EMERALD-3 — TL;DR
Design: Phase III, three-arm — STRIDE+lenvatinib+TACE (n=293) vs STRIDE+TACE (n=175) vs TACE alone (n=292); N=760; eeHCC. (ASCO 2026 LBA4000)
PFS (primary, met): 13.0 vs 9.8 mo; HR 0.70 (95% CI 0.57–0.86; P=0.0007) for STRIDE+lenvatinib+TACE. STRIDE+TACE: 12.9 vs 8.1 mo, HR 0.71 (95% CI 0.56–0.91). (RECIST v1.1, DCO1 02-Sep-2025)
ORR: RECIST v1.1 central 36.6% vs 30.0% (DCO1); mRECIST central 67.8% vs 54.8% (DCO1). Updated DCO2 (Feb 2026): 38.9%/40.8% vs 27.0%. (Erinjeri et al., ESMO GI 2026 LBA2)
OS (interim trend): STRIDE+lenvatinib+TACE 39.5 vs 34.7 mo, HR 0.84 (P=0.1814, NS); STRIDE+TACE NR vs 32.9 mo, HR 0.70 (P=0.0233, nominal). (DCO2 23-Feb-2026)
Regulatory: Investigational — no FDA approval for STRIDE ± lenvatinib + TACE in eeHCC as of July 2026.
Sponsor / drugs: AstraZeneca — durvalumab (Imfinzi) + tremelimumab (Imjudo) ± lenvatinib (Lenvima) + TACE.
Track oncology’s top KOLs in your specialty
Create a free account, pick the tumor types you cover, and go beyond the tweet — the intelligence pharma teams use to map influence and prepare for engagement:
- ✓Enhanced KOL profiles
- ✓Pharma influence & potential advisory-board patterns
- ✓2025 Open Payments financial analysis
- ✓Social-media sentiment & trend signals
Physicians Leading the EMERALD-3 Conversation

EMERALD-3 Conference Slides











Top Tweets on EMERALD-3











The EMERALD-3 Debate: Does TACE-Alone Overstate the Benefit?





Trial Overview
EMERALD-3 (NCT05301842)
Unresectable, embolization-eligible hepatocellular carcinoma (eeHCC). 760 patients randomized (STRIDE+lenvatinib+TACE n=293; STRIDE+TACE n=175; TACE alone n=292). Three-arm, randomized, open-label, sponsor-blinded. Sponsor: AstraZeneca. Regimen: STRIDE (durvalumab [Imfinzi] + single-dose tremelimumab [Imjudo]) ± lenvatinib + TACE. In the investigational arms, patients received the STRIDE regimen (Single Tremelimumab, Regular Interval Durvalumab), with or without lenvatinib, prior to TACE and then in combination with TACE thereafter.
Joseph P. Erinjeri, MD, PhD (Memorial Sloan Kettering) presented the ESMO GI 2026 tumor-response analysis (LBA2); ASCO 2026 LBA4000 (Abou-Alfa, Ren, Erinjeri et al.).
Efficacy Results
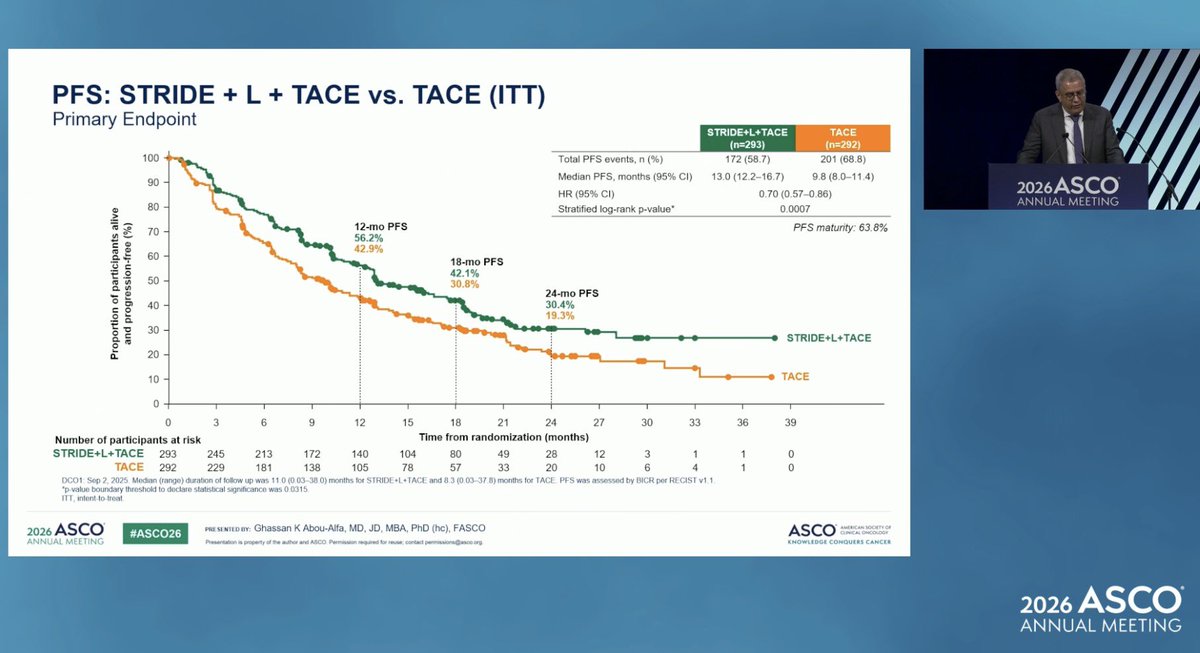
Progression-Free Survival — primary endpoint MET (ASCO 2026 LBA4000, DCO1)
Median PFS 13.0 mo (95% CI 12.2–16.7) with STRIDE + lenvatinib + TACE vs 9.8 mo (95% CI 8.0–11.4) with TACE alone; HR 0.70 (95% CI 0.57–0.86; P=0.0007) — primary endpoint MET (30% reduction in risk of progression or death).
STRIDE + TACE (without lenvatinib): Median PFS 12.9 mo vs 8.1 mo (TACE alone, first 175 randomized); HR 0.71 (95% CI 0.56–0.91) for STRIDE + TACE vs TACE alone.
PFS met: HR 0.70 (30% risk reduction) Source: AstraZeneca / ASCO 2026 LBA4000Objective Response Rate (ESMO GI 2026, DCO1)
ORR by RECIST v1.1 (central review, DCO1 02-Sep-2025): 36.6% (STRIDE+lenvatinib+TACE) vs 30.0% (TACE alone). By mRECIST (central review, DCO1): 67.8% vs 54.8%; by mRECIST (investigator assessment, DCO1): 58.9% vs 42.5%. At the later DCO2 (Feb 2026): ORR 38.9% (STRIDE+lenvatinib+TACE) and 40.8% (STRIDE+TACE) vs 27.0% (TACE alone). (Erinjeri et al., ESMO GI 2026 Abstract LBA2, per OncoDaily congress coverage)
Source: ESMO GI 2026 — Erinjeri (LBA2)Overall Survival — interim trend (STRIDE+lenvatinib+TACE: DCO2 28-Feb-2026; STRIDE+TACE: DCO2 23-Feb-2026)
STRIDE + lenvatinib + TACE: OS trend favored the STRIDE + lenvatinib + TACE arm: median 39.5 mo vs 34.7 mo (TACE); HR 0.84 (95% CI 0.65–1.09; P=0.1814) — interim, NOT statistically significant.
STRIDE + TACE: In the STRIDE + TACE arm, median OS was not reached vs 32.9 mo in the first 175 patients randomized to TACE alone; HR 0.70 (95% CI 0.51–0.95; P=0.0233, nominal / descriptive per pre-specified hierarchy).
Encouraging early OS trend — interim, immature Source: ASCO Daily News — EMERALD-3 OSDuration of Response
Duration of response and DoR were reported as improved with STRIDE-based regimens vs TACE alone; exact median DoR values were not disclosed in the public ESMO GI 2026 / ASCO 2026 releases reviewed.
Regulatory Status
EMERALD-3 vs EMERALD-1: What KOLs Are Debating
EMERALD-3 is the first Phase III trial to support a STRIDE-based, immunotherapy-plus-TACE approach in embolization-eligible HCC, meeting its primary PFS endpoint with improved ORR and DoR and an encouraging early OS trend. This stands in contrast to the companion trial EMERALD-1, where a confirmed PFS benefit for durvalumab (± bevacizumab) + TACE did NOT translate into an OS benefit at final analysis.
An emerging discussion point among HCC KOLs — clearly framed as hypothesis, not established fact — is that the timing of immunotherapy relative to embolization may matter. As Dr. Mark Yarchoan (Johns Hopkins) noted at #ESMOGI26, in EMERALD-3 immunotherapy was given before TACE (essentially neoadjuvant IO), whereas in EMERALD-1 IO came after TACE; he called the link "pure conjecture" but a potentially key difference. The ESMO GI discussant separately cautioned that PFS alone may not be a sufficient surrogate for OS in eeHCC, and that patient selection, early mortality, and post-TACE treatment sequencing all shape interpretation. The maturing EMERALD-3 OS data will be pivotal.

Physician Sentiment
About This Page
This profile aggregates verified physician commentary on EMERALD-3 from X (ASCO 2026 / #ESMOGI26) with primary-source clinical data. Every numeric claim is labelled with its source and data cut. KOL sentiment is derived from verbatim tweet text.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. All clinical figures are traceable to the labelled primary source and data cut. Last updated 2026-07-05.
EMERALD FAQ
What is the EMERALD-3 trial?
EMERALD-3 (NCT05301842) is an AstraZeneca Phase III, three-arm, randomized, open-label, sponsor-blinded trial of the STRIDE regimen (durvalumab [Imfinzi] plus a single priming dose of tremelimumab [Imjudo]) with or without lenvatinib, combined with transarterial chemoembolization (TACE), versus TACE alone in 760 patients with unresectable, embolization-eligible hepatocellular carcinoma.
Did EMERALD-3 meet its primary endpoint?
Yes. STRIDE + lenvatinib + TACE significantly improved progression-free survival versus TACE alone: median PFS 13.0 vs 9.8 months (HR 0.70; 95% CI 0.57–0.86; P=0.0007), a 30% reduction in the risk of progression or death, at the first data cutoff (2 Sep 2025). The STRIDE + TACE arm also improved PFS (12.9 vs 8.1 months; HR 0.71; 95% CI 0.56–0.91).
What were the ORR and overall survival results?
ORR by RECIST v1.1 (central review, DCO1 02-Sep-2025): 36.6% (STRIDE+lenvatinib+TACE) vs 30.0% (TACE alone). By mRECIST (central review, DCO1): 67.8% vs 54.8%; by mRECIST (investigator assessment, DCO1): 58.9% vs 42.5%. At the later DCO2 (Feb 2026): ORR 38.9% (STRIDE+lenvatinib+TACE) and 40.8% (STRIDE+TACE) vs 27.0% (TACE alone). (Erinjeri et al., ESMO GI 2026 Abstract LBA2, per OncoDaily congress coverage) Overall survival was an encouraging but immature interim signal: STRIDE + lenvatinib + TACE median 39.5 vs 34.7 months (HR 0.84; 95% CI 0.65–1.09; P=0.1814, not significant); STRIDE + TACE median not reached vs 32.9 months (HR 0.70; 95% CI 0.51–0.95; P=0.0233, nominal). Longer follow-up is awaited.
Is the EMERALD-3 STRIDE + TACE regimen FDA-approved?
No. As of July 2026 the STRIDE ± lenvatinib + TACE combination is investigational and not FDA-approved for embolization-eligible HCC. STRIDE (durvalumab + tremelimumab) is separately FDA-approved for unresectable HCC in the systemic setting (HIMALAYA), but that approval does not extend to the TACE-combination indication.
How does EMERALD-3 differ from EMERALD-1?
Both are AstraZeneca durvalumab + TACE trials in embolization-eligible HCC with contrasting readouts. EMERALD-1 (durvalumab ± bevacizumab, largely after TACE) confirmed a PFS benefit but missed OS at final analysis. EMERALD-3 (STRIDE ± lenvatinib, dosed before TACE) met its primary PFS endpoint with an encouraging early OS trend. KOLs including Dr. Mark Yarchoan have hypothesized that IO timing — neoadjuvant-style dosing before TACE in EMERALD-3 — may help explain the divergent survival signals, though this remains conjecture.