First-line unresectable hepatocellular carcinoma (HCC) — Bristol Myers Squibb
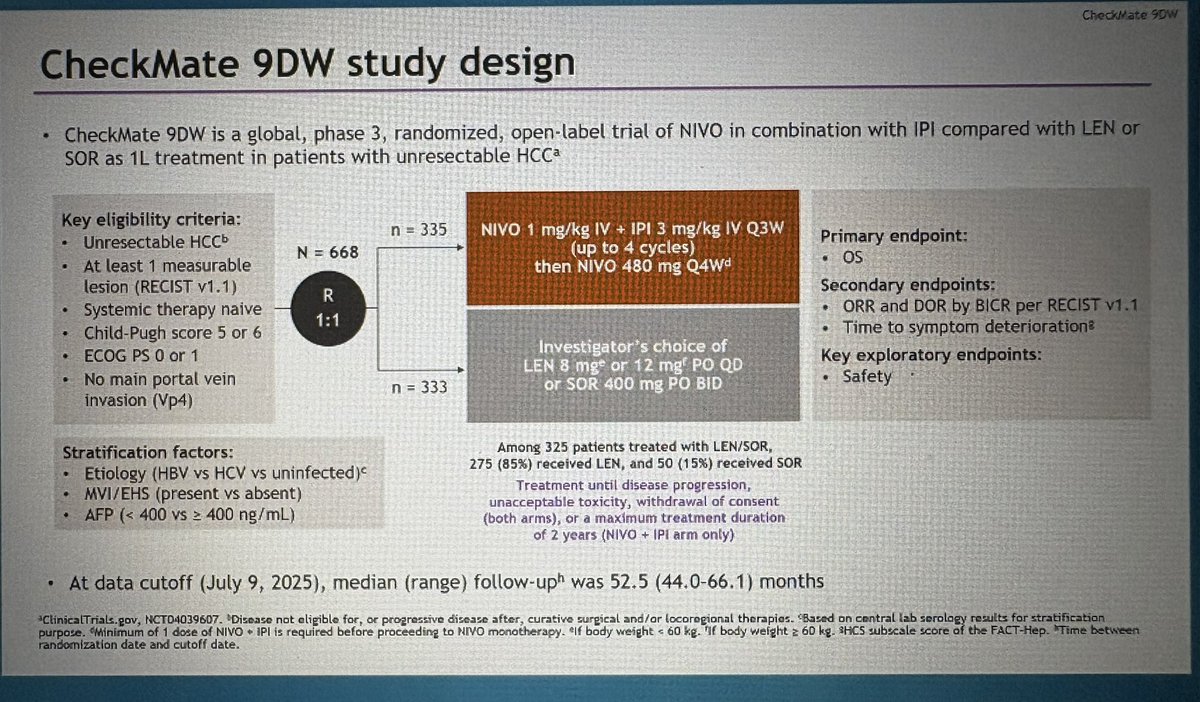
Discover KOL Sentiment on CheckMate-9DW →Design - Phase 3 nivolumab + ipilimumab vs investigator's-choice lenvatinib or sorafenib, 1L unresectable HCC (NCT04039607).
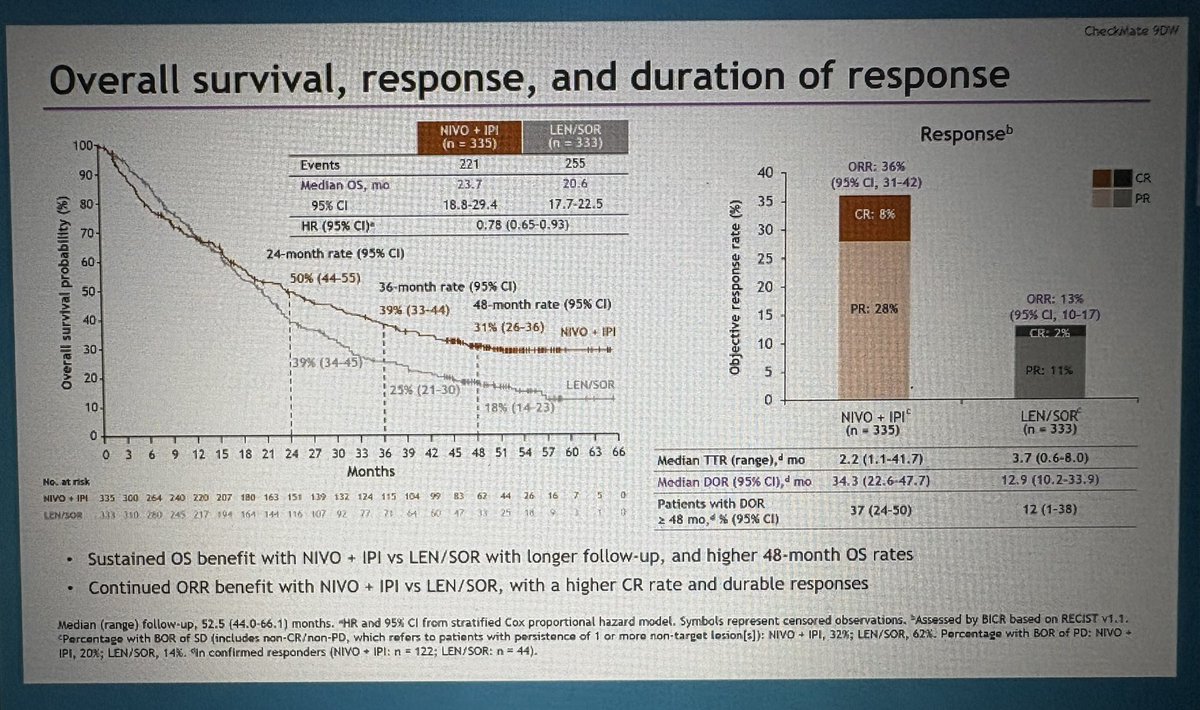
OS (primary) - Median 23.7 vs 20.6 mo, HR 0.79 (95% CI 0.65-0.96), P=0.018.
ORR - 36% vs 13% with the TKI comparator.
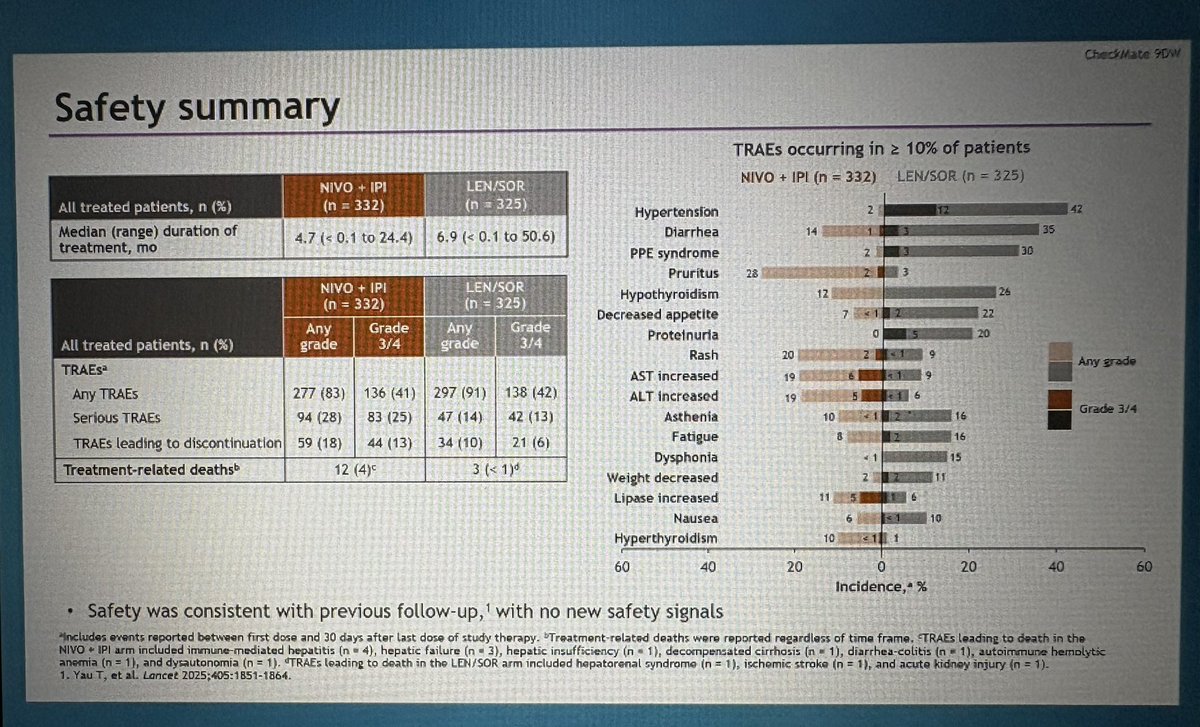
Safety - Grade >=3 treatment-related AEs 41% vs 42%; immune-mediated events (hepatitis, colitis, skin, endocrine); 12 treatment-related deaths in the nivo+ipi arm.
Regulatory - FDA approved April 11, 2025 - converted the CheckMate-040 accelerated approval to regular approval.
Sponsor / drugs - Bristol Myers Squibb; nivolumab (Opdivo) + ipilimumab (Yervoy).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.











Top tweets by impressions — click to view on X
Did you catch our #HCC 📺video update from #ESMO24? Dr Richard Finn reviews the data from HIMALAYA, CheckMate 9DW, LEAP-012 & IMbrave050 & discuss the key takeaways. Watch the short video…
CheckMate9DW expanded analyses
#HCC #GI25
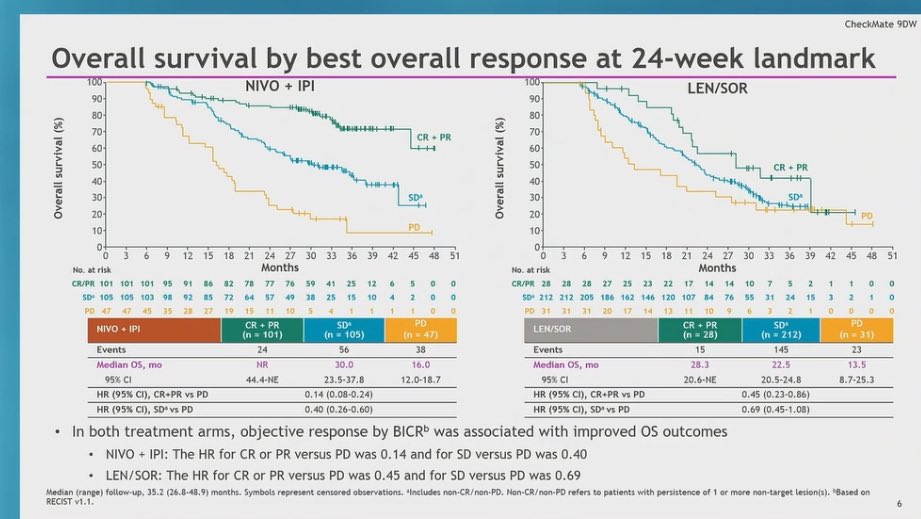
➡️ response in HCC predicts OS
➡️ at 24wks med OS not reached in responders ipi/nivo
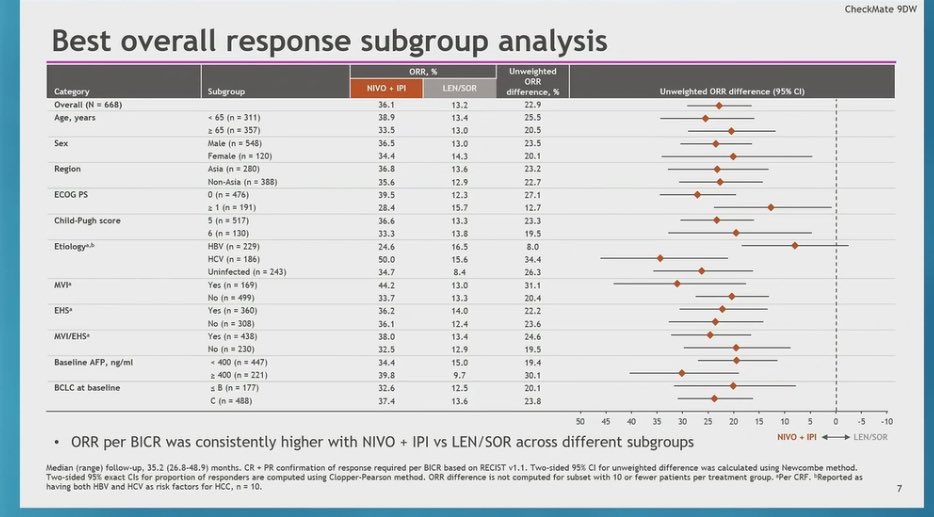
➡️responses consistent across subgroups
➡️still some toxicity…
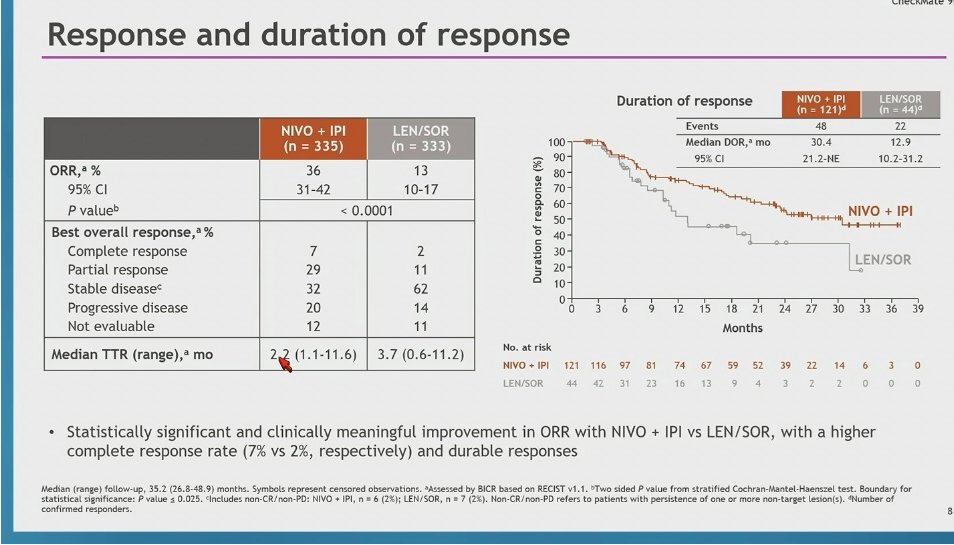
Most impressive data from #CheckMate9DW (frontline nivo/ipi in #HCC) is the median duration of response: 30.4 months❗️Reaffirms something we've seen time and time again⏩Anti-CTLA4 responses are the…
Nivolumab plus ipilimumab vs lenvatinib or sorafenib as first-line treatment for HCC: 4-year follow-up of CheckMate 9DW
#ASCOGI26
👉ORR: 36 vs 13%
👉mOS: 23.7 vs 20.6 mo
🧐 Very valid option in HCC;…
Nivolumab plus ipilimumab vs lenvatinib or sorafenib as first-line treatment for HCC
@TheLancet
https://t.co/QlVvcP1U0l
🔎CheckMate 9DW
👉mOS 23·7 vs 20·6 mo
👉ORR 36 vs 13%
👉Consistent efficacy in…
🙏@drlauragoff @VUMC_Cancer for putting things in perspective to close the @asco #asco24 #GI session 👏👏 re: Checkmate 9DW Nivo/Ipi in #HCC. @bmsnews #cancer #cancerresearch @jordanberlin5 @benhopark…
Overall Health-related quality of life & efficacy assessment in pts who discontinued due to TRAEs
🔎CheckMate 9DW
👉Time to def. deterioration: 22.3 vs 0.5 mo
👉20% stopped due to TRAEs —> OS…
Dr. Galle 4-year follow-up of CM9DW of #1L nivo/ipi vs. len/sorafenib in adv #HCC ➡️ sustained OS benefit median 23.7 vs 20.6 mos, ORR 36% (8% CR) vs 13% (2% CR) in favor of nivo/ipi. 4% G5 AEs with…

5/10 – Checkmate 9DW #HCC
#ASCO @ASCO
phase 3 Nivo1+ipi3 q3w ▶️maint nivo/TKI VS len85%/sor15% in 1L aHCC
📌 n=668, CP-A, PS 0-1
👉ORR 36% (7%CR) vs 13%, durable
👉mOS 23.7m vs 20.6m, HR0.79, p0.018 🌟
-…

Nivolumab plus ipilimumab versus lenvatinib or sorafenib as first-line treatment for unresectable hepatocellular carcinoma (CheckMate 9DW): an open-label, randomised, phase 3 trial @TheLancet…
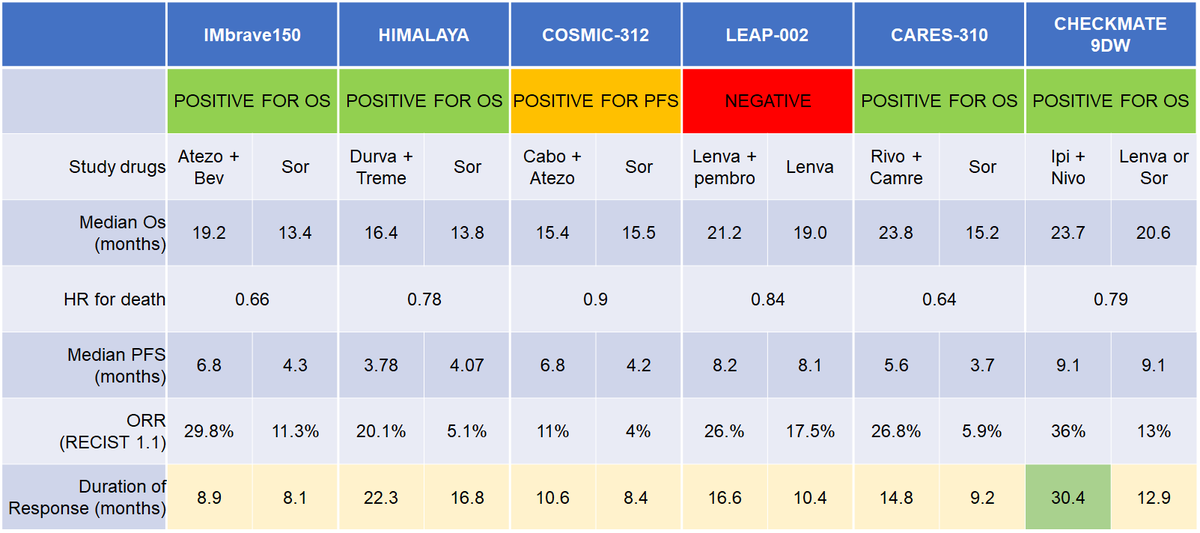
CheckMate-9DW converted the prior CheckMate-040 accelerated approval to regular approval (April 11, 2025) and established nivolumab + ipilimumab as the first immunotherapy regimen to demonstrate OS superiority vs. TKI in 1L unresectable HCC. The 6-month KM crossover (early HR 1.65, then sustained HR 0.61) is a defining nuance — patient selection matters. Competes with IMbrave150 (atezolizumab + bevacizumab), HIMALAYA (STRIDE: tremelimumab + durvalumab), and LEAP-002 (lenvatinib + pembrolizumab, negative).
Median: 23.7 months (nivolumab + ipilimumab) vs. 20.6 months (lenvatinib or sorafenib). HR 0.79 (95% CI 0.65-0.96), P=0.018 Median OS 23.7 months with nivolumab + ipilimumab vs. 20.6 months with investigator's choice lenvatinib or sorafenib; HR 0.79 (95% CI 0.65-0.96, P=0.018). ORR 36.1% vs. 13.2% (P<0.0001). Median PFS 9.1 vs. 9.2 months (not significantly different). Critical nuance: Kaplan-Meier curves crossed at 6 months — early HR 1.65 (early-mortality signal) then HR 0.61 sustained long-term benefit. First immunotherapy combination to demonstrate OS benefit vs. TKI standard in 1L HCC.
Median: 23.7 months (nivolumab + ipilimumab) vs. 20.6 months (lenvatinib or sorafenib). HR 0.79 (95% CI 0.65-0.96), P=0.018 See primary (OS is the primary endpoint).
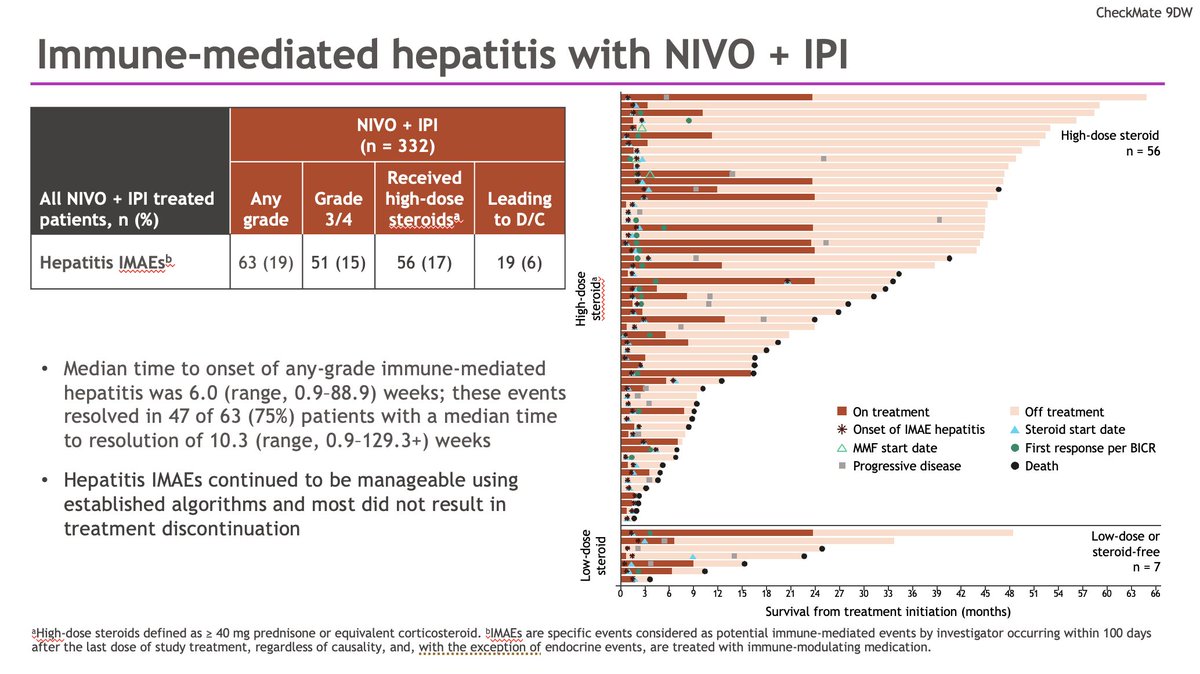
Grade ≥3 adverse events: 41% (nivo_ipi) vs. 42% (lenva_sora). Key AEs: immune-mediated hepatitis, colitis / diarrhea, skin toxicity (rash, pruritus), endocrinopathies (thyroid, adrenal). Grade ≥3 TRAE 41% (nivo+ipi) vs. 42% (TKI). 12 treatment-related deaths in nivo+ipi arm vs. 3 in TKI arm — a notable safety signal driven by early immune-related toxicity. Critical take-home: the 6-month KM crossover (early HR 1.65) reflects early treatment-related mortality; patient selection and early irAE monitoring are paramount.
✅ FDA-approved 1L standard; first IO combo with OS benefit over TKI in HCC. CheckMate-9DW converted the prior CheckMate-040 accelerated approval to regular approval (April 11, 2025) and established nivolumab + ipilimumab as the first immunotherapy regimen to demonstrate OS superiority vs. TKI in 1L unresectable HCC. The 6-month KM crossover (early HR 1.65, then sustained HR 0.61) is a defining nuance — patient selection matters. Competes with IMbrave150 (atezolizumab + bevacizumab), HIMALAYA (STRIDE: tremelimumab + durvalumab), and LEAP-002 (lenvatinib + pembrolizumab, negative).
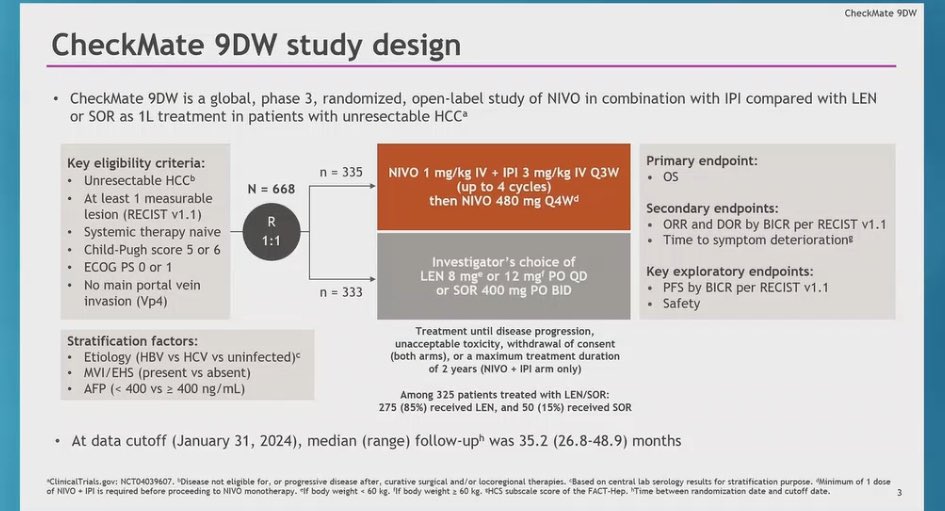
CheckMate-9DW is a Phase 3 randomized trial (NCT04039607) of first-line nivolumab (Opdivo) plus ipilimumab (Yervoy) versus investigator's choice of the tyrosine kinase inhibitors lenvatinib or sorafenib in patients with unresectable hepatocellular carcinoma. Overall survival was the primary endpoint.
Nivolumab plus ipilimumab significantly improved overall survival: median OS was 23.7 versus 20.6 months (HR 0.79; 95% CI 0.65-0.96; P=0.018). The objective response rate was 36% with the immunotherapy combination versus 13% with lenvatinib or sorafenib. It is the first dual-immunotherapy regimen to show an overall survival benefit over TKI therapy in first-line HCC.
Yes. On April 11, 2025 the FDA approved nivolumab (Opdivo) plus ipilimumab (Yervoy) for the first-line treatment of unresectable or metastatic hepatocellular carcinoma, converting the prior CheckMate-040 accelerated approval of this regimen to regular approval based on the CheckMate-9DW survival data.
Grade 3 or higher treatment-related adverse events occurred in about 41% of the nivolumab-plus-ipilimumab arm versus 42% with the TKI comparator, and the profile was dominated by immune-mediated events - hepatitis, colitis or diarrhea, skin toxicity, and endocrinopathies. Twelve treatment-related deaths were reported in the immunotherapy arm, underscoring the need for proactive immune-toxicity monitoring.
CheckMate-9DW gives clinicians a dual-immunotherapy (CTLA-4 plus PD-1) first-line option that improves survival over single-agent TKI therapy, complementing the atezolizumab-plus-bevacizumab and durvalumab-plus-tremelimumab (STRIDE) regimens. Regimen choice is individualized based on bleeding and autoimmune risk, liver function, and the toxicity profile each patient can tolerate.
See the bigger picture: Physician sentiment on OPDIVO (nivolumab) across its trial portfolio →