GI Cancer
ARMANI
About the ARMANI Trial
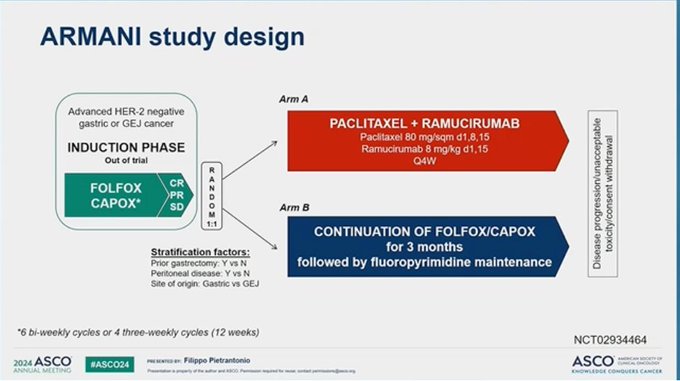
The ARMANI study is a randomized Phase II trial evaluating switch maintenance therapy in patients with advanced HER2-negative gastric or gastroesophageal junction (GEJ) cancer. Following initial induction with FOLFOX or CAPOX chemotherapy, patients were randomized 1:1 to either continue with the induction regimen or switch to maintenance therapy with paclitaxel plus ramucirumab. The primary endpoint was progression-free survival (PFS), with secondary endpoints including overall survival (OS), objective response rate (ORR), and safety.
The study demonstrated a significant benefit for switch maintenance, with improved PFS (6.6 vs. 3.5 months) and OS (12.6 vs. 10.4 months) compared to continued chemotherapy. However, this benefit came with an increased incidence of Grade 3 treatment-related adverse events in the paclitaxel/ramucirumab arm. These findings, presented at the 2024 ASCO Annual Meeting by Dr. Filippo Pietrantonio and discussed by experts including Dr. Sharlene Gill and Dr. Jun Gong, highlight the potential value of treatment sequencing to optimize outcomes in advanced HER2-negative gastric/GEJ cancer.
Table of Contents
Major Presentations and Milestones
ARMANI Trial design, results, and conclusions
ARMANI Sentiments and Criticisms
Professional Resources : Interactive Tweet History, Influence Diagram, Sentiment Table, AI Chatbot
ARMANI Trial: Major Presentations and Milestones
Primary speakers driving the story
Filippo Pietrantonio, MD (Istituto Nazionale dei Tumori, Milan) presented the phase 3 ARMANI trial at ASCO 2024, evaluating switch maintenance with paclitaxel plus ramucirumab versus oxaliplatin-based chemotherapy continuation in advanced HER2‑negative gastric or gastroesophageal junction (GEJ) cancer after 3 months of induction FOLFOX/CAPOX. Discussant Nataliya Uboha, MD, PhD (UW Carbone) contextualized the findings alongside EA2174 and RENAISSANCE, focusing on applicability in today’s biomarker‑driven first‑line landscape. Clinician coverage emphasized significant PFS and OS gains with ARMANI’s strategy, balanced by higher grade ≥3 toxicity.
Ramucirumab + paclitaxel as switch maintenance vs CTxcontinuation in GC & GEJ cancer #ASCO24 🔎ARMANI phase III trial, 197 pts 👉ORR 19 vs 15.7% 👉mPFS 6.6 vs. 3.5 mo 👉mOS 12.6 vs. 10.4 mo 👉AE ≥3 40.4 vs. 20.7% 🧠Switch maintenance after 3 months FOLFOX valid option for… https://t.co/K1H1vOnzFn https://t.co/Fnfwq4kwYO
— Arndt Vogel (@ArndtVogel) June 4, 2024
Arndt Vogel, MD (ASCO24): Key headline efficacy and safety metrics and a pragmatic take that switch maintenance is “a valid option” after induction FOLFOX.
@FilippoPietran4 Ram/paclitaxel as switch maintenance vs. continuation of 1st-line chemo in advanced HER2- cancers: The ARMANI phase III trial of gastric or GE jxn. #asco24 @ASCO - Fulfilled the primary endpoint: PFS = 6.6M vs. 3.5M (HR = 0.64) but noted⬆️ toxicities (40.4 vs.… https://t.co/uapXkwNqRW https://t.co/usB9uexgpH
— Dr. Cathy Eng (@CathyEngMD) June 4, 2024
Cathy Eng, MD (ASCO24): Fulfillment of the PFS primary endpoint with HR 0.64 and explicit toxicity caveat.
#ASCO24 @ASCO #EsophagogastricCA #ARMANI switch "maintenance" after induction FU/ox 📌 N=280, HER2- G/GEJ 📌 74% Gastric, 74% PS0, 50% peritoneal 👉impr PFS (+3.2m, HR0.62), and OS 12.6v10.4m, HR0.75 👉increased toxicity! 🤔Where does this fit with 1L IO and emerging… https://t.co/aF2WSxAmgZ https://t.co/qDCi7XTrxq
— Sharlene Gill, MD, MPH, MBA, FASCO (@GillSharlene) June 4, 2024
Sharlene Gill, MD, MPH, MBA (ASCO24): Baseline context and the key question of positioning vis‑à‑vis first‑line immunotherapy and emerging strategies.
ARMANI Trial Design, Results, and Conclusions
Trial Design:
Phase 3, HER2‑negative advanced gastric/GEJ adenocarcinoma. After 3 months of induction FOLFOX or CAPOX, patients with CR/PR/SD were randomized 1:1 to switch maintenance with paclitaxel plus ramucirumab versus continuation of FOLFOX/CAPOX (followed by fluoropyrimidine maintenance per schema). Reported stratification factors included prior gastrectomy (Y/N), peritoneal disease (Y/N), and primary site (gastric vs GEJ). Randomized population ~280 (Arm A n~144, Arm B n~136 per KM at‑risk tables).
Primary Results:
PFS (primary endpoint) improved with switch maintenance: median 6.6 vs 3.5 months, HR 0.64 (95% CI 0.49–0.81), p<0.001. OS improved: median 12.6 vs 10.4 months, HR 0.75 (95% CI 0.58–0.97), p=0.028. Multiple on‑session summaries also reported ORR 19% vs 15.7% and a 24‑month restricted mean PFS increase of ~2.4 months in the experimental arm.
Dr. Pietrantonio PhIII ARMANI adv HER2- G/GEJ cancer induction FOLFOX/CAPOX X3 mos rand 1:1 switch maint ram/taxol vs oxali-chemo X3 mos ➡️ median PFS 6.6 vs 3.5 mos & OS 12.6 vs 10.4 mos sig diff in favor of switch maint, G3 AEs 40% vs 20%. No #IO included #ASCO24 @OncoAlert https://t.co/3CDjsDpOxz
— Jun Gong (@jgong15) June 4, 2024
Safety:
Grade ≥3 treatment‑related adverse events were higher with paclitaxel+ramucirumab: 40.4% vs 20.7%. Notable events included neutropenia (grade ≥3 ~26% vs ~10%), hypertension (grade ≥3 ~6% vs ~0%), and peripheral neuropathy (any‑grade ~62% vs ~45%), consistent with known taxane/anti‑VEGFR profiles.
#ASCO24 ARMANI Trial: ⏰ Switch maintenance Paclitaxel/ Ramicurimab after induction with 3 months FOLFOX/CAPOX in metastatic HER2 -ve E/GEJ-AC ⏰ switch maintenance significantly improved PFS and OS ⏰ However, this came with increased rate of toxicity with 40.4 % vs 20.7%… https://t.co/7UWr5APpTX https://t.co/qHZEJQlgKh
— Osama Mosalem, MD (@OsamaMosalemMD) June 4, 2024
Key Conclusions:
Switch maintenance with paclitaxel plus ramucirumab after induction FOLFOX/CAPOX significantly prolongs PFS and OS versus continuing oxaliplatin‑based chemotherapy, at the cost of higher grade ≥3 toxicity. Presenters and discussants noted that ARMANI is most relevant for patients not receiving upfront PD‑1–based regimens or those ineligible for immunotherapy; positioning in current biomarker‑driven first‑line pathways remains an area for clinical judgment and further study.
ARMANI Sentiments and Criticisms
Positive Reception:
Massimo Di Maio: "Brilliant presentation of the Italian ARMANI trial by @FilippoPietran4 at #ASCO24. Bravo Filippo, as usual, and bravo to all investigators" https://x.com/MassimoDiMaio75/status/1798014085340270899
Noelle LoConte, MD: "ARMANI study supports chemo switch to pacli/ram after three months of FOLFOX for gastric ca with survival advantage" https://x.com/loconte/status/1798012783415767104
VJ Oncology summarized biomarker niche: "ARMMANI study on HER2-negative gastric/GEJ cancer with low/absent PD-L1. Paclitaxel + ramucirumab improved PFS … and OS …" https://x.com/VJOncology/status/1807051645471097127
Balancing Efficacy and Toxicity; Fit in IO Era:
Sharlene Gill, MD, MPH, MBA: "…impr PFS (+3.2m, HR0.62), and OS 12.6v10.4m, HR0.75 … increased toxicity! 🤔Where does this fit with 1L IO and emerging…" https://x.com/GillSharlene/status/1798018510792052889
Cathy Eng, MD: "Fulfilled the primary endpoint: PFS = 6.6M vs. 3.5M (HR = 0.64) but noted⬆️ toxicities (40.4 vs.…)" https://x.com/CathyEngMD/status/1798015028735447098
Emil Lou, MD, PhD: "ARMANI is an interesting therapeutic strategy … If toxicities can be reduced, it’s an approach to investigate in additional settings." https://x.com/cancerassassin1/status/1798014766495277299
ARMANI Temporal Sentiment Arc
Pre‑ASCO24 (Tease and anticipation)
- https://x.com/marklewismd/status/1783267445798830086
- Tone: Lighthearted anticipation as ARMANI became a talking point ahead of ASCO.
- Shift: Set the stage for first public presentation of mature efficacy data.
ASCO24 (Initial efficacy and safety readout)
Primary/KOL tweets:
Live from #ASCO24 #GE and #HPB Track 🔥🔥 ARMANI Phase III trial by @FilippoPietran4 ✅Ram+Pacli- switch maintenance vs oxaliplatin continuation in HER2- Gastric or GEJ Cancer ✅✅A +ve study➡️Over 3 months PFS gain ✅✅Increased OS ⬆️⬆️ 🧠Less than 60% received any… https://t.co/2ta6nP1M36 https://t.co/KJtEUfKgk0
— Deniz Can Guven (@DenizCanGuven1) June 4, 2024
- https://x.com/jgong15/status/1798013045568069737
- https://x.com/OsamaMosalemMD/status/1798017040910786744
- https://x.com/CathyEngMD/status/1798016450013339818
- Tone: Clear recognition of clinically meaningful PFS/OS gains with switch maintenance; immediate emphasis on toxicity and real‑world positioning relative to IO‑based first‑line therapy.
- Shift: From headline efficacy to operational fit—who benefits most, when to deploy, and toxicity mitigation.
Mid‑2024 (Post‑ASCO reflections and interviews)
Primary/KOL tweets:
🎥@FilippoPietran4 of @IstTumori discusses the ARMANI study on HER2-negative gastric/GEJ cancer with low/absent PD-L1. Paclitaxel + ramucirumab improved PFS (6.6 vs 3.5 months) and OS (12.6 vs 10.4 months):
— VJ Oncology (@VJOncology) June 29, 2024
➡️https://t.co/mhCCoRDVQY⬅️
@ASCO @OncoAlert #ASCO24
- https://x.com/GillSharlene/status/1798018510792052889
- https://x.com/MassimoDiMaio75/status/1798014085340270899
- Tone: Continued positive interpretation of efficacy; growing focus on identifying the right biomarker contexts (e.g., low/absent PD‑L1, no upfront IO) and acknowledging toxicity trade‑offs.
- Shift: From trial results to practice implementation in selected patient subsets not receiving IO in first line.
Overall arc: Enthusiasm for a pragmatic, non‑IO maintenance strategy with OS benefit, tempered by higher toxicity and the need to define optimal use in an IO‑first era. Subsequent discussions stressed patient selection and toxicity management to translate ARMANI into practice.
ARMANI Professional Resources