Resectable esophageal adenocarcinoma (cT1N+ or cT2-4a N0/+, M0) — University Hospital Schleswig-Holstein / German Research Foundation
Discover KOL Sentiment on ESOPEC →Design - Phase 3 perioperative FLOT chemotherapy vs neoadjuvant CROSS chemoradiotherapy, resectable esophageal adenocarcinoma (NCT02509286); primary endpoint overall survival.
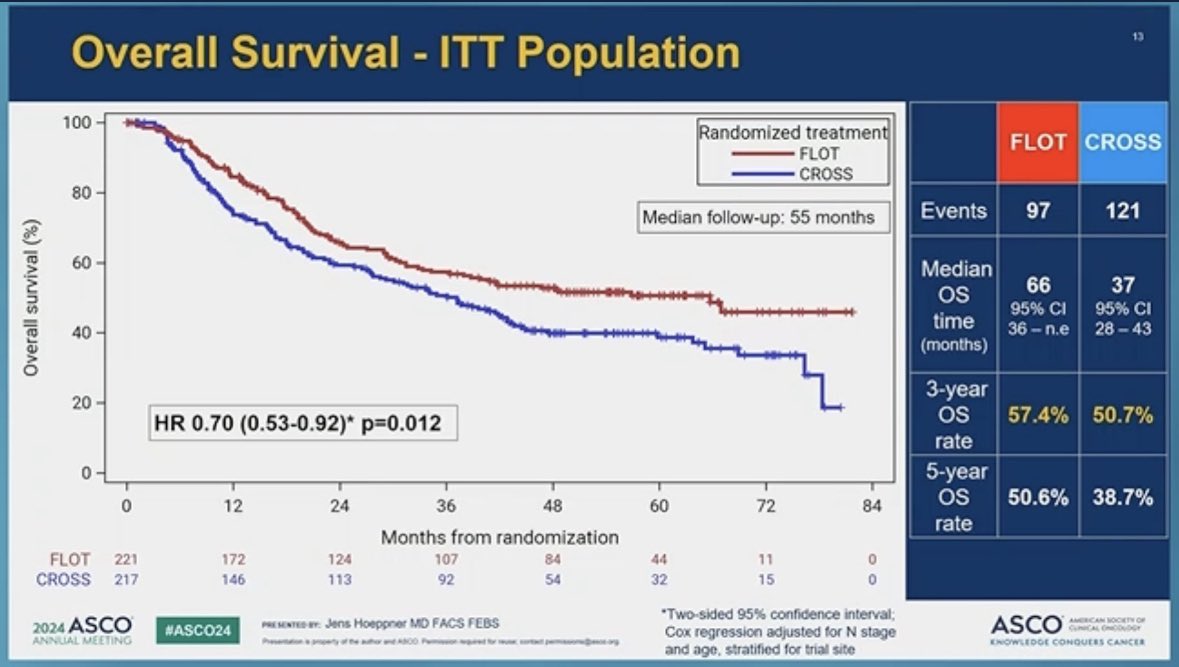
OS (primary, ITT) - Median 66 vs 37 mo, HR 0.70 (95% CI 0.53-0.92), P=0.01; 3-yr OS 57.4% vs 50.7%; 5-yr OS 50.6% vs 38.7% - a ~29-month median-OS improvement with FLOT.
Practice impact - First head-to-head Phase 3 comparison in pure esophageal adenocarcinoma; FLOT won on overall survival, and the trial established perioperative FLOT as the preferred standard over CROSS.
Safety - Grade >=3 AEs 58.0% (FLOT) vs 50.0% (CROSS); FLOT neutropenia 19.8%, diarrhea 6.8%; serious AEs 47.3% vs (CROSS) comparable.
Regulatory - Not a novel-drug FDA approval - both regimens use established agents; academic practice-changing (NEJM 2025).
Sponsor - University Hospital Schleswig-Holstein / German Research Foundation (academic).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.













Top tweets by impressions — click to view on X
🚨🚨🚨 #ESOPEC🚨🚨🚨
🔥Practice shifting trial🔥
Patients with resectable, locally advanced, esophagus/GEJ adenocarcinoma
Randomized
Peri-op FLOT (FLOT4)
vs
Pre-operative chemoradiation…
🚨ESOPEC Pub has landed!🚨
See data review below!
For now, "standard" will appropriately shift to peri-operative FLOT BUT we should not be satisfied as outcomes remain suboptimal
Ongoing ❓❓
- does…
OK, wait, something doesn't make sense with ESOPEC
Even excluding the presumably more radio-sensitive squams, why is the adeno arm performing worse in a contemporary trial vs. the CROSS study…
Isolated locoregional failures were halved w CROSS, but unsurprisingly many more distant metastases.
Also notable that CROSS group had many more distant mets even BEFORE start of therapy (11 vs. 1),…
Big dif in OS favoring FLOT over CROSS in ESOPEC!
Look forward to details & discussion in a few hours.
#ASCO24
https://t.co/csudkS1ZkP https://t.co/hC9oqG5Jq8
ESOPEC, a large randomized trial involving patients with resectable esophageal cancer, showed that perioperative chemotherapy improved overall survival as compared with preoperative…
❓Is CROSS out after ESOPEC?
Real-world CROSS outcomes from Nerherlands
@eClinicalMed
➡️4765 patients
✅87.5% completed full CROSS regimen
✅pCR: 20.5%
✅mOS: 33.7 mo, 3-year OS: 48.1%
❗️adjuvant…

ESOPEC trial
It’s been a long 15 year journey, but so nice to see Docetaxel triplets come on top for the benefit of our patients!
CROSS just doesn’t work for GEA-EAC- radiation compensates for poor…

#ASCO24 plenary, ESOPEC trial asked a very important clinically relevant question and answered it the right way. Kudos to the investigators but would have loved to see QOL and toxicity data as well.…
Out? No. Sicker/older non-FLOT candidates, non-surgical candidates, SCC, we still don’t know CM577 OS, ~50% of failures with FLOT are locoregional
Still a LOT of unmet need here! @NiuSanford…
ESOPEC is the first head-to-head Phase 3 comparison of perioperative FLOT vs. neoadjuvant CROSS in pure esophageal adenocarcinoma. FLOT won on OS, PFS, pCR, and 90-day post-op mortality. Investigators concluded FLOT should be preferred. Discussant noted CROSS may have underperformed vs. prior trials (mOS 37 months here vs. 43-50 months historically), but the study nonetheless settles the question. Post-neoadjuvant adjuvant nivolumab (CheckMate-577, non-pCR) and emerging organ-preservation concepts will reshape the landscape further. 5-year OS of 50% remains suboptimal — room for further improvement.
Median: 66 months (perioperative FLOT, 95% CI 36-NE) vs. 37 months (neoadjuvant CROSS chemoradiation, 95% CI 28-43). HR 0.7 (95% CI 0.53-0.92), P=0.01 3-year OS rate: 57.4% (FLOT) vs. 50.7% (CROSS). 5-year OS rate: 50.6% (FLOT) vs. 38.7% (CROSS). FLOT conveyed a 30% survival benefit over CROSS at median 55 months follow-up. Median OS 66 months (95% CI 36-NE) with perioperative FLOT vs. 37 months (95% CI 28-43) with neoadjuvant CROSS; HR 0.70 (95% CI 0.53-0.92, P=0.01). 3-year OS 57.4% vs. 50.7%; 5-year OS 50.6% vs. 38.7%. Per-protocol analysis: mOS NR vs. 39 months, HR 0.72 (P=0.023). Median PFS 38 vs. 16 months, HR 0.66 (P=0.001). pCR 16.8% (FLOT) vs. 10.0% (CROSS). Hoeppner et al., NEJM 2025;392(4):323-335.
Median: 66 months (FLOT) vs. 37 months (CROSS). HR 0.7 (95% CI 0.53-0.92), P=0.01 OS is the primary endpoint (see above). Practice-changing 29-month improvement in median OS.
Grade ≥3 adverse events: 58.0% (flot) vs. 50.0% (cross). Key AEs: neutropenia (19.8% FLOT), diarrhea (6.8% FLOT), leukopenia (6.3% FLOT; 9.7% CROSS), pneumonia (5.8% FLOT; 9.2% CROSS), pleural effusion (3.1% CROSS). Grade ≥3 AEs 58.0% (FLOT) vs. 50.0% (CROSS). Serious AEs 47.3% vs. 41.8%. 90-day postoperative mortality 3.1% (FLOT) vs. 5.6% (CROSS) — notably LOWER with FLOT despite higher preoperative AE burden. Completion rates: 87.3% (FLOT) vs. 67.7% (CROSS) received full neoadjuvant dosing.
✅ Practice-changing: perioperative FLOT is new SOC over CROSS for resectable esophageal adenocarcinoma. ESOPEC is the first head-to-head Phase 3 comparison of perioperative FLOT vs. neoadjuvant CROSS in pure esophageal adenocarcinoma. FLOT won on OS, PFS, pCR, and 90-day post-op mortality. Investigators concluded FLOT should be preferred. Discussant noted CROSS may have underperformed vs. prior trials (mOS 37 months here vs. 43-50 months historically), but the study nonetheless settles the question. Post-neoadjuvant adjuvant nivolumab (CheckMate-577, non-pCR) and emerging organ-preservation concepts will reshape the landscape further. 5-year OS of 50% remains suboptimal — room for further improvement.
ESOPEC is a Phase 3 randomized academic trial (NCT02509286, Germany) comparing perioperative FLOT chemotherapy (fluorouracil, leucovorin, oxaliplatin, docetaxel) with neoadjuvant CROSS chemoradiotherapy in patients with resectable esophageal adenocarcinoma (cT1N+ or cT2-4a, M0). Overall survival was the primary endpoint.
Perioperative FLOT significantly improved overall survival over neoadjuvant CROSS: median overall survival was 66 versus 37 months (HR 0.70; 95% CI 0.53-0.92; P=0.01), a roughly 29-month improvement. Three-year overall survival was 57.4% versus 50.7% and 5-year overall survival was 50.6% versus 38.7%, all favoring FLOT.
No. ESOPEC compares two established treatment regimens - perioperative FLOT chemotherapy versus neoadjuvant CROSS chemoradiotherapy - using drugs that are already established generics. It is a practice-defining academic trial (NEJM 2025) rather than a study leading to a new FDA drug approval.
Grade 3 or higher adverse events occurred in 58.0% of the FLOT arm versus 50.0% of the CROSS arm. Common grade 3 or higher events with FLOT included neutropenia (19.8%) and diarrhea (6.8%); CROSS showed events such as leukopenia and pneumonia. Serious adverse events were reported in about 47.3% of the FLOT arm, and both regimens were considered manageable.
ESOPEC is the first head-to-head Phase 3 comparison of perioperative FLOT versus neoadjuvant CROSS in pure esophageal adenocarcinoma. Because FLOT won on overall survival (as well as progression-free survival, pathologic complete response, and 90-day postoperative outcomes), it established perioperative FLOT as the preferred standard of care over CROSS chemoradiotherapy for this population.