Definitively unresectable, BRAF wild-type colorectal cancer with liver-only metastases — Assistance Publique - Hôpitaux de Paris / French National Cancer Institute
Discover KOL Sentiment on TRANSMET →Design - Phase 3 liver transplantation + chemotherapy vs chemotherapy alone, definitively unresectable BRAF wild-type colorectal cancer with liver-only metastases (NCT02597348); primary 5-year overall survival.
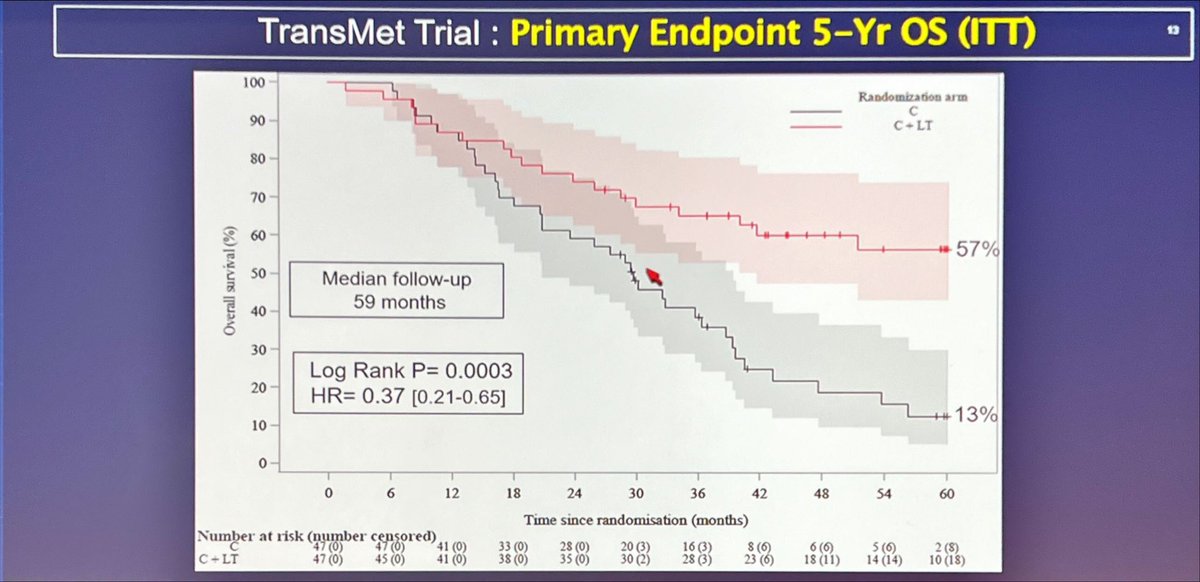
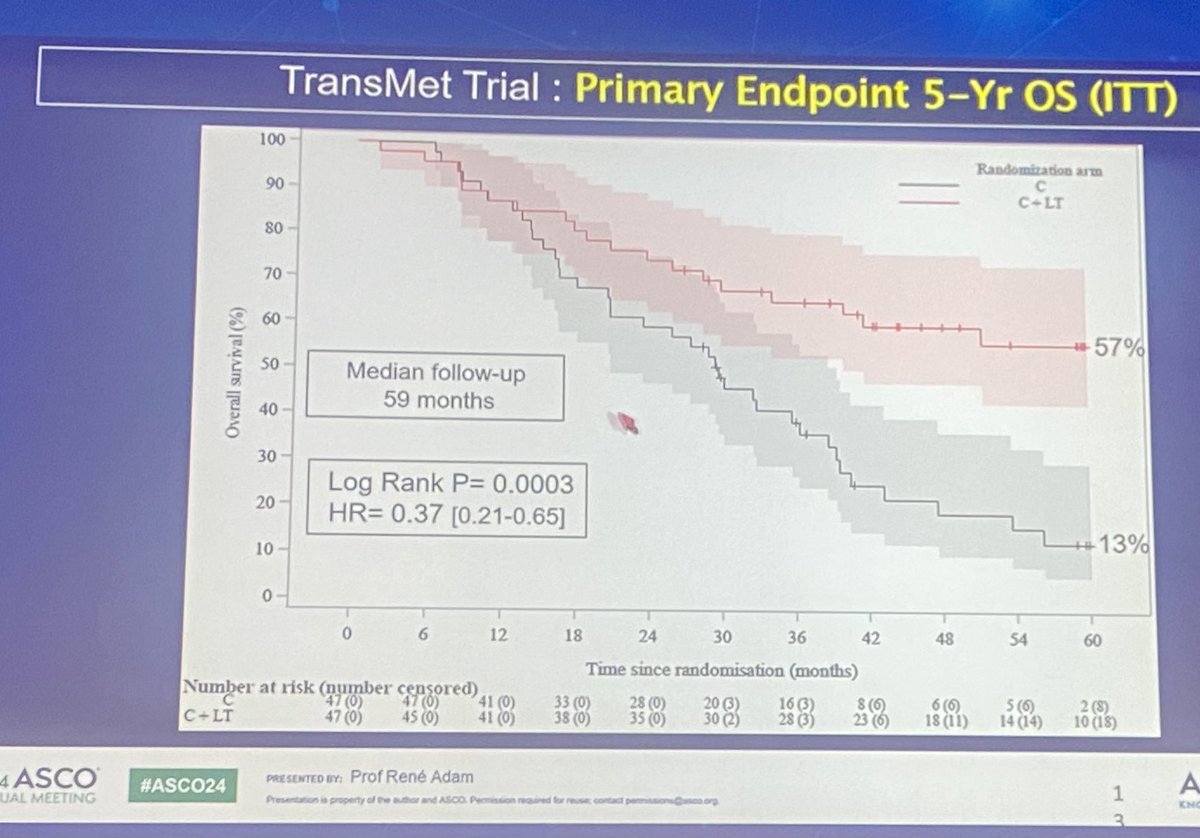
5-yr OS (primary, ITT N=94) - 56.6% (transplant + chemo) vs 12.6% (chemo alone); median not reached vs 29.7 mo; HR 0.37 (95% CI 0.21-0.65), P=0.0003.
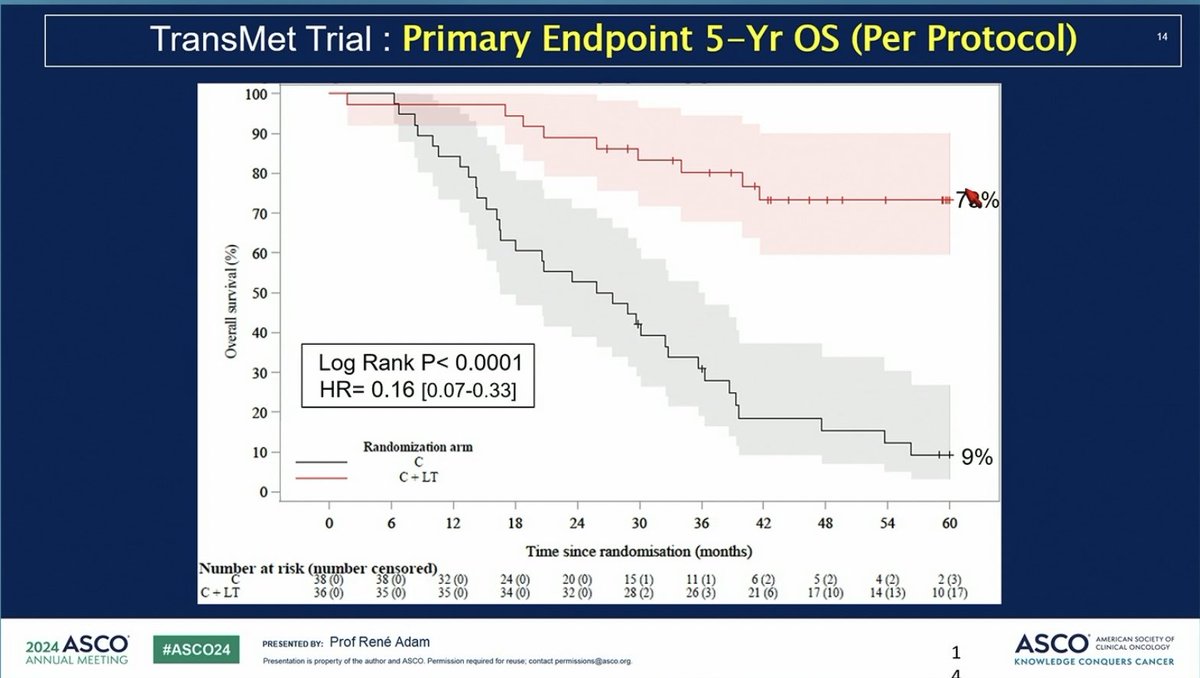
5-yr OS (per-protocol) - 73.3% (transplant + chemo) vs 9.3% (chemo alone) - a roughly 4-fold improvement in highly selected patients.
Safety - Transplant-specific risks (graft rejection, infection, secondary malignancy) and immunosuppression complications; tailored post-transplant immunosuppression + postoperative chemotherapy (not fully quantified in summary sources).
Regulatory - Not an FDA drug approval - a surgical/transplant strategy; practice-influencing per Lancet 2024 for highly selected patients.
Sponsor - AP-HP / French National Cancer Institute (academic).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.
















Top tweets by impressions — click to view on X
CTx & liver transplantatison vs CTx in pts with unresectable CRC liver metastases at #ASCO24
🔎prospective trial TRANSMET, 94 pts
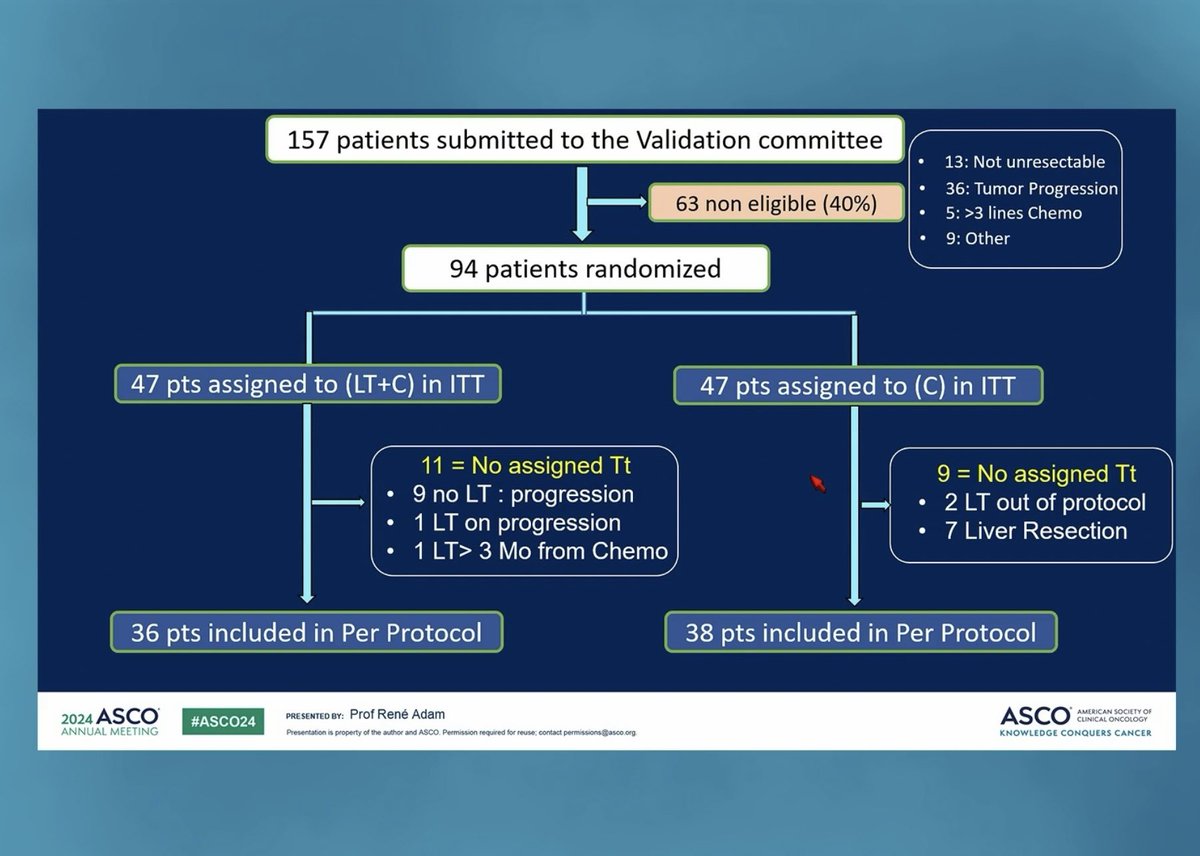
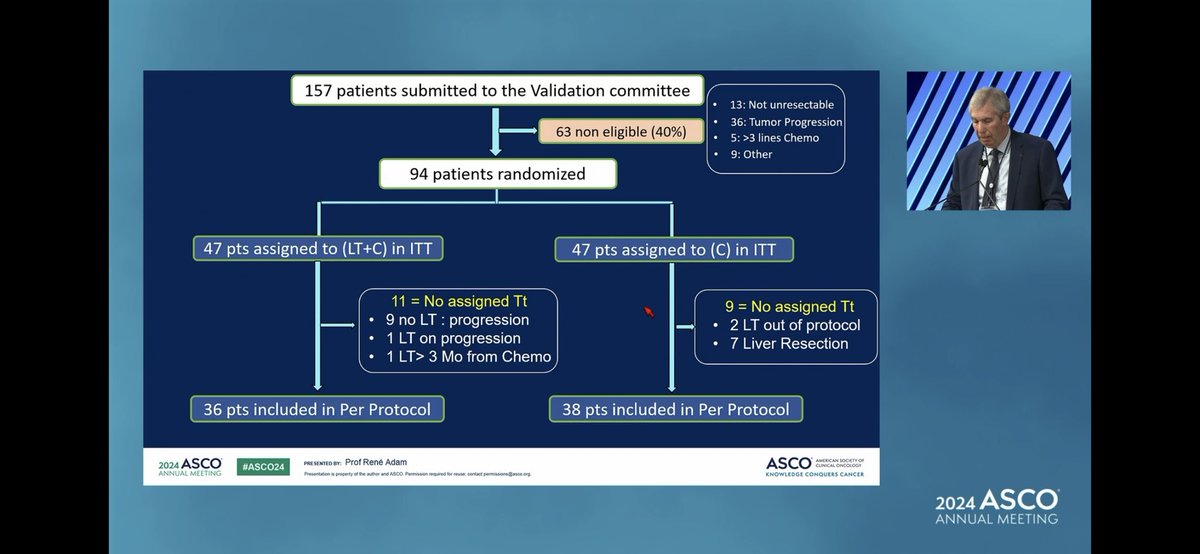
👉40% excluded, 9 drop out, 81% underwent LTx
👉mPFS 17.4 vs 6.4,…
ESMO GI 2024 take-home messages: Colorectal cancer
#ESMOGI24
👉more options: Liver transplantation (TRANSMET), ICI combos (Nivo/Ipi; Botensilimab/Basiliximab..), sequential therapy, molecular…
TRANSMET: CT+liver transplant vs CT alone in pts with
unresectable CRC liver mets
- 94 pts
- 5-year OS in ITT: 57% in CT+LT vs 13% in CT arm (HR 0.37,p=0.0003)
- 74% of transplanted pts had…
1:2 - Transmet trial presented at @ASCO #ASCO24. Is this the new standard for unresectable colorectal liver metastases?
What do people think? @kharofaJ @shimulshah73 @DavendraSohal @IHPBA…
Issues with Transmet Trial.
1- The chemotherapy alone arm did not get any Locoregional therapy ( surgery or Ablation) , even in responding patients.
That's not what we do in real world .
2 -…
TRANSMET: addition of liver transplant to chemo in CRC with unresectable liver mets: big OS benefit (5 yr 57% v 13%).
Curve plateauing at 5 years suggests ~1/2 pts can be cured!
Challenge is liver…

TransMet #ASCO24 game-changer
➡️definitively unresectable CRC LM
➡️chemo vs chemo &transplant
➡️heavily pre treated
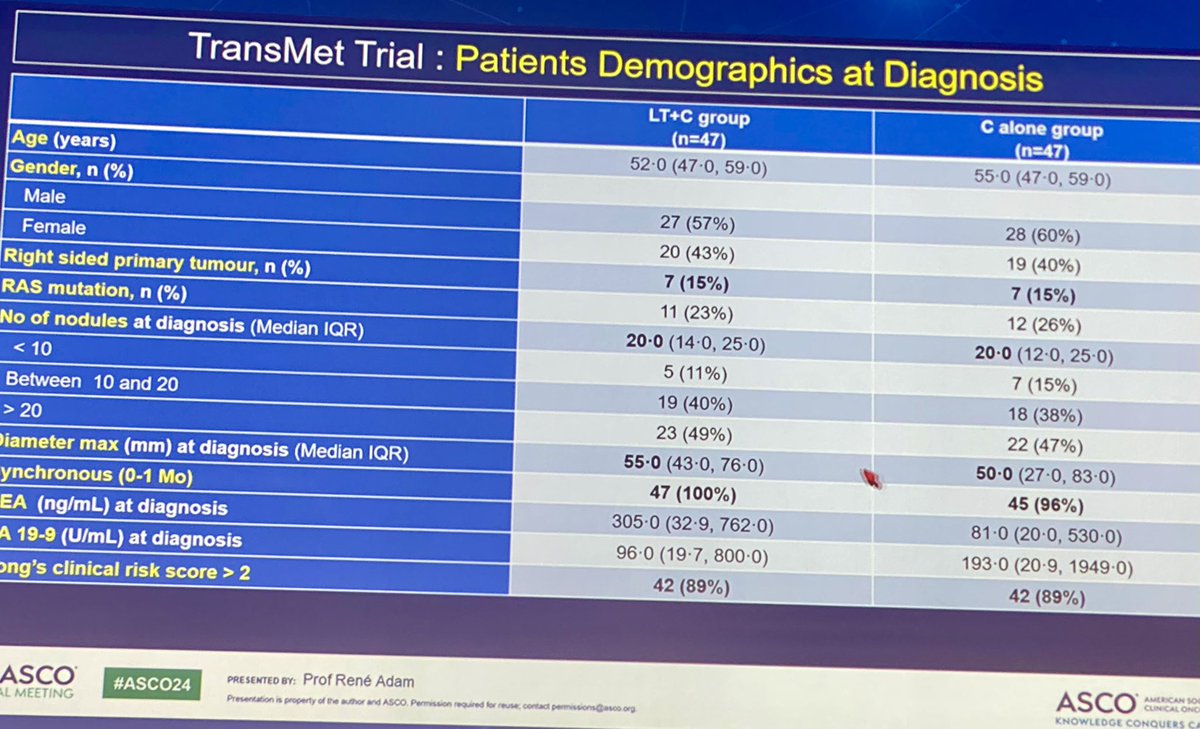
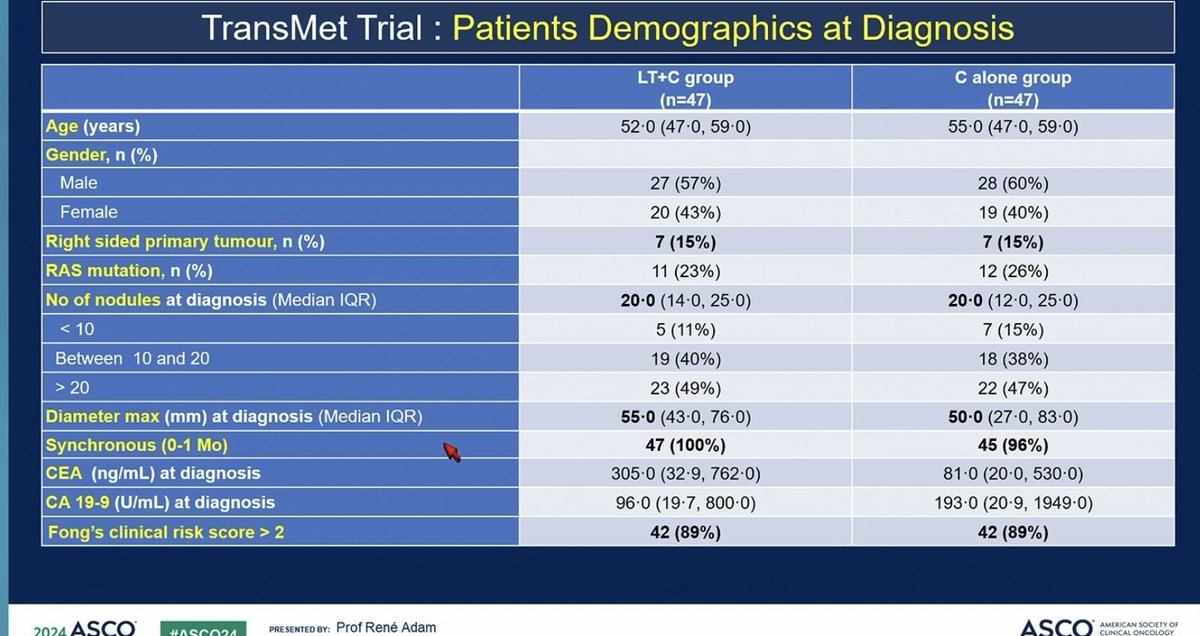
➡️highly selected 👇🏻note %RASWT and left sided
➡️v impressive 5 yr OS 57 v13%…

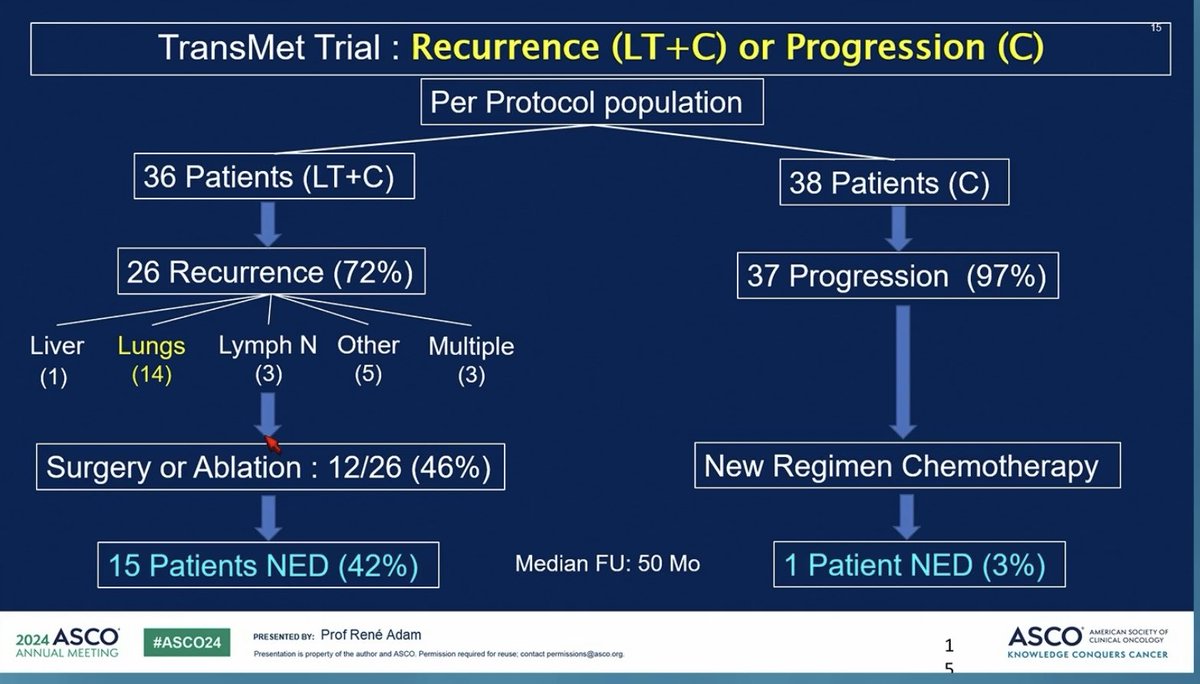
#ASCO24: Dr Rene Adam TransMET showed major OS benefit, HR =0.16 of #livertransplant in liver unresectable #CRC. Recurrences mostly ex-liver and treated in transplant arm. @OncoAlert…
Invited discussant of TRANSMET
by @ChiaraCrem1 #ESMOGI24
😅more then "practice-changing"? "mind-changing"?
❓How to implement in clinical practice
#ESMOAmbassadors @myESMO https://t.co/cY6hcZVcId

#ASCO24 @ASCO #CRCsm
TRANSMET - Chemo +/- OLTx in unresectable liver metastases, OS Dr Rene Adam 🇫🇷
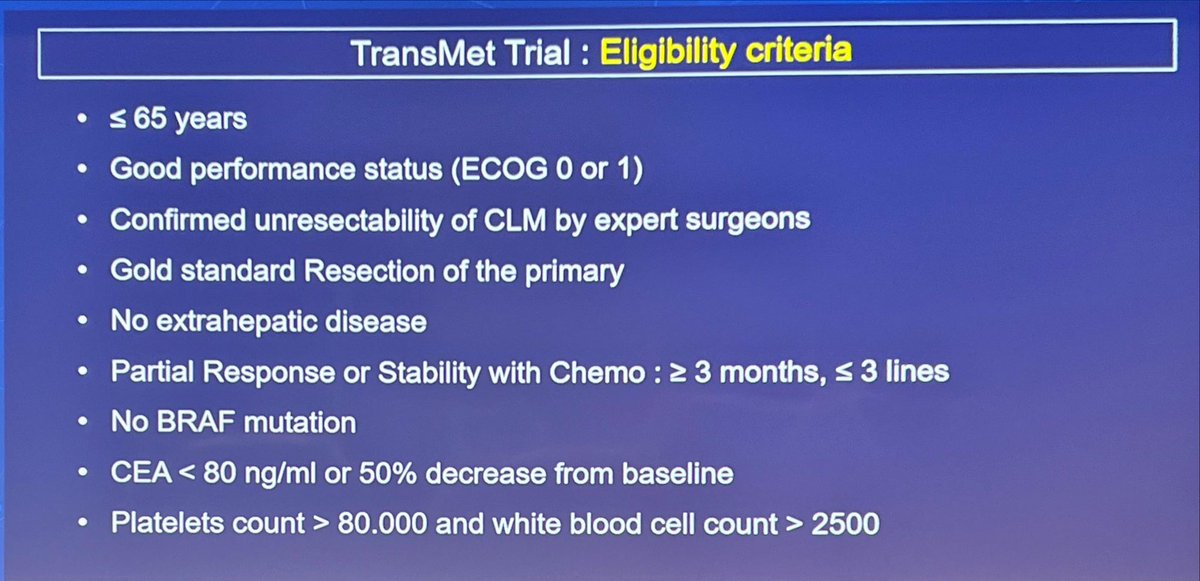
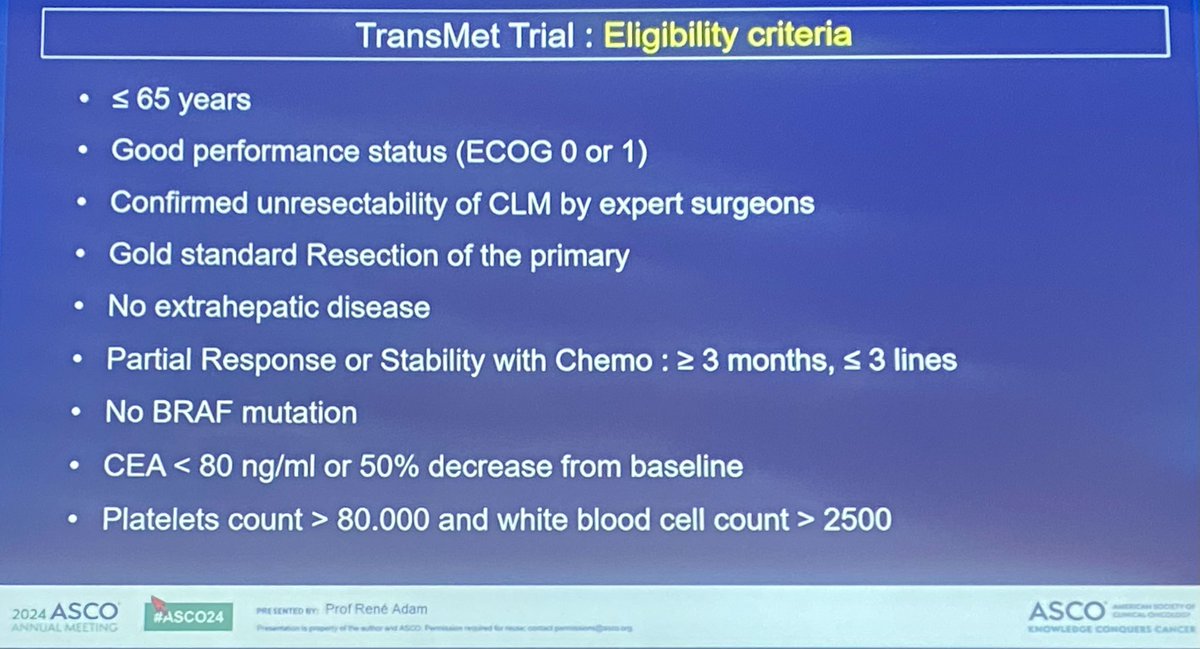
📌<65y, no BRAFmut, CEA <80
📌 n=94, 15% R-sided, median 20 tumours, 60% 3+L of chemo. 36/47…
TRANSMET demonstrates a 4-fold 5-year OS improvement (ITT 57% vs. 13%) with liver transplant + chemo vs. chemo alone in a highly selected patient population: BRAF wild-type, liver-only metastases, resected primary, ≤3 chemo lines, response to chemo, absence of extrahepatic disease, age 18-65. Only a very small fraction of mCRC patients will be eligible. Practical hurdles: donor organ scarcity, expert selection panels, access to transplant centers, prioritization ethics vs. other cancer/non-cancer LT indications. Living donor LT is discussed but has separate ethical concerns. Paradigm-shifting data nonetheless.
Median: not reached (liver transplantation + chemo) vs. 29.7 months (chemotherapy alone). HR 0.37 (95% CI 0.21-0.65), P=0.0003 5-year OS (ITT) rate: 56.6% (LT+chemo) vs. 12.6% (chemo). 5-year OS (per-protocol) rate: 73.3% (LT+chemo) vs. 9.3% (chemo). ITT analysis (N=94): 5-year OS 56.6% (95% CI 43.2-74.1) with LT+chemo vs. 12.6% (95% CI 5.2-30.1) with chemo alone; HR 0.37 (95% CI 0.21-0.65, P=0.0003). Per-protocol (N=74; excludes 11 LT and 9 chemo patients who did not receive assigned treatment): 5-year OS 73.3% vs. 9.3%; HR 0.16 (95% CI 0.07-0.33, P<0.0001). Median OS not reached (LT+chemo) vs. 29.7 months (chemo ITT) or 26.6 months (chemo PP). Median PFS 17.4 vs. 6.4 months, HR 0.34 (95% CI 0.20-0.58, P<0.0001). Median follow-up 59.3 months. 28 (74%) of LT patients had recurrence; 13 (46%) treated with surgery/ablation; 15 of 38 LT patients ultimately disease-free. Adam et al., Lancet 2024;404:1107-1118.
HR 0.37 (95% CI 0.21-0.65), P=0.0003 5-year OS is the primary endpoint (see above). Practice-changing 4-fold improvement in 5-year survival in highly selected patients.
Grade ≥3 TRAE rates, transplant-specific AEs (graft rejection, infection, secondary malignancy), and immunosuppression-related complications not quantified in available summary sources. Patients received tailored post-LT immunosuppression and postoperative chemotherapy.
✅ Practice-changing: liver transplantation is new standard for highly selected permanently unresectable CRC liver-only metastases. TRANSMET demonstrates a 4-fold 5-year OS improvement (ITT 57% vs. 13%) with liver transplant + chemo vs. chemo alone in a highly selected patient population: BRAF wild-type, liver-only metastases, resected primary, ≤3 chemo lines, response to chemo, absence of extrahepatic disease, age 18-65. Only a very small fraction of mCRC patients will be eligible. Practical hurdles: donor organ scarcity, expert selection panels, access to transplant centers, prioritization ethics vs. other cancer/non-cancer LT indications. Living donor LT is discussed but has separate ethical concerns. Paradigm-shifting data nonetheless.
TRANSMET is a Phase 3 randomized academic trial (NCT02597348, France) of liver transplantation plus chemotherapy versus chemotherapy alone in patients with definitively unresectable, BRAF wild-type colorectal cancer confined to the liver (liver-only metastases). Five-year overall survival was the primary endpoint. This is the colorectal-cancer TRANSMET liver-transplant trial, not a drug study.
TRANSMET showed a dramatic survival benefit in a highly selected population. In the intent-to-treat analysis (N=94), 5-year overall survival was 56.6% with liver transplantation plus chemotherapy versus 12.6% with chemotherapy alone (median not reached versus 29.7 months; HR 0.37; 95% CI 0.21-0.65; P=0.0003). In the per-protocol analysis, 5-year overall survival was 73.3% versus 9.3% - roughly a 4-fold improvement.
TRANSMET does not correspond to an FDA drug approval, because the intervention is liver transplantation - a surgical procedure - combined with standard chemotherapy, not a new drug. The Lancet 2024 results have influenced practice for carefully selected patients, but eligibility depends on strict selection criteria and transplant-program resources rather than a regulatory drug label.
Candidates are a highly selected group: patients with definitively unresectable colorectal liver metastases that are confined to the liver (no extrahepatic disease), with BRAF wild-type tumors, and with disease control on systemic chemotherapy. Rigorous selection is essential, and the approach requires a liver-transplant program with appropriate immunosuppression and follow-up.
The approach carries transplant-specific risks including graft rejection, infection, and immunosuppression-related complications, as well as a potential for secondary malignancy. The striking survival benefit applies to a highly selected population, and the difference between the intent-to-treat (56.6%) and per-protocol (73.3%) 5-year survival underscores how patient selection and completing transplantation drive the outcome.