back in Fashion
DEVIL
DEVIL
PRACE
PRADA
2026ASCO
ANNUAL MEETING
ASCO ====
....
---
[Slide 2]
VEFG's Role in Squamous NSCLC
Squamous NSCLC
In 2006,
Ramucirumab was
was excluded from
bevacizumab was
the first and only
bevacizumab trials
approved for use in
VEGF inhibitor found
due to bleeding risks
non-squamous
safe and effective
including life-
NSCLC in
with docetaxel for 2nd
threatening pulmonary
combination with
line treatment of sq
hemorrhage
paclitaxel/carbo
NSCLC in 2014
The NEW EXCLAIN d MEDICINI
Randomized Phase II Trial Comparing
Ramucirumab plus docetaxel versus placebo plus docetaxel for
Bevacizumab Plus Carboplatin and Paclitaxel
second-line treatment of stage IV non-small-cell lung cancer
CHAMPION AETICLE
after disease progression on platinum-based therapy (REVEL):
With Carboplatin and Paclitaxel Alone in
a multicentre, double-blind, randomised phase 3 trial
Previously Untreated Locally Advanced or
Paclitaxel-Carboplatin Alone or with
- - - - - - - I -
- Itemil
Metastatic Non-Small-Cell Lung Cancer
Bevacizumab for Non-Small-Cell Lung Cancer
- - institute - - - - Salage
legs -
Lamont 2014, 34 665-73
Authort - LAST - the - BY -
Alan Sandler, M.D. Robert Con, FRIE - Pm. M.D., Jule Brahmer, M.D.
Cam. LATTER - a - is - and -
joan H. Schiller, M.D. Aftime Cressist M.D. Rogero Lilenbaum, M.D.
—
- - M.D.
(3) - 22 -
- Number
.
2026 ASCO
PRESENTED ST: Julie R Brahmer, MD. MSc. FASCO, FAID
ASCO
AMERICAN SOCIETY or
#ASCO26
CLINICAL CHICOLOGY
ANNUAL MEETING
- a property of the ato and ASCO Perman I to - - 1
KNOWLEDGE CONQUERS CANCER
---
[Slide 3]
HARMONi-6 Interim OS Results
Ivonescimab
Tislelizumab
100
+ chemo
+ chemo
90
(N=266)
(N=266)
78.9%
mOS, months
27.89*
23.69
80
(95% CI)
(27.89, NE)
(20.11, NE)
64.7%
Stratified HR
0.66
70
(95% CI)
(0.50, 0.87)
60
72.2%
p-value
0.0017
Os (%)
I
50
48.6%
40
I
30
I
I
20
Median Follow-up only ~21 mos
10
Requires Longer Follow-up
0
0
6
12
11
It
30
Time (Manths)
Number at risk
166
238
202
119
.
0
160
238
186
III
.
0
Lu S et al ASCO 2026
2026 ASCO
#ASCO26
PRESENTED ET. Julie R Brahmer, MD, MSc. FASCO, FAID
ASCO
MERICAN SOCIETY or
ANNUAL MEETING
CONICAL OWCOLOGY
1 a many of to author and ASCO - - " - - 1
KNOWLEDGE CONQUERS CANCER
[Slide 1]
2026ASCO
ANNUAL MEETING
---
[Slide 2]
survival (interim analysis)
Ivonescimab with chemotherapy significantly improved OS
100
vonescimab
Tislelizumab
78.9%
+ chemo
+ chemo
90
(N=266)
(N=266)
80
mOS, months
27.89
23.69
Overall Survival (%)
64.7%
(95% CI)
70
(27.89, NE)
(20.11, NE)
60
Stratified HR
72.2%
0.66
(95% CI)
50
(0.50,0.87)
40
p-value
0.0017
43.6%
30
OS significance boundary: 0.0049
20
10
Ivonescimab+chemo
The median OS in the ivonescimab group
would have not been reached without the
0
Tislelizumab+chemo
last single event
0
3
6
9
12
15
18
21
24
27
30
No. at risk (censored)
Months
vonescimab
266(0)
252(0)
238(0)
224(0)
202(8)
152(46)
119(73)
85(108)
49(135)
15(168)
0(182)
Chemo
Tislelizumab
266(0)
257(0)
238(0)
211(0)
186(6)
142(36)
113(55)
80(77)
43(107)
12(136)
0(146)
Data cutoff date: Feb 27. 2026
Median Follow-up: 21.36 months
+ Chemo
Abbreviation: mOS, median overall survival; NE, not estimable; HR, hazard ratio; CI, confidence interval
ASCO
PRE SENTED BY:
Shun
LII,
MD.PhD
15.
CHOWLEDGE
consults
2026 ASCO
#ASCO26
author
ASCO
ANNUAL MEETING
2026ASCO ANNUAL MEETING
ASCC
ASCO
ASCO
ASCO
ASCO
ASCO
SCO
ASC
---
[Slide 3]
Conclusions
first-line Ivonescimab with chemotherapy significantly improved OS in advanced squmous NSCLC as
treatment compared with tislelizumab plus chemotherapy
mos: 27.89 vs. 23.69, HR=0.66 (95%Cl: 0.50, 0.87), p=0.0017
chemotherapy vonescimab with chemotherapy showed comparable safety profile to tislelizumab plus
≥ G3 TRAE: 69.2% VS. 58.9%
Similar rates of AEs leading to discontinuation or death between the two arms
HARMONi-6 supports adoption of ivonescimab with chemotherapy as a new standard
for patients with advanced squamous NSCLC in first-line treatment in China
A global phase 3 study (HARMONi-3, NCT05899608) is underway
2026 ASCO
PRESENTED
BY:
Shun Lu, MD, PhD
ASCO
UNCA -
#ASCO26
ENOWLEDGE CONQUERS CANCEL
ANNUAL MEETING
Presentation property the ather and ASCO Permission required for - and 1
[Slide 1]
2026
ASCO
ANNUAL MEETING
Ivonescimab plus chemotherapy versus tislelizumab
plus chemotherapy in previously untreated advanced
squamous non-small cell lung cancer: Overall surviva
results of the Phase 3 HARMONi-6
Presented by: Shun Lu, MD, PhD
Chen Zhiwei¹, Fang Yang², Yongzhong Luo3, Longhua Sun⁴, Lin Wu3, Zhengelang Han5, Yun Fan6, Yanqiu Zhao', XingYa Li8, Haipeng Xu9, Xiangjiao Meng
Ying Liu", Zhiye Zhang12, Hui Luo13, Qin Shi14, Xuelei Ma15, Xuezhen Ma Zhomgmin Zhang17, Michelle Y. Xia18, Shun Lu1
Shanghai Chest Hospital, Shanghai, Jiao Tong University, School of Medicine, Shanghai Chink Harbin Wedical University Cancer Hospital, Harbin, China; Hunan Cancer Hospital, Changsha, China; The
Affiliated Hospital of Nanchang University, Nanchang, China; The Affiialed Hospital of Xuzhou Medical University Kuzhou, China; "Zhejiang Cancer Hospital, Hangzhou, China; Henan Cancer Hospital,
Zhengzhou, China, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China; Fujan Provincial Tumor Hospital, Fuzhou, China; Shandong Cancer Hospital and Institute, Jinan, China; Jili
Cancer Hospital, Changchun, China The First Affiliated Hospital of Henan University of Science and Testerology, Lucyang, China; Jiangxi Cancer Hospital, Nanchang, China; Fuzhou pulmonary hospit
Agian, China Fuzhou, China; West China Hospital of Sichuan University, Chengdu, China; "Qingdad Central Hospital, Dingdao, China; "Linyi People's Hospital, Linyi, China; "Akeso Biopharma, Inc., Zhongsha
2026 ASCO
#ASCO26
PRESENTED in Shun Lu, MD, PhD
ANNUAL MEETING
ASC
Insertation property to are and AS02 Permission - a -
KNOWLEDGE
---
[Slide 2]
Study design
A multicenter, randomized, double-blind, parallel-controlled phase 3 study
Ivonescimab (20 mg/kg, Q3W)
Ivonescimab
Key Eligibility Criteria
+
Carboplatin (AUC 5, Q3W)
(20 mg/kg, Q3W)
Pathologically confirmed
+
Pacilitaxel (175 mg/m², Q3W)
up to 24 months
squamous NSCLC
up to 4 cycles
Stage IIIB-IV
R
No prior systemic therapy
1:1
Tislelizumab (200 mg, Q3W)
Tislelizumab
No EGFR mutations or ALK
N=532
+ Carboplatin (AUC 5, Q3W)
rearrangements
(200 mg, Q3W)
+
Pacilitaxel (175 mg/m2, Q3W)
up to 24 months
ECOG PS 0 or 1
up to 4 cycles
Stratification Factors:
Endpoints:
Stage: IIIB/IIIC vs. IV
Primary endpoint: PFS by IRRC per RECIST v1.1
PD-L1 TPS: ≥1% vs. <1%
Key secondary endpoint: os
Secondary endpoints: PFS by INV, ORR, DCR, DoR, TTR and safety
Abbreviation: score; PD-1, programmed NSCLC, non-small death-1; cell TPS, lung tumor cancer, EGFR, epidermal growth factor receptor, ALLIK, anaplastic lymphoma kinase; ECOG PS, Eastern Cooperative performance
rate; DoR duration of response: TTR, time to response. 1.1; PFS, progression-free sumrual; OS, overall survival; INV, investigator; ORR, overall response radiology rate; DCR, committee; disease control
RECIST v1.1, response evaluation criteria in solid proportion tumors version score; R, randomization; AUC, area under the curve; Q3W, every three weeks; IRRC, independent Oncology review Group
2026 ASCO
#ASCO26
PRE SENTED BT: Shun Lu, MD, PhD
ANNUAL MEETING
Presentation property of the author and ASCO Permission required for rese contact
ASCO
AMERICAN SOCIETY or
CLINICAL ONCOLOGY
KNOWLEDGE CONQUERS CANCER
---
[Slide 3]
Overall survival (interim analysis)
Ivonescimab with chemotherapy significantly improved OS
Ivonescimab
Tislelizumab
+
chemo
+ chemo
(N=266)
(N=266)
100
78.9%
mOS, months
27.89
23.69
90
(95% CI)
(27.89, NE)
(20.11, NE)
80
64.7%
Stratified HR
0.66
Overall Survival (%)
70
60
72.2%
(95% CI)
(0.50, 0.87)
50
p-value
0.0017
40
48.6%
30
OS significance boundary: 0.0049
20
10
Ivonescimab+chemo
The median OS in the ivonescimab group
would have not been reached without the
0
Tislelizumab+chemo
last single event
0
3
6
9
12
15
18
21
24
27
30
No. at risk (censored)
Months
Ivonescimab
+Chemo
266(0)
252(0)
238(0)
224(0)
202(8)
152(46)
119(73)
85(100)
49(135)
15(168)
0(182)
Tislelizumab
255(0)
257(0)
238(0)
211(0)
186(6)
142(36)
113(55)
+Chemo
43(107)
12(136)
0(146)
Data cutoff date: Feb 27, 2026
Abbreviation: mOS, median overall survival; NE, not estimable; HR, hazard ratio; CI, confidence interval
Median Follow-up: 21.36 months
2026 ASCO
#ASCO26
PRE SENTED BY: Shup Lee, MD PhD
ANNUAL MEETING
ASCO
AMERICAN SOCITY or
Presentation a property of the who and ASCO Permission required or rive contact a
CUNICAL ONCOLOGY
KNOWLEDGE CONQUERS CANCER
---
[Slide 4]
Key takeaway points
VEGF
Ivonescimab
HARMONi-6
PD-1
I
Ivonescimab is the worldwide first PD-1/VEGF dual-target bispecific antibody
and has been approved in China in two lung indications since 2024
Ivonescimab plus chemotherapy significantly improved overall survival
(OS) in previously untreated advanced squamous NSCLC compared with
tislelizumab plus chemotherapy
I
HARMONi-6 met its primary endpoint, all key secondary and secondary
endpoints, and had a manageable safety profile consistent with prior studies
2026 ASCO
PRESENTED If Shun Lu, MD, PhD
ASCO
AMERICAN SOCIETY OF
CLINICAL
#ASCO26
ONCOLOGY
ANNUAL MEETING
- your who and 400 Penicion - - and
CHOWLEDGE CONQUERS CANCER
[Slide 1]
Refresh from ESMO 2025 Presentation:
HARMONI
Subgroup Analysis of PFS by IRRC (Oct 2025 Presentation)
PFS benefit favored ivonescimab across all key subgroups.
Observed important baseline imbalances in the older patient subgroup (Age ≥65), such as target lesion size,
brain metastases. After adjusting for these covariates, the adjusted HR for Age ≥65 was 0.69.
Ivonescimab+chemo
Tislelizumab+chemo
Events/Number of
Events/Number of
Hazard ratio
Favors Ivonescimab+chemo
Favors Tislelizumab+chemo
Characteristic
Subjects
Subjects
(95% CI)
Overall
94/266
127/266
0.60 (0.46. 0.78)
Age, years
<65
37/135
69/139
0.40 26, 0.59)
>65
57/131
58/127
0.88 (0.61. 1.27)
Sex
Male
90/256
118/238
0.59 (0.45. 0.78)
Female
4/10
9/28
Previously
ECOG PS
0
16/42
21/42
0.61 32. 1.17)
1
78/224
106/222
0.61 (0.45, 0.82)
Presented PFS
Disease Stage
IIIB/IIIC
12/21
8/20
IV
82/245
119/246
0.55 (0.41. 0.73)
Data -
PD-L1 TPS
<1%
42/105
58/105
0.55 (0.37, 0.82)
>1%
52/161
69/161
0.66 (0.46, 0.95)
Oct 2025
1-49%
35/112
47/99
0.63 41. 0.98)
>50%
17/49
22/62
0.71 (0.37, 1.33)
23 metastases sites
(ESMO 2025 and Chen,
Yes
17/42
26/39
0.46 (0. 25. 0.85)
No
77/224
101/227
0.64 (0.48, 0.87)
et. al., The Lancet)
Liver metastases
Yes
11/28
24/45
0.53 26. 1.08)
No
83/238
103/221
0.64 (0.48, 0.85)
Brain metastases
Yes
2/9
11/17
No
92/257
116/249
0.64 (0.49. 0.85)
0.125
0.25
0.5
1
2
4
Shun Lu
Hazard ratio (95% CI)
If the number of events at a level of a subgroup is less than 10. the median PFS and hazard ratio will not be provided
ESMO 2025 Presidential Symposium
Ivonescimab is an investigational therapy not presently approved by any regulatory authority other than China's National Medical Products Administration (NMPA).
⚠️ Investigational Ivonescimab is not approved by FDA or EMA
Ivonescimab (AK112) is the first-in-class PD-1/VEGF bispecific antibody developed by Akeso and licensed by Summit Therapeutics for the US, Canada, Europe, Japan, and other regions. It was first approved in China (May 2024) for EGFR-mutant NSCLC and (April 2025) for 1L PD-L1+ NSCLC monotherapy. The HARMONi-6 OS data, presented at ASCO 2026 Plenary, support a planned Akeso China sBLA filing for 1L squamous NSCLC. Summit's global confirmatory program (HARMONi-3) is ongoing — the squamous cohort missed its interim PFS bar in May 2026, with final PFS expected H2 2026.
HARMONi-6 (AK112-306, NCT05840016) is a single-region, multi-center, randomized Phase 3 trial conducted in China and sponsored by Akeso. It enrolled 532 patients with previously untreated, locally advanced or metastatic squamous NSCLC, irrespective of PD-L1 expression, with approximately 63% centrally located tumors and 33.8% with multi-site / liver / brain metastases. The primary endpoint was investigator-assessed PFS (met at interim, HR 0.60); the key secondary endpoint was OS, which crossed the pre-specified efficacy boundary at the planned interim analysis (data cutoff Feb 27, 2026).
Design
Randomized, double-blind, active-controlled Phase 3 (China). 1:1 randomization. Stratified by stage (IIIB/C vs IV) and PD-L1 TPS (<1% vs ≥1%).
Population
n=532. Previously untreated locally advanced or metastatic squamous NSCLC, irrespective of PD-L1. ~63% centrally located tumors; 39% PD-L1 TPS <1%.
Intervention
Ivonescimab 20 mg/kg Q3W + paclitaxel 175 mg/m² + carboplatin AUC5 (q3w ×4) vs Tislelizumab 200 mg + the same chemo backbone, followed by ivonescimab or tislelizumab maintenance up to 24 months.
Endpoints
Primary: PFS (BICR). Key secondary: OS. Other: ORR, DoR, safety, PRO. Independent Data Monitoring Committee assessed pre-specified OS interim.
PI & Site
Prof Shun Lu, MD, PhD — Director, Lung Cancer Center, Shanghai Chest Hospital, Shanghai Jiao Tong University School of Medicine.
Sponsor
Akeso, Inc. (HKEX: 9926.HK) sponsor of record. Summit Therapeutics (NASDAQ: SMMT) holds ex-China rights to ivonescimab.
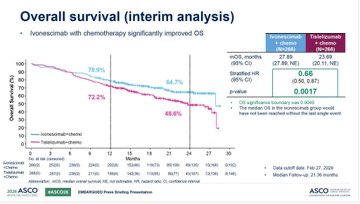
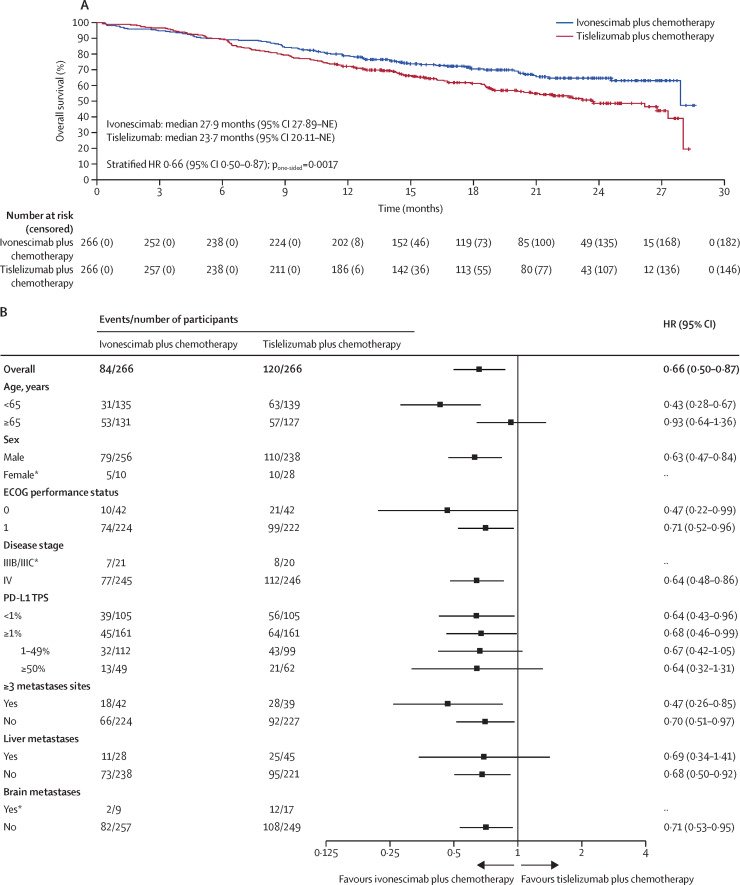
Ivonescimab + chemo demonstrated a statistically significant and clinically meaningful OS benefit vs tislelizumab + chemo at the pre-specified interim. HR 0.66 (95% CI 0.50–0.87; p=0.0017) — a 34% reduction in the risk of death. Median follow-up 21.4 months (data cutoff Feb 27, 2026). Median OS 27.9 months (ivonescimab arm) vs 23.7 months (tislelizumab arm). 24-month OS rates: 64.7% vs 48.6%; 12-month OS 78.9% vs 72.2%. The interim crossed the pre-specified efficacy boundary (p<0.0049). OS benefit was directionally consistent across pre-specified subgroups; subsequent anticancer therapy was comparable between arms.
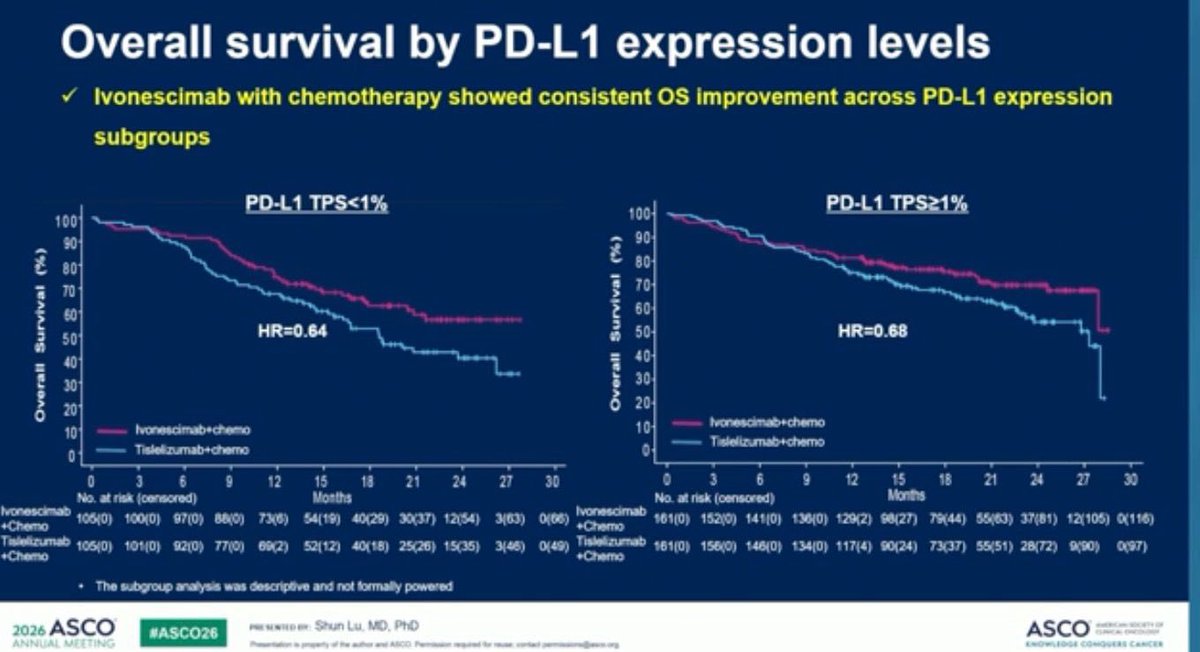
HARMONi-6 met its primary PFS endpoint at the earlier interim analysis. Median PFS 11.1 months vs 6.9 months (HR 0.60; 95% CI 0.46–0.78; p<0.0001) at median follow-up 10.3 months by BICR — a 40% reduction in disease progression or death. By investigator assessment: HR 0.64 (95% CI 0.50–0.84). PFS benefit was consistent across PD-L1 subgroups (TPS <1%: 9.9 vs 5.7 mo, HR 0.55; TPS ≥1%: 12.6 vs 8.6 mo, HR 0.66). Updated PFS at the ASCO data cut was 11.4 vs 6.9 months (HR 0.60).
Objective response rate was 75.9% (ivonescimab) vs 66.5% (tislelizumab), p=0.008. In PD-L1 TPS ≥1%: ORR 80.1% vs 70.2%. Median duration of response was 11.2 months vs 8.4 months (p=0.0219). Responses were both higher and more durable in the ivonescimab arm — consistent with the OS benefit reported at ASCO 2026.
Safety (ASCO 2026 interim cut, data cutoff Feb 27, 2026)
At the ASCO 2026 interim cut, overall safety was manageable and consistent with the established platinum-doublet plus IO profile. Grade ≥3 treatment-related AEs: 69.2% (ivonescimab) vs 58.9% (tislelizumab), driven predominantly by chemotherapy-related myelosuppression (neutropenia, leukopenia, anemia). Serious treatment-related AEs: 41.4% vs 34.3%. Grade ≥3 hemorrhage — a mechanism-of-interest event for anti-VEGF agents in squamous histology — was uncommon but numerically higher in the ivonescimab arm: 2.6% vs 0.8%. Treatment-related discontinuation: 5.3% vs 4.5%. No new safety signals were identified versus the primary PFS analysis (WCLC 2025 / The Lancet).
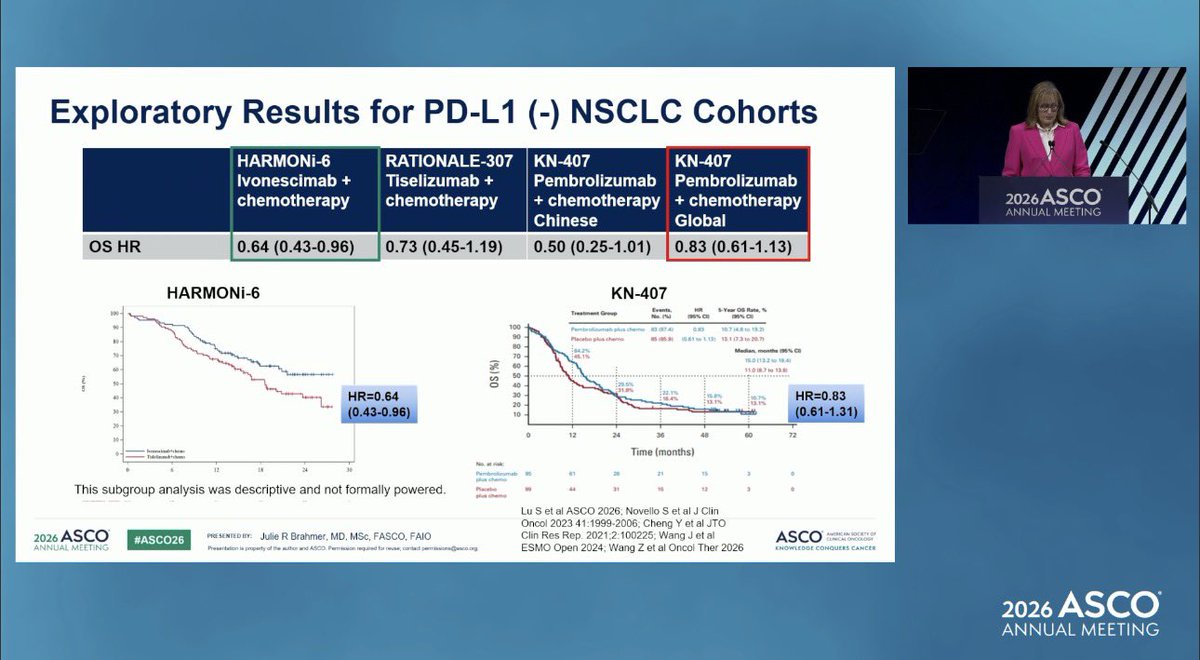
HARMONi-6 is the first Phase 3 trial in which any regimen has beaten a PD-1 + chemo control on OS in 1L NSCLC head-to-head — a benchmark that single-agent ivonescimab failed to clear vs Keytruda in HARMONi-2 (Chinese 1L PD-L1+ NSCLC, 22.3% death-risk reduction, immature). It also re-opens the door to anti-VEGF mechanisms in squamous NSCLC, a population historically excluded from bevacizumab due to bleeding risk. In her invited discussion, Dr Julie Brahmer (Johns Hopkins) called the result provocative but cautioned against immediate ex-China practice change: HARMONi-6 enrolled an exclusively Chinese, almost entirely male population, excluded patients >75, showed attenuated benefit in those >65 (HR near 1.0), and had relatively short follow-up — leaving global applicability and bleeding-risk generalizability open. This was the first single-region Chinese dataset featured at an ASCO Plenary in 61 years. Ex-China translation remains an open question: the global confirmatory HARMONi-3 squamous cohort missed its interim PFS bar on May 1, 2026, and Summit (NASDAQ: SMMT) shares fell ~25% on the news. Final HARMONi-3 PFS is expected H2 2026.
Peer-reviewed publications, sponsor releases, and oncology news on the ASCO 2026 Plenary (LBA4) readout. Sourced and cross-checked against the trial's primary-source notebook; verified links only.