MajesTEC-3 is a randomized phase 3 trial of teclistamab + daratumumab SC (Tec-Dara) versus daratumumab-based standard care (DPd/DVd) in relapsed/refractory myeloma. KOLs called it "unprecedented": median PFS was not reached vs 18.1 months (HR 0.17), and 36-month overall survival was 83% vs 65% (HR 0.46). The FDA approved Tec-Dara (Tecvayli + Darzalex Faspro, Johnson & Johnson) on March 5, 2026 for relapsed/refractory myeloma after at least one prior line.
Phase 3 · NCT05083169Teclistamab + DaratumumabRelapsed/Refractory MMPFS HR 0.17 · OS HR 0.46FDA Approved · Mar 5 2026
On March 5, 2026 the FDA approved teclistamab (Tecvayli) in combination with daratumumab and hyaluronidase-fihj (Darzalex Faspro) for adults with relapsed or refractory multiple myeloma who have received at least one prior line of therapy, including a proteasome inhibitor and an immunomodulatory agent — based on the MajesTEC-3 trial.
[Slide 1]
MajesTEC-3: PFS By Risk Status (ITT)
Tec-Dara
DPd/DVd
Events
Median
Events
Median
n/N
PFS (mo)
n/N
HR (95% CI)
PFS (mo)
Functional high risk
5/26
NE
14/20
23.2
0.22 (0.08-0.62)
Non-functional high risk
8/82
NE
57/94
20.8
0.11 (0.05-0.23)
Prespecified std. risk
15/126
NE
84/145
24.7
0.16 (0.09-0.27)
Prespecified high risk
20/104
NE
78/104
14.4
0.15 (0.09-0.25)
Expanded std. riskᵇ
5/52
NE
34/55
24.2
0.12 (0.04-0.30)
Expanded high riskᵇ
30/169
NE
122/180
15.8
0.18 (0.12-0.26)
1 HRCA
17/105
NE
69/111
17.9
0.19 (0.11-0.32)
≥2 HRCAs
13/64
NE
53/69
14.4
0.16 (0.08-0.29)
0.01
0.1
1
10
Tec-Dara better DPd/DVd better
Tec-Dara consistently improved PFS vs DPd/DVd regardless of disease biology
CI, confidence interval; HR hazard ratio; ITT. intent-to-treat; NE, not estimable; Std., standard "Prespecified standard risk: none of del(17p). 1(4;14), or 1(14;16). Prespecified high risk: >1 of del(17p). t(4;14). or t(14;16). Expanded
standard risk: none of del(17p). t(4;14). t(14;16), amp(1q21). or gain(1q21). Expanded high risk: >1 of del(17p). t(4;14). t(14;16). amp(1q21). or gain(1q21).
6
Presented by R Banenee at the 31st European Hematology Association (EHA) Annual Meeting: June 11-14. 2026: Stockholm. Sweden
---
[Slide 2]
MajesTEC-3: PFS by Prespecifieda Cytogenetic Risk
Estimated
100
36-mo PFS rate
87.4%
Tec-Dara, std. risk
% surviving without progression
80
Tec-Dara, high risk
77.7%
60
40
37.1%
DPd/DVd, std. risk
Std. risk: Tec-Dara, n=126; DPd/DVd, n=145
20
HR, 0.16 (95% CI, 0.09-0.27)
High risk: Tec-Dara, n=104; DPd/DVd, n=104
11.5%
DPd/DVd, high risk
HR, 0.15 (95% CI, 0.09-0.25)
0
4
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
45
48
Months
No. at risk
Tec-Dara, std. risk
126
116
108
105
105
104
103
102
101
99
97
64
36
17
6
0
0
DPd/DVd, std. risk
145
131
115
99
87
82
78
73
69
62
53
34
20
10
2
1
0
Tec-Dara, high risk
104
89
86
82
82
79
77
75
74
73
71
47
31
10
3
0
0
DPd/DVd. high risk
104
85
71
61
53
45
35
30
24
20
18
10
2
2
1
0
0
Tec-Dara demonstrated superior PFS vs DPd/DVd regardless of
cytogenetic risk and mirroring the overall study effect (HR 0.17)¹
"Prespecified standard risk: none of del(17p). t(4;14). or t(14;16). Prespecified high risk: 21 of del(17p). t(4;14). or t(14;16).
1. Costa LJ, et al. N Engl J Med. 2026,394(8):739-752.
7
Presented by R Banerjee at the 31st European Hematology Association (EHA) Annual Meeting: June 11-14, 2026; Stockholm, Sweden
---
[Slide 3]
MajesTEC-3: MRD-Negative ≥CR by Prespecified
Cytogenetic Risk
MRD-negative ≥CRᵃ (10⁻⁵)
MRD-negative ≥CRᵃ (10⁻⁶)
Tec-Dara
100
100
DPd/DVd
90
OR, 5.08
90
(95% CI, 2.90-8.88)
OR, 12.83
OR, 8.29
80
80
(95% CI, 4.46-15.42)
OR, 21.28
(95% CI, 5.77-28.53)
(95% CI, 7.93-57.14)
MRD-negative ≥CR rate, %
70
62.6
70
57.9
58.9
60
60
54.7
50
50
40
40
30
24.8
30
20
20
14.7
9.7
10
10
5.4
0
0
n=107
n=129
n=95
n=93
n=107
n=129
n=95
n=93
Prespecified std. riskb
Prespecified high riskc
Prespecified std. riskb
Prespecified high riskc
Tec-Dara substantially increased MRD-negative ≥CR rates,
with an MRD-negative ≥CR (10⁻⁶) rate that was 10-fold that of DPd/DVd
OR, odds ratio. "MRD-negative >CR refers to MRD negativity achieved within 3 months prior to achieving CR/sCR or at any time after CR/sCR and before progression or subsequent therapy. Assessed in the MRD NGS primary
analysis set, defined as all randomized patients except those recruited in China (due to China instead utilizing NGF for MRD assessment). Prespecified standard risk: none of del(17p). 1(4;14), or 1(14;16). Prespecified high risk: 21
of del(17p), 1(4;14), or t(14;16).
8
Presented by R Banerjee at the 31st European Hematology Association (EHA) Annual Meeting: June 11-14, 2026; Stockholm, Sweden
---
[Slide 4]
MajesTEC-3: MRD-Negative ≥CR by
Functional High-Risk Statusᵃ
MRD-negative ≥CRb (10⁻⁵)
MRD-negative ≥CRb (10⁻⁶)
Tec-Dara
DPd/DVd
100
100
90
OR, 4.47
90
OR, 5.95
80
(95% CI, 2.32-8.60)
OR, 12.75
80
(95% CI, 2.98-11.88)
(95% CI, 1.42-114.40)
MRD-negative ≥CR rate, %
70
70
61.3
58.8
OR, NE
60
60
(95% CI, NE-NE)
50
42.9
50
38.1
40
40
30
26.1
30
19.3
20
20
10
5.6
10
0
0
0
n=80
n=88
n=21
n=18
n=80
n=88
n=21
n=18
Not FHR after 1 prior LOT
FHR after 1 prior LOT
Not FHR after 1 prior LOT
FHR after 1 prior LOT
Tec-Dara consistently increased MRD-negative >CR rates vs DPd/DVd at both 10⁻⁵ and
the more stringent 10⁻⁶ threshold in patients with FHR MM
Functional high-risk status defined as patients with 1 prior LOT and progressive disease within 18 months of ASCT or start of initial therapy. MRD-negative >CR refers to MRD negativity achieved within 3 months prior to achieving
CR/sCR or at any time after CR/sCR and before progression or subsequent therapy. Assessed in the MRD NGS primary analysis set, defined as all randomized patients except those recruited in China (due to China instead utilizing
NGF for MRD assessment).
14
Presented by R Banerjee at the 31st European Hematology Association (EHA) Annual Meeting: June 11-14, 2026; Stockholm, Sweden
[Slide 1]
Teclistamab (RRMM): (Pts) With Relapsed Ratumumab
and Rahul on Cytogenetic
- Raphael Jin Lu," Banerjee, Charlotte 12 Niels WCJ Hamza Carson, " van de Hashmi, Agata Meletios . Donk? Caeiro, Weill Tyczynska, Roberto to Sun, Larry A 12 Dimopoulos, Alain 4: D Mina,' Kentos, Anderson 2 Markus Maria 19,20 Vania Hansson, Jr, Elena Victoria Hungria, Zamagni, a Mateos, Mark % na Anna Grey, Nizar Satosh K Surbhi Bahlis, Yoshihara, Charlotte Aurone # Kihyun Toftmann Perrot! Kim, Ajay Hansen, K Nooka,
Institute, Consejo Fred Hulchinson Superior Emoy University Cancer de Conter, Adanta Vieyra, Sextle GA " USA Lijuan University Kang, of Hongmel Kristen Xu, Lantz, Ricardo " Anne Claudio Attar, Seifert, . Cerchione. Deborah * Salomon Briseno- Sidana, Manier Toomey, Paula * Jesis Rodriguez Paul Geerts,
a
Service Cirical Athers, SA, Medizinsche Cárdiba, Research d'Hematologie, School Argentina Kink of Center ACT for Hematologic Oncopole Certificate). Johnan Disease, Principal Toubute CBERONG Being France Ching Salamance Beigun Emay Washington, The Salamance Royal Spain Seate Ane Writing M de Cancer inestigición American Cance Haria University Christopher Medical " Chiu, Caigary Luciano Costa's Lina Otaro, . Case
i
I
I
/
/
1
Göleborg Mediche Titala Cancer Scan Center Chirurgiche, Sweden Clinica Zeole Medicine The University The Athers, Nethertands, Bologra, Greece: to *2. *You Bologra, talk Car Bladipod styoge "Chica Kore, Neueger, Certano, The Natinomya, that Dresdien, Demany PRIN Copentages, Carata Terrary
RCCS,
Cancer
Medicale,
Center,
New
Spain
True,
*
taly,
NY,
Badges
law
Center, Johnson Presented & Johnson, by TN R Ratan Banerjee "Johnson Lie, & France, PA "Cancer Dine Certer University Katara de CIMA, in Into
at the 31st European Hematology Association (EHA) Annual Meeting: June No. 11-14, 2028; - Stockhaim, Sweden
---
[Slide 2]
Rahul
Banerjee
EHA2026
Congress
eha
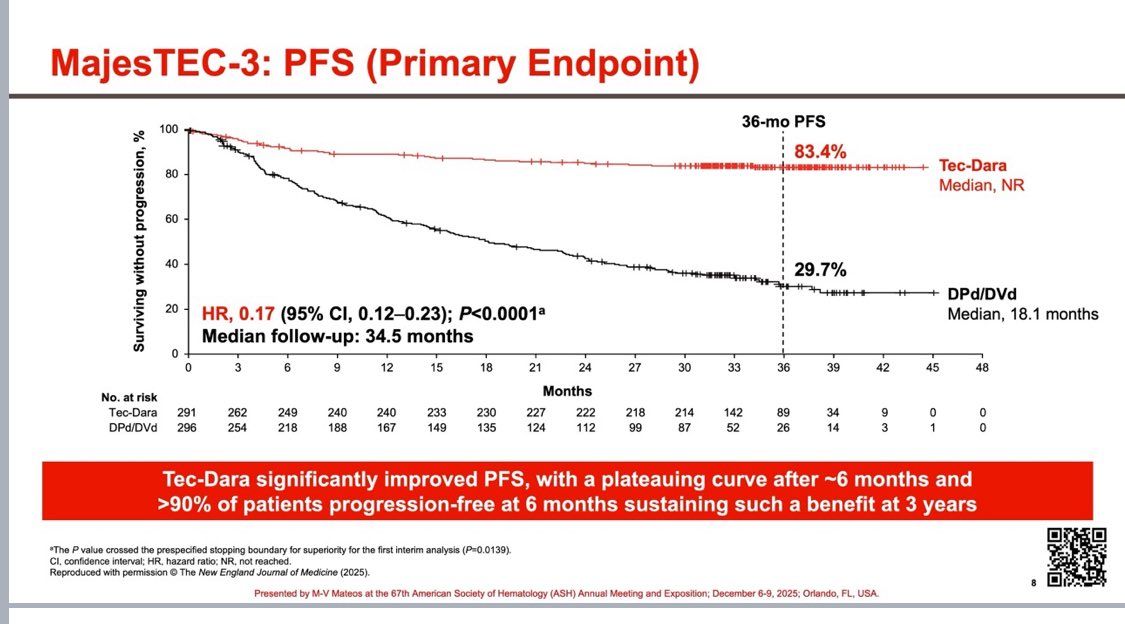
Median PFS was not reached with Tec-Dara versus 18.1 months with daratumumab-based standard care — a hazard ratio of 0.17 (95% CI 0.12–0.23, P<0.0001), an 83% reduction in the risk of progression or death at nearly three years of follow-up (3-year PFS 83.4% vs 29.7%). Depth of response strongly favored Tec-Dara (≥CR 81.8% vs ~32%; higher MRD-negativity) in this 587-patient randomized trial.
At 36 months, overall survival was 83.3% with Tec-Dara versus 65.0% with standard care — HR 0.46 (95% CI 0.32–0.65, P<0.0001), a 54% reduction in the risk of death.
The PFS benefit was consistent across cytogenetic risk: HR 0.16 with ≥2 high-risk cytogenetic abnormalities (HRCAs), 0.19 with 1 HRCA, and 0.15 in the prespecified high-risk group. Estimated 36-month PFS reached ~87% (standard risk) and ~78% (high risk) with Tec-Dara.
As a BCMA-directed bispecific combination, infection risk is the central safety consideration. KOLs emphasize close monitoring, routine monthly IVIG, and infection-prevention measures. MajesTEC-3 used a less-frequent, daratumumab-like teclistamab dosing schedule with subcutaneous administration. Cytokine release syndrome occurred in ~60% of patients but was limited to grades 1–2 and resolved.
A randomized phase 3 trial of teclistamab + daratumumab SC (Tec-Dara) vs daratumumab-based standard care (DPd or DVd) in relapsed/refractory myeloma after 1–3 prior lines, presented at ASH 2025 (LBA-6) and published in the NEJM.
What were the results?
Median PFS not reached vs 18.1 mo (HR 0.17, 95% CI 0.12–0.23, P<0.0001); 36-month OS 83.3% vs 65.0% (HR 0.46).
Is Tec-Dara FDA approved?
Yes. On March 5, 2026 the FDA approved teclistamab + daratumumab hyaluronidase-fihj (Tecvayli + Darzalex Faspro) for relapsed/refractory multiple myeloma after at least one prior line of therapy, based on MajesTEC-3.
What is the main safety concern?
Infection risk; KOLs emphasize close monitoring, routine monthly IVIG, and infection prevention.
Why does it matter?
KOLs called the benefit "unprecedented" and noted it could shift first-relapse standard of care from monotherapy to a bispecific-based combination as early as second line.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. KOL quotes verbatim from public posts; impressions/sentiment from the KOL Pulse database. Efficacy figures verified against ASH 2025 LBA-6, NEJM, and the J&J press release. Last updated June 2026.